IMAGING IN LYMPHOMA Diagnosis Staging Responce assesment Follow










![2 -[F-18]fluoro-2 -deoxy-dglucose](https://slidetodoc.com/presentation_image_h2/c9f3e35621e6d41192f777a0e9e83396/image-14.jpg "2 -[F-18]fluoro-2 -deoxy-dglucose")

 Typically high FDG uptake Diffuse")





- Slides: 27
IMAGING IN LYMPHOMA Diagnosis Staging Responce assesment Follow up
Conventional radiology
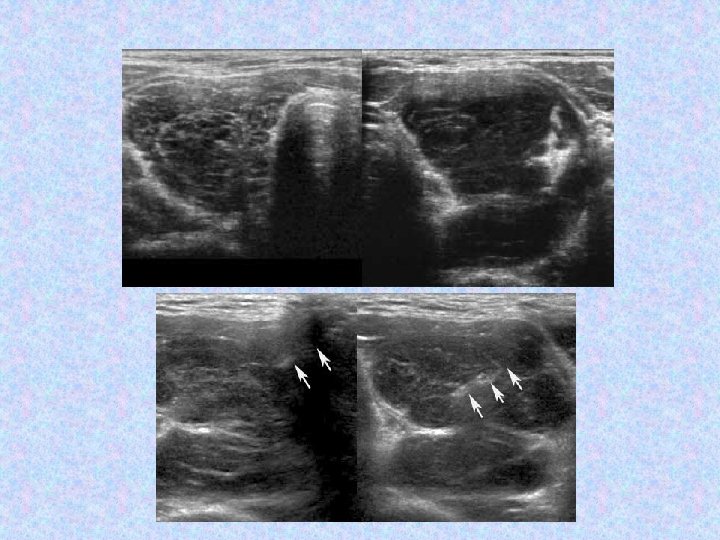
Ultrasonography
MRI
Diffusion weighted MRI
whole body DW MRI
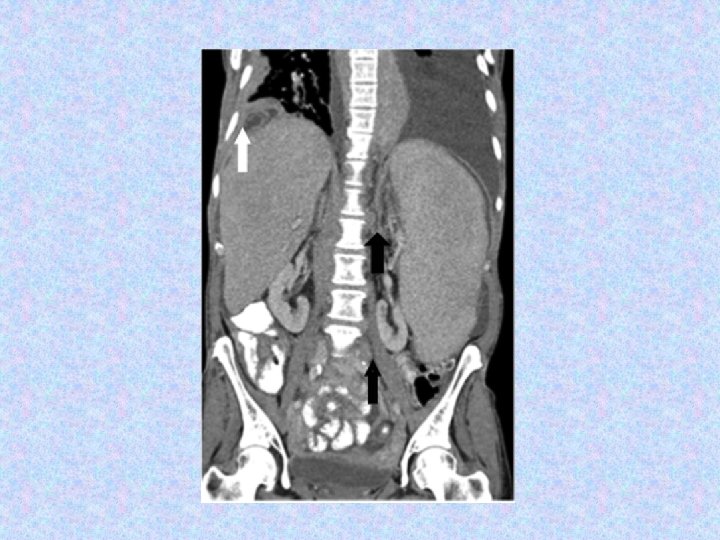
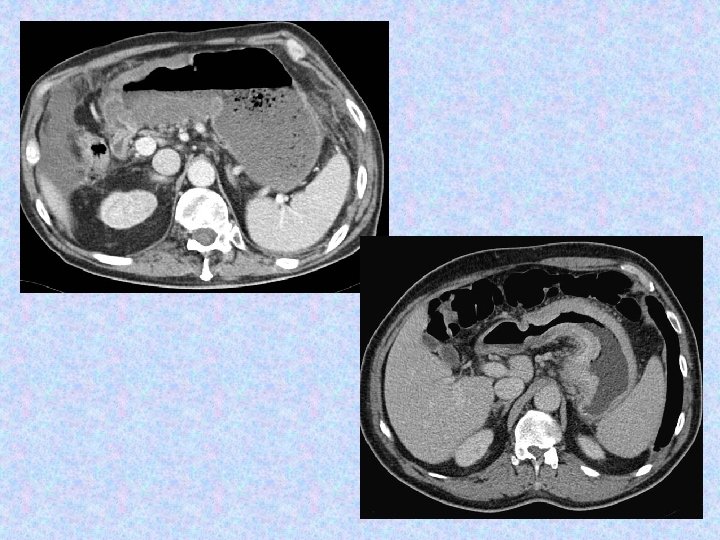
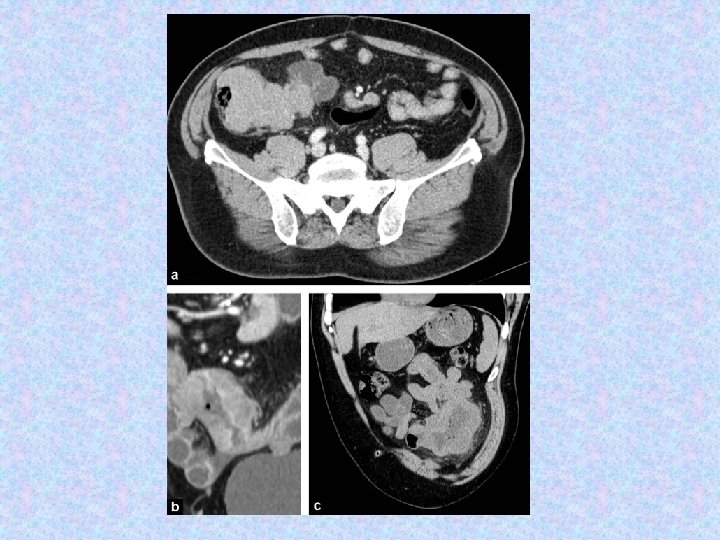
MDCT The essential anatomic method
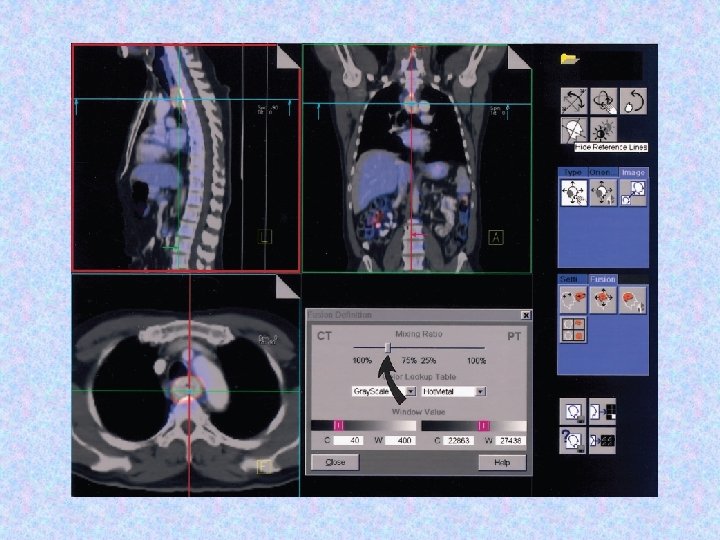
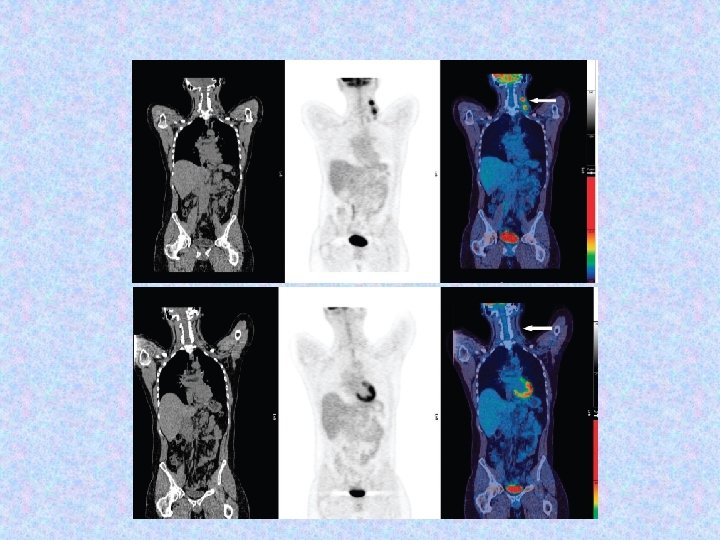
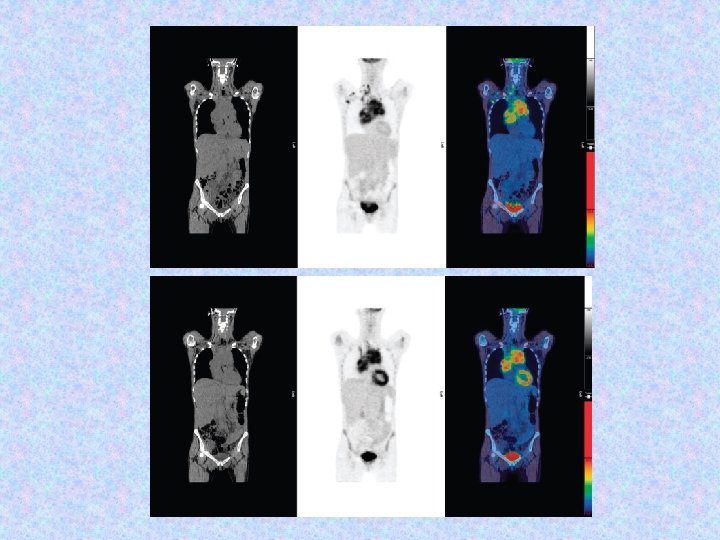
FDG/PET-CT Essential imaging test for staging, treatment planning, and response assessment of many lymphomas
