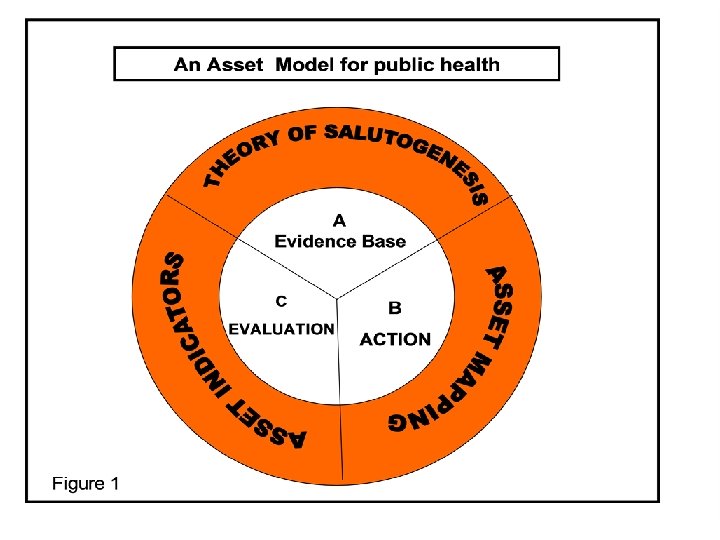
Illustrating The Asset Model For Public Health Applications

Illustrating The Asset Model For Public Health: Applications For Policy, Research And Practice In Young People’s Health Antony Morgan, Fiona Brooks CRIPACC, University of Hertfordshire www. hbscengland. com

‘The misery of youth: Teenagers depressed and fearful as drink, drugs and crime take their toll’ July 2008, Daily Mail

The Asset Model… ‘. . policy development has focused too much on the failure of individuals and local communities to avoid disease rather than their potential to create and sustain health and continued development’ Source: Morgan and Ziglio (2007)

Assets versus deficits for Young People The more we provide young people with opportunities to experience and accumulate the positive effects of protective factors (health assets), the more likely they are to achieve and sustain mental well being in later life

Health assets – how are they defined? • A health asset can be defined as any factor (or resource), which enhances the ability of individuals, communities and populations to maintain and sustain health and well-being. • Examples might include: – resilience as a protective factor for young peoples health development and wellbeing – social capital may act as a protective factor for communities particularly those that are most disadvantaged ?

Assets and Deficits • Deficit models focus on identifying problems and needs of populations requiring professional resources, resulting in high levels of dependence on hospital and welfare services (risk factors and disease). • In contrast: Asset models tend to accentuate positive ability, capability and capacity to identify problems and activate solutions , which promote the self esteem of individuals and communities leading to less reliance on professional services

Assets and deficits • What makes us strong? Risk factors: • Fitness • What factors make us more resilient (more able to cope in times of stress)? • Body Fat • Cholesterol • What opens us to more fully • Smoking experience life? • Excess alcohol and other drugs

Supporting Macro Environment Good Education Decent Housing Increasing personal socioeconomic circumstances – chances for increasing well being Access to health promoting physical environments High Standards of Living Key development assets Increasing age – less opportunity for mental well being to effect +ve health promoting behaviour Young People’s Mental Well Being Positive Health Promoting Behaviour Low levels of substance misuse Increased healthy eating and physical activity Safer sexual health Low incidence of bullying
 n Support (family relationships, caring school and neighbourhood) n")
40 Development Assets (Scales, 2001) n Support (family relationships, caring school and neighbourhood) n Empowerment (community values youth, young people seen as resources) n Constructive use of time (participation in clubs and associations) • Commitment to learning (achievement motivation) • Positive values (caring and responsible to others) • Social competencies (cultural competence, peaceful conflict resolution • Positive identity (self esteem

Mechanisms and pathways for building young people’s health e. g. social cohesion and wellbeing Emotional Well Being Social Cohesion (feelings of safety and trust, sense of belong Social Well Being Mental Well Being Psychological Well Being P O S I T I V E H E A L T H B E H A V I O U R S
 more important than others?")
Modelling Assets Using HBSC • Are some assets (protective factors) more important than others? • What are the cumulative effects of multiple assets on young people's mental well being? • How do different social and cultural impact on the benefits of these assets? ‘Redressing the balance between asset and deficit models for research’

Summary • Focuses on positive health promoting and protecting factors for the creation of health. • Emphasis on a life course approach to understanding the most important key assets at each life stage. • Passionate about the need to involve young people in all aspects of health development process • Recognises that many of the key assets for creating health lie within the social context of young people’s health inequalities • Helps to reconstruct existing knowledge in such a way as to help policy and practice to promote positive approaches to health

Positive Lives, Positive Futures
")
Life Satisfaction in Adolescent Girls: An Assets-Based Investigation (HBSC)

Life Satisfaction An individual’s subject sense of life satisfaction is an important aspect of overall well-being In young people associated with significant health related outcomes and life chances. Middle years of childhood little gender differentiation in life satisfaction Mid adolescence in majority of countries in Europe and North America girls consistently report lower life satisfaction than male peers

