Identifying HIV2 Infections Using Differential Serological Assays HIV1
/HIV-2(gp 36) (Select HIV or")






 /HIV-2 /(gp 36)")
 Misdiagnosis: Cross Reaction on HIV-1 Western Blot SIV Western Blot")
![HIV-1/HIV-2 Discriminatory Assays HIV-1 /HIV-2 EIA [Select- HIV Adaltis Inc. ] • Individual microwells](https://slidetodoc.com/presentation_image_h/767bb5004a3f5fa13e333acefa4df688/image-12.jpg "HIV-1/HIV-2 Discriminatory Assays HIV-1 /HIV-2 EIA [Select- HIV Adaltis Inc. ] • Individual microwells")
![HIV-1/HIV-2 Discriminatory Assays Multispot HIV-1/HIV-2 Rapid test [Bio. Rad] • Incorporates highly conserved HIV-1](https://slidetodoc.com/presentation_image_h/767bb5004a3f5fa13e333acefa4df688/image-13.jpg "HIV-1/HIV-2 Discriminatory Assays Multispot HIV-1/HIV-2 Rapid test [Bio. Rad] • Incorporates highly conserved HIV-1")
 • Non-discriminatory: extensive cross reactivity")
 • SIV extensive Cross reactivity with HIV-2 antibodies •")





 Specimens Detected (10/01/04 - 09/30/07) • 11 specimens were confirmed HIV-2(+) from")


- Slides: 23
Identifying HIV-2 Infections Using Differential Serological Assays HIV-1 (gp 41)/HIV-2(gp 36) (Select HIV or Multi. Spot) by Testing HIV EIA Reactive Specimens Unconfirmed HIV-1 Antibody by HIV-1 Western Blot Robert A. Myers Ph. D.
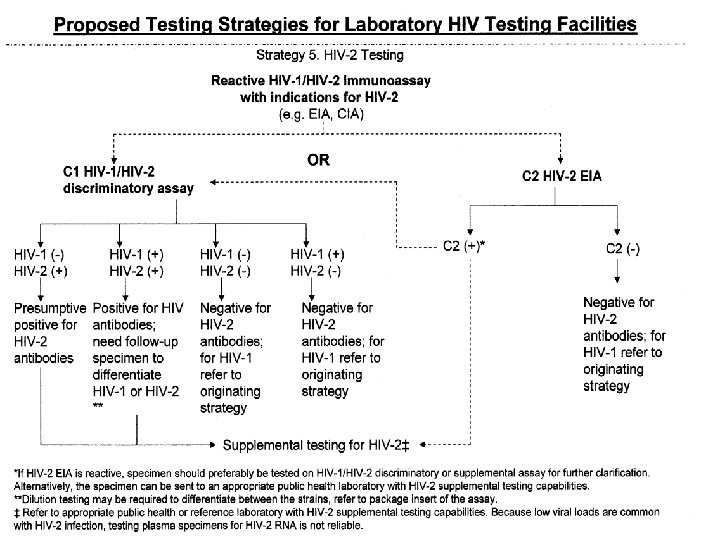
Presentation Overview • The key feature of proposed testing Strategy #5 is the use of a HIV-1/HIV-2 discriminatory assay to quickly identify presumptive HIV-2 infections by testing HIV EIA reactive specimens that cannot be conclusively confirmed positive for HIV-1 antibodies • For over 15 years our laboratory has successfully used HIV-1/HIV-2 discriminatory EIA and/or HIV-1/HIV-2 rapid test to routinely identify presumptive HIV-2 cases that sporadically appear in our testing population
Presentation Overview • Why do we need to routinely perform HIV-2 screening in Maryland? • What assays are used in our HIV-2 testing strategy? • What have we found using HIV-1/HIV-2 discriminatory assays as proposed in testing strategy #5 ?
