Il Reclutamento Alveolare Giuseppe Foti Istituto di Anestesia






 Vrec 20, He (ml) * 1000 800 Vrec 20 underestimates,")
 3000 2500 2000 1500 1000 All Δrec in ΔFRC !! 500")

 (suction flow 200 ml/min). Gas")
")























 PMI = PMusc. Index Foti")




 • High PMI &")

 what stays open at end expiration depends on what has been opened")


: 788 -95 Re-expansion of atelectasis during general anaesthesia:")

 2000 1800 1600 1400 1200 1000 800 600 All Δrec")







- Slides: 57
Il Reclutamento Alveolare Giuseppe Foti Istituto di Anestesia e Rianimazione Università di Milano-Bicocca dir. Prof. A. Pesenti Ospedale S. Gerardo Monza
Reclutamento Alveolare: riapertura zone collassate PEEP 5 PEEP 10 PEEP 15 • E’ la Pa. O 2 il miglior indicatore di Rec ? • E’ la PEEP il maggior determinante del Rec ?
Pa. O 2 dipende non solo da quello che accade agli alveoli… • • • Cardiac Output Emoglobina VO 2 p. H, CO 2 Vasocostrizione Ipossica (per es: NO) etc… Perché non misurare Rec dal versante alveolare ?
Chord Cpl Alveolar recruitment
Estimating Δrec by P/V curve analysis Assumes that FRC immediately equalizes coming from different PEEP
FRC is different coming from different Ventilatory SET UP !!
1200 Vrec 20 (ml) Vrec 20, He (ml) * 1000 800 Vrec 20 underestimates, not homogeneously , 600 Alveolar recruitment 400 * 200 0 -200 5 - 15
Pneumonia Volume (ml) 3000 2500 2000 1500 1000 All Δrec in ΔFRC !! 500 0 0 10 20 30 40 50 60 70 Paw (cm. H 2 O)
HOW TO NOT MEASURE FRC ? IT WORKS ! IT’S CLINICAL PRACTICE !
OXYGEN WASHIN WASHOUT sidestream O 2 analyser (OXIMON, Drager) (suction flow 200 ml/min). Gas sampling FRC Portable PC O 2 analyser
FRC = QO 2 / ΔFe. O 2 (Δ Fe. O 2 min: 20%) QO 2 = Q totale erogata – Q restituita al sistema – Q consumata Fi O 2 Fe O 2
WASHOUT vs HELIUM SLOPE INTERCEPT r 2 4000 0. 953 53 0. 960 Controlled 200 150 3000 Differences 100 2000 1000 50 0 -50 0 2000 3000 4000 -150 -200 0 1000 -250 0 1000 2000 3000 averages 4000 IT WORKS ! MAY BE CLINICAL PRACTICE in near FUTURE
Determinanti del Reclutamento alveolre 50 PEEP keep it open Pplat Open the Lung % 40 Opening pressure 30 Closing pressure 20 10 0 0 5 10 15 20 25 30 35 40 45 50 Paw [cm. H 2 O] Crotti et al. Am J Respir Crit Care Med 2001
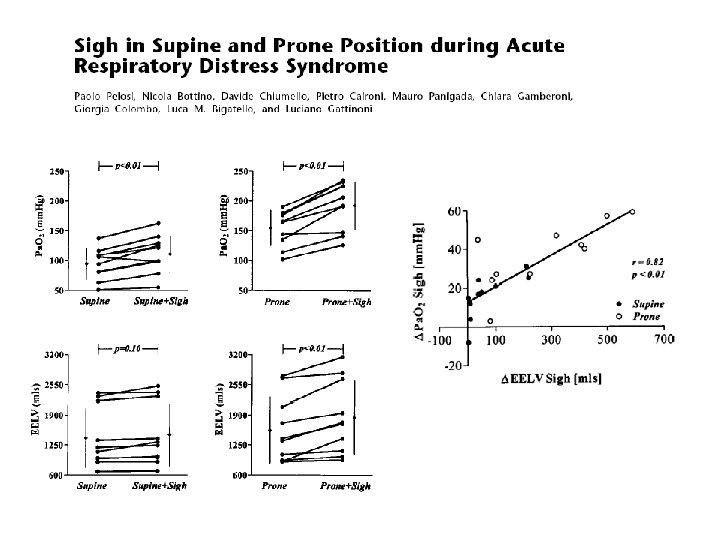
Recruitment maneuvers & SIGH