Boys 15 year olds with high life satisfaction Girls

Life Satisfaction – England 2010 90 88 86 84 Girls life satisfaction 2005/6 Girls life satisfaction 2009/10 82 Boys life satisfaction 2005/6 Boys life satisfaction 2009/10 80 78 76 74 11 year old 13 year old 15 year old

Mental Health 19 Source Morgan et al 2008 HBSC

Life Satisfaction – an assets approach Association between subjective life satisfaction in young people and health related risk behaviours (Thome and Espelage 2004; Zullig 2001) Factors that may operate in a protective way to sustain high life satisfaction among girls have been given relatively less attention. Aim: To identify and examine potential assets that may function to support and sustain positive life satisfaction among adolescent girls.

Life Satisfaction A self-reporting of life satisfaction. Measured using a Cantril Ladder. Here is a picture of a ladder. The top of the ladder ‘ 10’ is the best possible life for you and the bottom ‘ 0’ is the worst possible life for you. In general, where on the ladder do you feel you stand at the moment? Tick the box next to the number that best describes where you stand. 10 Best possible life 9 8 7 6 5 4 3 2 1 0 Worst possible life

Identifying factors related to Life Satisfaction 132 candidate variables from HBSC survey associated with the following topics: • Age • Communication with friends • Parental control • Eating • Socialising • Dieting • Hygiene • Leisure activities • Parental smoking • Health • Academic achievement • Peers smoking • Smoking • Life at school • Periods started • Alcohol • Family affluence • Fighting • Communication with parents • Bullying • Neighbourhood • Feelings • Living arrangements Analyse using non-multilevel ordinal regression.

Results of modelling Factors associated with life satisfaction Physical health • girls who eat vegetables at least two days a week have better life satisfaction; (p-values range from less than 0. 001 to 0. 024) • girls who do not smoke have better life satisfaction than those who smoke every day; (p-value = 0. 001) • the better that girls rate their health, the better their life satisfaction; (p-values all 0. 001 or lower) • girls who are "extremely" or "very" fit and well have better life satisfaction than others. (p-values all 0. 041 or lower)

Emotional well-being • girls who do not see themselves as "much too fat" have better life satisfaction (p-values range from 0. 003 to 0. 024); • the less girls say they "feel low", the greater their life satisfaction. (p-values range from less than 0. 001 to 0. 006).

Community and School • girls who like school have better life satisfaction than those who "don't like it at all” (p-values range from less than 0. 001 to 0. 003) • girls who agree that where they live people say 'hello' have better life satisfaction than those who disagree a lot (p-values of 0. 001 and less than 0. 001 respectively) • girls who do not "disagree a lot" that they have good places to go have better life satisfaction than others. ” (pvalue = 0. 008).

Family Life • girls who have been on vacation more than twice in the past 12 months have better life satisfaction than those who have been only once or not at all (p-values of less than 0. 001 and equal to 0. 001 respectively) • girls who find it "very easy" to talk to a father-figure have better life satisfaction (p-values of 0. 033 and 0. 027 respectively) • girls who responded "extremely" about doing things they wanted in free time have better life satisfaction (p-values range from less than 0. 001 to 0. 008); • the more positively girls agreed that their parents treated them fairly, the greater their life satisfaction. (p-values range from less than 0. 001 to 0. 037).

Potential Assets? Physical and emotional health Being highly physically active and accessing a good diet, navigating smoking as a risk behaviour - (as opposed to other risk behaviours) Having a positive body image related to weight and less often feeling low School and Community Enjoyment of school and feeling have a friendly community with at least some good accessible spaces (more significant than attainment and having a perceived ‘well off’ neighbourhood) Family Open democratic parenting style that allowed choices over free time and particularly a positive relationship with a father figure

Key issues & Questions Highlights key aspects of physical health and family, school and community life that may be most significant in terms of contributing to girls life satisfaction. What is the relationship to socio-economic circumstances? – points intersections between socio-economic inequalities and gender inequalities that may be significant for promoting gender equality ?

Key issues & Questions What assets based policy and practice actions would most support an improvement in girls life satisfaction? Millennium development goal gender equality and empowerment of women which is essential for better health and wellbeing (WHO, 2005).

Key Questions How valuable is an assets framework for understanding girls health and well-being? Strengths ? Limitations? How far does an assets framework provide a new understanding of girls health needs?

For More Infomation n f. m. brooks@herts. ac. uk antony. morgan@nice. org. uk n Morgan A and Ziglio E (2007) Revitalising the evidence base for public health: an assets model, Promotion and Education Supplement 2 pp 17 -22 n Morgan A, Davies M and Ziglio E (2010) Health Assets in a Global Context: Theory Methods Action. Springer: new York: In Press n Fenton, C, F Brooks, N Spencer and A Morgan. 2010. "Sustaining a positive body image in adolescence: an assets-based analysis. " Health and Social Care in the Community 18(2): 189 -198.
- Slides: 31