IDIOPATHIC SCOLIOSIS Dr Samir Al sayegh Consultant Pediatric





: S Calculated by subtracting the convex")
















")











- Slides: 35
IDIOPATHIC SCOLIOSIS Dr. Samir Al sayegh Consultant Pediatric Orthopedic and Spine Surgeon King Abdullah Specialized Children Hospital S
Idiopathic Scoliosis S Idiopathic scoliosis is a structural lateral curvature of the spine for which no cause can be established with cobb angle ≥ 10°. S Traditionally, idiopathic scoliosis has been categorized based on the patient's age at onset: S Infantile (0 to 3 years) S Juvenile (4 to 9 years) S Adolescent (10 years to maturity)
Idiopathic Scoliosis S Idiopathic scoliosis now is divided into only two subgroups: S early onset (0 to 5 years) S late onset (after the age of 5 years)
Infantile Scoliosis S This category comprises about 1% of all idiopathic scoliosis in children. S Infantile scoliosis is unique in many ways: S It presents as a left thoracic curve in approximately 90% of cases S 60% of patients are males S Most curves develop within the first 6 months of life S Approximately 85% of these curves are self-limited and resolve spontaneously
Infantile Scoliosis S Bad prognostic factors: S Female gender S Right thoracic curve S Double structural curves S Curves appear after age of one year
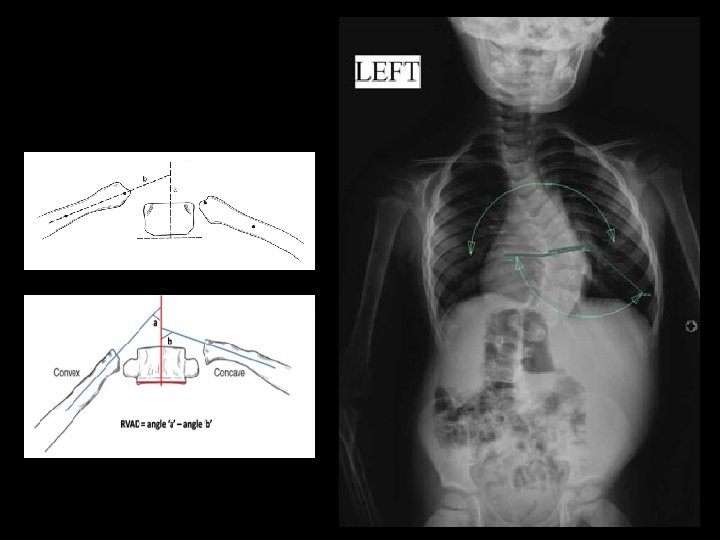
Infantile Scoliosis S Mehta rib-vertebral angle difference (RVAD): S Calculated by subtracting the convex value from the concave value at the apical vertebra of the thoracic curve. S If the angle is greater than 20 degrees, the child is likely to fall into the 15% category of individuals who progress. S If the angle if less than 20 degrees, the curve is likely to resolve
Infantile Scoliosis S The phase of the rib head: S It is based on the relation of the head and neck of the ribs to the vertebral body at the apex of the scoliosis S If the convex rib does not overlap the vertebral body on the anteroposterior radiograph, it is classified as phase I S If overlaps the vertebral body, it is classified as phase II
Infantile Scoliosis S Treatment S Observation S Bracing S Casting S Surgery
Infantile Scoliosis S Observation: S It is usually the first method of treatment for a young child with a spinal deformity. S Follow up every four to six months and have new X-rays made and compare them with the previously made films. S Continue to observe as long as there is no drastic increase in the size of the curve. S If progression of the curve is documented, a different form of treatment will need to be instituted.
Infantile Scoliosis S Bracing: S The purpose of the brace is to slow the inevitable progression of the curve, not to correct the curve. S The curve should be flexible in bending films. S The child should wear the brace fulltime. Braces are generally removed for bathing and special occasions
Infantile Scoliosis S Casting: S The goal of casting in children under 2 years of age is curing the scoliosis. S This requires cast changes under anesthesia every 2 -3 months (minimum 5 casts) with the goal of achieving a straight spine. S A brace will be needed after the casting treatment is done to maintain correction. S Children demonstrating "recurrence" can be re-casted for four months to re-correct the deformity before continuing with brace management.
Infantile Scoliosis S Surgery: S Growing rods S MAGEC rods S SHILLA Procedure
Infantile Scoliosis S Growing Rods: S The theory of the growing rod operation is to allow for continued controlled growth of the spine. S The curve is spanned by one or two rods under the fascia to avoid damaging the growth tissues of the spine. The rods are then attached to the spine above and below the curve with hooks or screws. S The child then returns every six months to have the rods "lengthened” S When the child becomes older and the spine has grown, the doctor will remove the instrumentation and perform a formal spinal fusion surgery.
Growing Rods
Infantile Scoliosis S MAGEC Rods: S It is a growing rods system that expand using an external remote control in the outpatient clinic and do not require scheduled expansions in the operating room.
MAGEC Rods
Infantile Scoliosis S SHILLA Procedure: S It involves doing a short spinal fusion at the most curved portion (apex) of the spine using pedicle screws and rods. The rods are attached then at the top and bottom of the spine to pedicle screws without locking plugs that allow for continued growth of the spine.
SHILLA Procedure
Juvenile Scoliosis S This category comprises about 10% to 15% of all idiopathic scoliosis in children. S Juvenile curves that reach 30 o tend to continue to worsen without treatment. S Bracing is often used to manage these curves. S nearly 95% of children in the juvenile age range go on to surgical treatment.
Juvenile Scoliosis S Treatment: S Observation S Bracing S Surgery
Adolescent Scoliosis S By far the most common type of idiopathic scoliosis. S Adolescent idiopathic scoliosis generally does not result in pain or neurologic symptoms. S If these symptoms occur, further evaluation and testing may be necessary.
Adolescent Scoliosis S Physical Findings: S Shoulder height asymmetry S Waistline asymmetry S Trunkal shift S Prominence on the back or a rib hump S Normal neurological examination
Adolescent Scoliosis S Imaging Studies: S A standing X-ray of the entire spine (PA/Lateral) S Bending spine X-ray. S Traction spine X-ray. S MRI whole spine.
Adolescent Scoliosis
27° 24° 55° T 12 -7° 20° 60°
15° 20°
Adolescent Scoliosis
Adolescent Scoliosis S Treatment: S Observation S Bracing S Surgery
Adolescent Scoliosis S Observation: S Observation is generally for patients whose curves are less than 25º who are still growing, or for curves less than 45º in patients who have completed their growth.
Adolescent Scoliosis S Bracing: S Bracing is for patients with curves that measure between 25º and 40º during their growth phase. S The goal of the brace is to prevent the curve progression.
Adolescent Scoliosis S Surgery: S Surgical treatment is used for patients whose curves are greater than 45º while still growing or greater than 50 º when growth has stopped. S The goal of surgical treatment is two-fold: S To prevent curve progression S To obtain spine balance and curve correction
Adolescent Scoliosis S Approaches: S Posterior only S Anterior only S Combined Anterior and posterior
27° 24° 55° T 12 -7° 20° 60°