Slutsky style • • • Pressure = 35 -50 cm. H 2 O Time = 20 -40 sec, 1 -3 manoeuvre Mode: CPAP, APRV (lo vediamo nelle prove più tardi) Check: BP, Sp. O 2, on-line blood gas If vanishing effect PEEP
Recruitment maneuver 10 7 12 10 15
Lachmann’s style
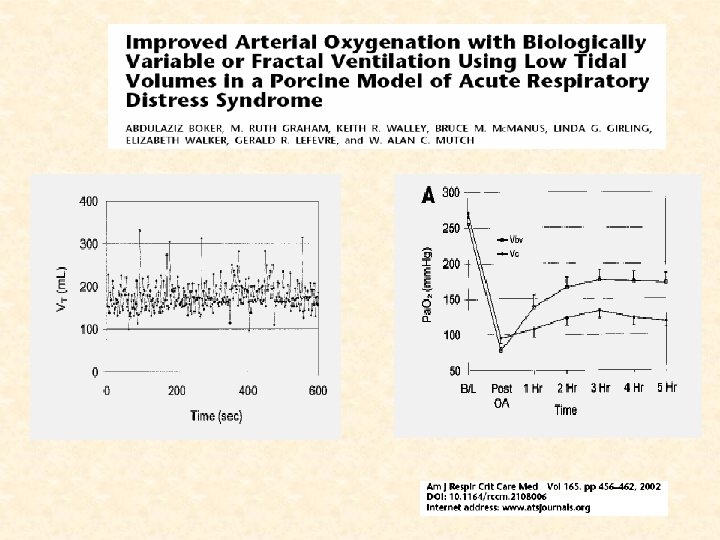
Effects of periodic lung recruitment maneuvers on gas exchange and respiratory mechanics in mechanically ventilated acute respiratory distress syndrome (ARDS) patients. Foti G. , Cereda M. , et al. Intensive Care Med 2000, 26 (5) 501 -07
Effects of periodic lung recruitment maneuvers on gas exchange and respiratory mechanics in mechanically ventilated acute respiratory distress syndrome (ARDS) patients. Foti G. , Cereda M. , et al. Intensive Care Med 2000, 26 (5) 501 -07
Alveolar Recruitment and positioning PRONATION
Perché funziona la pronazione ? Cominciamo dalle cose semplici Am. J. Respir. Crit. Care Med. , Volume 161, Number 5, May 2000, 1660 -1665 The Prone Position Eliminates Compression of the Lungs by the Heart RICHARD K. ALBERT and ROLF D. HUBMAYR
Diaphragm position and Distribution of ventilation PRONE SUPINE
Oxygenation Response to a Recruitment Maneuver during Supine and Prone Positions in an Oleic Acid–Induced Lung Injury Model NAHIT CAKAR, THOMAS VAN der KLOOT, MELYNNE YOUNGBLOOD, ALEX ADAMS, and AVI NAHUM Am J Respir Crit Care Med Vol 161. pp 1949– 1956, 2000 Prone + RMs effect Proning effect RMs should be repeated following prone position
Recruitment by recover of spontaneous breathing
Diaphragm activity and recruitment spontaneous breathing controlled ventilation, NMBA
BIPAP e Respiro Spontaneo
BIPAP vs PCV: Gas exchange BIPAP PCV Putensen et al. AJRCCM 2001; 164, 43 -49
Set: BIPAP+PSV, Pmax = 35 -40 cm. H 2 O Ti = 3 -5 s. RRBIPAP = 0. 5 -1 b. p. m .
Dynamics of re-expansion of atelectasis during general anesthesia Rothen HU, Neuman p, Berglund J, Valtaysson J, Magnusson a and Hedenstierna G. British J of Anesthesia (1999): 82, 4, 551 -6 Start 1. 5 sec. 1 sec. 3. 5 sec. L’insufflazione deve durare almeno 3 sec.
Sigh improves tollerance to spontaneous breathing
Conclusioni: -Pao 2 ma…. non per molto -Pplat per aprire -PEEP per mantenere aperto Partial Ventilatory Support RMs and SIGH Pronazione
Why SIGH during PSV ? Low PSV TV Muscle activity Derecruitment SIGH
Is it Partial Ventilatory Support ?
End Inspiratory occlusion: PMI = Pel, rsi - (PEEP+PS) PMI = PMusc. Index Foti G. , Cereda M et al. AJRCCM 1997