Why do we routinely test for HIV-2 In Maryland? • In in 1991 we conducted a retrospective study that re-tested HIV-1 WB indeterminate sera using HIV-2 specific synthetic peptide EIA’s and found 8 specimens of 457 tested that were confirmed positive for HIV-2 antibodies (J. AIDS 1992. 5: 417 -423) • These specimens were from 4 HIV-2 infected individuals who were identified using available demographic information as West African expatriates living in the MD suburbs of Washington DC
Maryland in the Shadow of the National Capitol • Washington DC is an International City associated with extensive international travel and immigration into the region • Significant HIV diversity has been documented in our testing populations in the DC metro area • All HIV-2 cases documented to date in our testing populations were from two MD Counties in the DC metro area
HIV-1 Genetic Diversity In Maryland
HIV-2 Cases in Maryland • Using HIV-1/HIV-2 discriminatory assays as • • proposed in testing strategy #5 on average we have found one to two new HIV-2 infected individuals in our testing population each year since 1991 for a total of 30 documented HIV-2 cases to date 5 of the 30 HIV-2(+) patients were negative in HIV-1 viral lysate based assays 9 of 18 HIV-2(+) patients were negative in HIV-1 recombinant protein based EIA (Recombigen) All HIV-2 cases had antibodies that cross reacted with gag and/or pol antigens on HIV-1 western blots Cross reactions to HIV-1 env antigens were less pronounced ( in one case complete cross reactions gag pol and env HIV-1 antigens was documented)
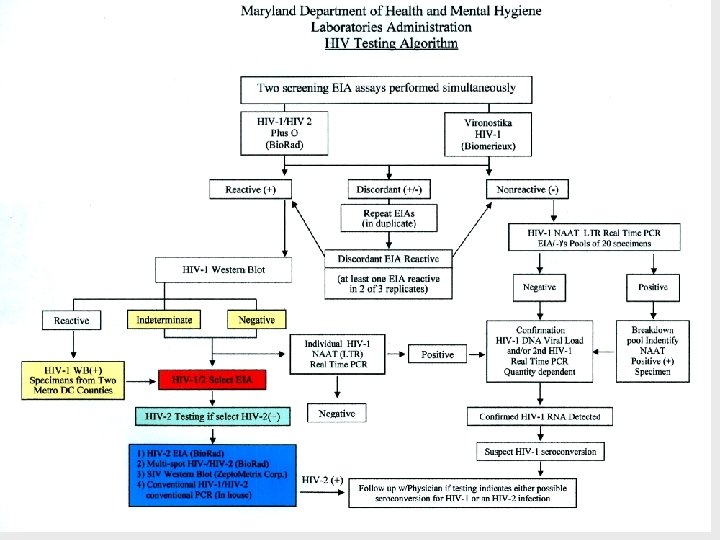
HIV-2 Testing Strategy • We internally use a differential HIV-1(gp 41) /HIV-2 /(gp 36) synthetic peptide EIA (Select HIV ) to initially identify HIV-2(+)’s from HIV-1/HIV-2 screening EIA(+)’s not confirmable as HIV-1 (+) by WB • We also test all HIV-1 WB(+) specimens from two Maryland Counties adjacent to Washington DC where the majority of HIV-2 infections routinely are found in Maryland • If HIV-2 infection is suspected [Select EIA: HIV-2 (+)] we perform: • HIV-2 EIA ( Bio-Rad) reportable • Multi-spot (Bio-Rad) reportable • SIV WB ( Gene Labs) • In-house conventional proviral HIV-1/HIV-2 (LTR) DNA PCR (requires fresh EDTA blood for PBMC’s)
HIV-2 (+) Misdiagnosis: Cross Reaction on HIV-1 Western Blot SIV Western Blot
HIV-1/HIV-2 Discriminatory Assays HIV-1 /HIV-2 EIA [Select- HIV Adaltis Inc. ] • Individual microwells coated with either HIV-1 or HIV 2 transmembrane synthetic peptide antigens • EIA binding ratio determines HIV specific reactivity: • Binding ratio: HIV-2 (O. D. signal)/HIV-1 (O. D. signal) >2. 0 HIV-2 , <0. 5 HIV-1 and>0. 5 to <2. 0 dual HIV-1 and HIV-2 reactivity dilute specimen to determine predominant reactivity • The Select–HIV EIA is not FDA approved therefore it is only used as supplemental test inconjunction with other HIV-2 assays in our HIV-2 testing algorithm
HIV-1/HIV-2 Discriminatory Assays Multispot HIV-1/HIV-2 Rapid test [Bio. Rad] • Incorporates highly conserved HIV-1 and HIV-2 • • recombinant or synthetic peptide transmembrane antigens coated on microscopic particles immobilized membrane in individual test cartridge Interpretation of individual spotted antigens determines HIV specific reactivity Dilution procedure for specimens demonstrating dual HIV 1 and HIV-2 reactivity at screening FDA approved for in vitro diagnostic use but is not approved to screen blood plasma , cell or tissue products We primarily use this assay as a supplemental test to verify HIV-1 or HIV-2 reactivity that has been demonstrated in other assays (i. e. , Select-HIV EIA or Genetic Systems HIV-2 EIA)
HIV-2 Assays HIV-2 Viral Lystate EIA (Genetic Systems Bio-Rad) • Non-discriminatory: extensive cross reactivity with HIV-1 antibodies and the non-specific reactions associated with 1 st generation EIA’s • FDA Approved Assay: Generates Reportable Results • When HIV-2 testing is specifically requested • When discriminatory assays are reactive for HIV-2 afterretesting HIV screening EIA reactive specimens that cannot be confirmed as HIV-1 positive • All specimens that were exclusively HIV-2 reactive specimens in the discriminatory assays were HIV-2(+) reactive in viral lystate EIA
