IMMUNOLOGY OF TRANSPLANTATION Prof fawzia aboali Ainshams faculty


IMMUNOLOGY OF TRANSPLANTATION Prof. fawzia aboali Ainshams faculty of medicine
are put into another person's")
Organ Transplantation Organs or tissues from one human being(the donor)are put into another person's body (the recipient). Ø In 1959, Joseph Murray and his colleagues in Boston successfully transplanted a Kidney that were donated by fraternal twins and it functioned for 20 years without immunosuppression drugs. Ø First successful Liver transplant- on 7/23/1967 Ø First successful Heart transplant- In Cape Town, South Africa on 1/2/68 Ø First successful Bone Marrow transplant- on 8/25/68

Ch. 17

Why Is it Difficult? n n Organ transplantation is difficult because of the HLA antigens located on the cell surface. Human Leukocyte Antigen (HLA) also referred to as Major Histocompatibility Complex (MHC) plays a role in intercellular recognition and discrimination between self and non-self.
 HLA antigen typing, 2) screening of the")
Histocompatibility test consists of three tests: 1) HLA antigen typing, 2) screening of the recipient for the anti. HLA antibodies 3) the lymphocyte crossmatch or compatability test.
 ØIs located on short arm of chromosome 6 ØIt includes")
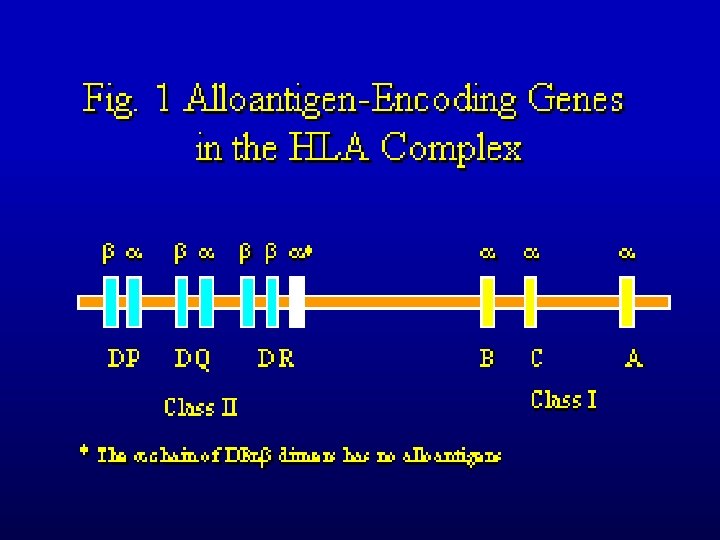
MAJOR HISTOCOMPATIBILITY COMPLEX (MHC) ØIs located on short arm of chromosome 6 ØIt includes 3 regions: n n class Ia , class Ib , class II and class III Ø They are targets for rejection Ø They are inherited from both parents as MHC

Different HLA Alleles n n Class I- HLA A HLA B HLA C 451 alleles 782 alleles 238 alleles Class II- HLA DR HLA DQ HLA DP HLA DM HLA DO 525 alleles 105 alleles 147 alleles 11 alleles 21 alleles

Requirements for Transplant n Each transplant center has different requirements for allele matches. In order to find a match, doctors require that at least a minimum of 3 allele matches. HLA-A, HLA-B and HLADRB 1. One set of the three antigens are inherited from your mother and the other set is inherited from your father. This makes 6 antigens to match

Requirements for Transplant

Chance of a Match n n Mother/Father: 25% chance of full match One Sibling: 25 % chance of full match Two Siblings: 44 % chance of full match Three siblings: 58% chance of full match
 – in the same individual: from one site")
TYPES OF GRAFTS Autologous graft (autograft) – in the same individual: from one site to another one Isogenic (isograft) – between genetically identical individuals Allogeneic (allograft or homograft) – between different members of the same species Xenogeneic (xenograft) – between mmbers of different species