Prone positioning attenuates and redistributes ventilator-induced lung injury in dogs Alain Broccard, MD, FCCP; Robert S. Shapiro, MD; Laura L. Schmitz, MD; Alex B. Adams, MPH, RRT; Avi Nahum, MD, Ph. D; John J. Marini, MD CRITICAL CARE MEDICINE 1999; 27: 2574 -2575 PRONE SUPINE Prone position as “Lung Protective Strategy”?
What has been proven ? Prone - supine study
“The common theme of all the letter is that the use of prone position should not be descarded on the basis of the negative study by Gattinoni and collegues” A. Slutsky NEJM Vol 346, n° 4, Jannuary 24, 2002 pag 297
End Inspiratory occlusion: • Low PMI & low effort (A) • High PMI & high effort (B) Foti G. , Patroniti N. Pesenti A. in “Tecniche di ventilazione artificiale”ed. Torri G. -Calderini E.
MV day 7. 1± 1. 5 1. 0 ± 0. 3 Est, cw 10 ± 2 6 ± 1 Pao-Pes 19 ± 3 29 ± 2
Conclusion: 1) what stays open at end expiration depends on what has been opened at end inspiration 2) Adjusty PEEP to mantain recruitment
Respiratory mechanics BIPAP PCV Putensen et al. AJRCCM 2001; 164, 43 -49
Recruitment maneuver and anesthesia Fi. O 2 0. 4 Post induction Post recruitment 5’ 45’ Fi. O 2 1
Br J Anaesth 1993 Dec; 71(6): 788 -95 Re-expansion of atelectasis during general anaesthesia: a computed tomography study. Rothen HU, Sporre B, Engberg G, Wegenius G, Hedenstierna G. Area of atelectasis (cm 2) Ci vogliono almeno 30 cm. H 2 O per riaprire le zone collassate
During OA injury PEEP trial
Legionella Pneumoniae Volume (ml) 2000 1800 1600 1400 1200 1000 800 600 All Δrec in ΔEELV !! 400 200 0 0 10 20 30 40 50 60 70 Paw (cm. H 2 O)
Closed Dilution Technique Ci Vi FRC Mass conservation Cf Vf ? Ci - Vi FRC = Vi Cf
Helium dilution technique 1 3 2 4 Patroniti N et al. Intensive Care Med 2004; 30: 282
RM’s and hemodynamics
Recruitment maneuvers Let’s require transpulmonary opening pressure equal to 30 cm. H 2 O [“sticky atelectasis”] Paw applied = 40 cm. H 2 O “Soft” Cw “Stiff” Cw EL/Etot = 0. 8 TP = 32 cm H 2 O EL/Etot = 0. 5 TP = 20 cm H 2 O opened closed RMs Pressure for “Stiff” Cw
Tecniche di reclutamento alveolare: • Play with ventilators – RMs, SIGH • Positioning – Pronation • Partial Ventilatory Support – BIPAP – PSV
• 3 consecutive VC breaths • Pplat 45 cm. H 2 O • No Insp. Pause • Ti = 2. 5 sec. No commercial machine can perform Sigh the way we studied it
Courtesy Prof Rouby