SIV Western Blot (Zepto. Metrix) • SIV extensive Cross reactivity with HIV-2 antibodies • Used as a supplemental test to test HIV-2 EIA reactive specimens • Interpretation not standardized • Some cross reactivity to HIV-1 antibodies can be observed primarily to gag and pol antigens
Differential HIV-1 LTR and HIV-2 LTR Proviral DNA PCR’s • Requires PBMC separated from a • • fresh whole blood (EDTA) followup specimen Useful to resolve possible dual HIVHIV-1 -1/HIV-2 infection Conventional PCR : Sensitivity 10 copies/ PCR rxn. HIV-1 LTRIII & LTR IV primers (Refn. : J. Virology 1991; 65 : 28162828) Product Size: 255 bp HIV-2 LTRC & LTR D primers (Refn. : J. Virology 68 7433 -7447) Product Size: 199 bp
Notes: * 8 of 8 Confirmed positive for HIV-2 antibodies ** 3 of 30 Confirmed positive for HIV-2 antibodies
HIV-1 Western Blot Indeterminate Specimens With HIV-2 Reactivity • 8 specimens from 5 individuals demonstrated strong HIV -2 reactivity in the Select HIV EIA (signal/cut off values(17. 05 -21. 05) and had undiluted HIV-1/HIV-2 binding ratios of [325 to 14. 2 : >2. 0= HIV-2(+)] • All 8 strongly HIV-2 reactive specimens were confirmed as HIV-2(+) by Mutispot: HIV-2(+), Viral Lysate HIV-2 EIA(+) and SIV WB(+) • In two of the 5 individuals follow-up proviral HIV-2 LTR PCR testing demonstrated HIV-2 DNA in the patients PBMC’s
HIV-1 Western Blot Negative Specimen With HIV-1/HIV-2 Reactivity • One hemolized specimen demonstrated weak HIV-1 /HIV-2 reactivity in Select HIV EIA for HIV-1 (signal/cutoff: 1. 14) and HIV-2 (signal/cutoff: 1. 89) Binding ratio (1. 74: undifferentiated at screening dilution) • This specimen was initially only reactive in the HIV 1/HIV-2 Plus O EIA (signal/cutoff: 4. 95) , was HIV-1 WB(-) and HIV-1 NAAT(-) • The Select HIV EIA HIV-2 reactivity could not be verified by Multispot(-) and SIV WB(-) • Patient was negative in both EIA screening assays and both HIV-1/HIV-2 discriminatory assays upon follow-up
HIV-1 Western Blot Positive Specimens with HIV-1 & HIV-2 Reactivity • 3 specimens from the same individual had HIV-2 (+)binding ratios( avg. 21. 45) at the screening dilution. The HIV-2 (+) status was confirmed by Mutispot: HIV -2(+) by dilution, SIV WB(+) and proviral HIV-2 LTR (+) by PCR • 20 of 30 specimens dually reactive for HIV-1 & HIV-2 in the Select HIV EIA had limited HIV-2 cross reactivity that was resolved at the screening dilution by the HIV-2/HIV-1 binding ratios (<0. 5) that indicated HIV-1 infections • 7 specimens had HIV-1 binding ratios after dilution and were also Multispot HIV-1(+) after dilution
HIV-2 (+) Specimens Detected (10/01/04 - 09/30/07) • 11 specimens were confirmed HIV-2(+) from 6 individuals • 4 Specimens (2 individuals) were reactive in both EIA’s and were HIV-1 WB indeterminate • 2 Specimens (2 individuals) were reactive in the HIV-1/HIV-2 +O EIA and negative in the viral lysate EIA and were HIV-1 WB indeterminate • 2 Specimen (1 individual) was reactive in the HIV-1 /HIV-2 +O EIA and grey-zone reactive in the viral lysate EIA and was HIV-1 WB indeterminate • 3 specimens (1 individual )were reactive in both EIA’s and were HIV-1 WB positive
Concluding Remarks • Our data has demonstrated the utility of using discriminatory HIV-1/HIV-2 assays as proposed in testing strategy #5 to quickly and accurately identify HIV-2 infections in our testing population • We strongly recommend the routine use of a differential HIV-1/HIV-2 serology tests to properly evaluate reactive results from HIV-1/HIV-2 combination screening EIA’s if HIV-2 infections occur in your testing population • Recognize the need for manufacturers to develop cost effective HIV-1/HIV-2 discriminatory assays
Acknowledgements: • The staff of Maryland DHMH Retrovirology, Molecular Diagnostics, and Molecular Epidemiology Laboratories • The staff of Maryland DHMH AIDS Administration • The organizers of the CDC/APHL HIV Diagnostics Conference