Clinical Types of Rejection Hyperacute- within 24 hours graft is never vascularized preexisting antibodies (complement) Crossmatching to prevent this Acute- within a few weeks TH cell activation Chronic- a long time later humoral and cell-mediated an intractable problem

Ch. 17

Mechanisms of graft rejection qdisparity of genetic background between donor and recipient q. Sensitization q. Dendritic cells in graft may act as APCs q. Host effector cells can migrate q. Donor cells can migrate to periphery and present graft antigens there q. Other cells may act as APCs

VARIABLES DETERMINING TRANSPLANT OUTCOME Donor-host antigenic disparity Strength of host anti donor response Immunosuppressive regimen The condition of the allograft Primary disease of the host

PATHOGENESIS OF CHRONIC REJECTION Is the result of organ damage by immunologic and non-immunologic factors Initially – the minor damage and activation of endothelium by cytotoxic T cells and antibodies

PATHOGENESIS OF CHRONIC REJECTION -2 § Production by endothelial cells biologically active mediators (PDGF, PAF, TNF, thromboxans etc. ) § Secretion of cytokines by infiltrating lymphocytes § Mitogenic effect on myocytes and fibroblasts results in cell proliferation and fibrosis

CHRONIC REJECTION IS MORE FREQUENT WHEN: Were previous episodes of acute rejection There is a low number of compatible HLA antigens with recipient Patient on inadequate immunosuppression >>>

CHRONIC REJECTION IS MORE FREQUENT WHEN: <<< In the case of cytomegaly virus infection The period of organ storage was too long Patient is heavy smoker and/or is hyperlipidemic Organ mass is unproportionally small as compared to body mass

Ch. 17

Graft Rejection Is Mediated By T Cells

Immunosuppressive therapy ØMost drugs are nonspecific ØOther rapidly-dividing cells are affected (epithelial cells, bone marrow cells) ØMitotic inhibitors- azothiaprine, methotrexate ØCorticosteroids- anti-inflammatory
, Tacrolimus (FK-506) – inhibit IL-2 production by T")
MODERN IMMUNOSUPPRESSIVE THERAPY Cyclosporin (Cs. A), Tacrolimus (FK-506) – inhibit IL-2 production by T cells Sirolimus (rapamycin) – inhibits signals transmitted by IL-2 binding to IL-2 R (antiproliferating effect) Azathioprine – reduces numbers and function both, T and B cells.
 – inhibits DNA synthesis and protein glycosylation")
MODERN IMMUNOSUPPRESSIVE THERAPY -2 Mycophenolate mofetil (MMF) – inhibits DNA synthesis and protein glycosylation Anti-IL-2 monoclonal antibodies FTY 720 – dramatic effect on lymphocyte migration
 Is common complication in recipients of bone marrow transplants")
GRAFT VERSUS HOST DISEASE (GVH) Is common complication in recipients of bone marrow transplants Is due to the presence of alloreactive T cells in the graft It results in severe tissue damage, particularly to the skin and intestine
 It may be avoided by careful typing, removal of")
GRAFT VERSUS HOST DISEASE (GVH) It may be avoided by careful typing, removal of mature T cells from the graft and by immunosuppressive drugs It is manifested by marked rise of several cytokines in patient’s serum (IFN- , TNF, IL-1, IL-2, IL-4)

RISK FACTORS IN FORMATION OF GVH Acute GVH Previous pregnancies in female donor High T cell number in marrow HLA disparity Transplant from female to male Low immunosuppression Herpes virus infection Chronic GVH Aging of donor and recipient Donor’s leukocyte transfusion Previous acute GVH High dosage radiation Transplant from female to man HLA disparity

Why is the fetus not rejected? “Protected” site Local immunosuppression §uterine epithelium and trophoblast* secrete cytokines that suppresses TH 1 §placenta secretes a substance that depletes tryptophan: T cell starvation? §tolerance of paternal MHC antigens? §Outer layer of placenta; does not express MHC Class I and Class II antigens

- Slides: 31