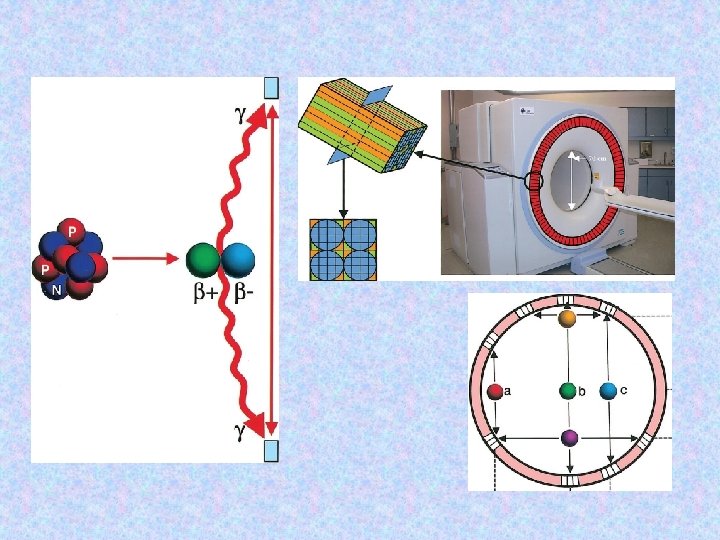
Hybrid PET-CT scanner
2 -[F-18]fluoro-2 -deoxy-dglucose
Differential uptake of FDG
TYPE FDG AVIDITY Hodgkin lymphoma (10% of all lymphomas) Typically high FDG uptake Diffuse large B-cell lymphoma (33% of NHL) Typically high FDG uptake Follicular lymphoma (20% of NHL) Variable (low to moderate FDG uptake) Marginal zone lymphoma (9% of NHL) Variable (none to high FDG uptake) Chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma of CLL type (7% of NHL) Variable (low to moderate uptake); high avidity suggests malignant transformation Mantle cell lymphoma (MCL) (7% of NHL) Variable (low to high FDG uptake)
In identifying lymph node involvement: CT SENSITIVITY 88% SPECIFITY 86% PET -CT SENSITIVITY 94% SPECIFITY 100%
For organ involvement: CT SENSITIVITY PET -CT SENSITIVITY 50% 88% SPECIFITY 90% 100%
Lugano Criteria for Response Assessment on CT Complete Response Complete disappearance of radiologic evidence of disease Partial Response Progressive No Disease Response If only a single lesion is present, 50% decrease in the PPD <50% decrease New or from baseline increased adenopathy; Splenic volume increase
The five-point scale of FDG uptake 1 No FDG uptake > background 2 FDG uptake < mediastinum 3 FDG uptake > mediastinum but < liver 4 FDG uptake moderately > liver 5 FDG uptake markedly >>liver and/or new lesions
Lugano Criteria for Response Assessment on PET-CT Complete Response Score of 1, 2, 3 in nodal or extranodal sites Partial Response Progressive No Disease Response Score of 4 or 5 Score 4 or 5 in with no obvious any lesion with reduced uptake change in FDG an increase in compared with uptake intensity of baseline uptake from baseline