Immnopathology lec 3 By Dr Mays Ibrahim Rejection

Immnopathology lec 3 By Dr. Mays Ibrahim

Rejection of Tissue Transplants � Allografts transplantation of organs from one individual to another of the same species. � Rejection is a complex phenomenon involving both cell- and antibody-mediated reactions that destroy the graft. � Immune Recognition of Allografts Rejection of allografts is a response mainly to MHC molecules.

Host T cells recognize allograft HLA by two pathways—direct and indirect: � Direct pathway: Host T cells recognize donor HLA on APC derived from the donor; the most important cells in this process are donor dendritic cells. Host CD 8 T cells recognize donor class I HLA molecules and mature into CTL; host CD 4 T cells recognize donor class II HLA molecules; they proliferate and differentiate to form TH 1 (and possibly TH 17) effector cell populations. Indirect pathway: Host T cells recognize donor HLA after processing and presentation on host APC (analogous to any other exogenous processed antigen). The principal response is therefore a DTH mediated by CD 4 T lymphocytes.

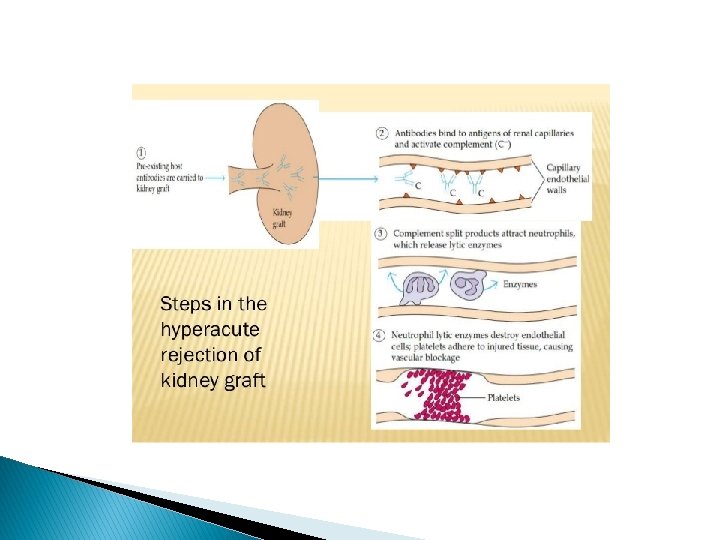
Types � � Hyperacute Rejection Occurs when the recipient has been previously sensitized to graft antigens (e. g. , by blood transfusion or pregnancy). Mediated by preformed antibodied Occur immediately after transplantation (minutes to days) Acute Rejection Typically occurs within days or months of transplantation or after cessation of immunosuppressive therapy. Both cellular and humoral mechanisms can contribute. Gradual onset of oliguria and azotemia. Treated with increase immunosuppressive dose Chronic rejection occurs over months to years gradual onset of oliguria, hypertension and azotemia Micro: arteries show dense obliterative intimal fibrosis, causing allograft ischemia. Poor response to treatment
 Hematopoietic stem cell (HSC) transplantation is used as")
� Transplantation of Hematopoietic Stem Cells(HSC) Hematopoietic stem cell (HSC) transplantation is used as therapy for: � 1. Hematopoietic malignancies. e. g. Leukemia � 2. Aplastic anemia’s. � 3. Certain inherited disorders e. g. immune deficiency states and severe forms of thalassemia. Sources of Hematopoietic Stem Cells for Transplantation: � � 1. from donor bone marrow, 2. from the umbilical cord blood of newborns, a readily available rich source of HSCs.

� The recipient receives chemotherapy and/or irradiation to destroy malignant cells (e. g. , in leukemia) and to create a graft bed; then, HSCs are infused into the peripheral blood, from which they home to bone marrow. Rejection of allogeneic HSC transplants seems to be mediated by some combination of host T cells and NK cells that are resistant to radiation therapy and chemotherapy.
 Transplantation: 1. graft-versus-host disease(GVHD) : This occurs when immunologically")
Complications of Hematopoietic Stem Cells(HSC) Transplantation: 1. graft-versus-host disease(GVHD) : This occurs when immunologically competent T cells (or their precursors) are transplanted into recipients who are immunologically compromised. Acute GVHD (occurring days to weeks after transplantation): causes epithelial cell necrosis in three principal target organs: liver, skin, and gut. Chronic GVHD may follow the acute syndrome or may occur insidiously. The patients develop skin lesions resembling those of systemic seclerosis.


Immunodeficiency Syndromes • Primary immunodeficiencies are usually hereditary and manifest between 6 months and 2 years of life as maternal antibody protection is lost. • Secondary immunodeficiencies result from altered immune function due to infections, malnutrition, aging, immunosuppression, irradiation, chemotherapy, or autoimmunity.
: Definition: inherited immunodeficiency characterized by developmental failure to")
Primary Immunodeficiencies X-Linked Agammaglobulinemia (Bruton’s Agammaglobulinemia): Definition: inherited immunodeficiency characterized by developmental failure to produce mature B cells and plasma cells, resulting in aggamaglobulinemia Result from genetic mutation of B cell bruton tyrosine kinase(BTK)(normally expressed in early B cells and is critical for B-cell maturation, T cells are entirely normal. Clinical finding: Male infant Recurrent infections beginning at 6 months of life Common infections: pharyngitis, otitis media, bronchitis, and pneumonia Organisms: H. influenza, s. pneumococcus, and staph aureus

Di. George syndrome: definition: embryologic failure to develop the 3 rd and 4 th pharyngeal pouches, resulting in the absence of the parathyroid gland thymus clinical findings: hypocalcemia and tetany T cell deficiency Recurrent infection with viral and fungal organisms
 � Definition: combined deficiency of both cellular and humoral mediated")
Severe combined immunodeficiency (SCID) � Definition: combined deficiency of both cellular and humoral mediated immunity due to stem cell defect Mode of inheritance X-linked ( chemokine receptor mutation) Autosomal recessive ( deficiency of adenosine deaminase) Clinical features: Susceptible to candida cytomrgalovirus and pneumocystic carini infection Other immunodeficiency disease: Wiskott Aldrich syndrome Isolated Ig. A immunodeficiency Hyper Ig. M syndrome Genetic deficiency of the complement

Thank you
- Slides: 14