IBLS Clinical presentation 1 2 nd year Medicine

IBLS Clinical presentation 1 2 nd year Medicine- May 2008 1

Objectives 1. Describe iron metabolism. 2. List the causes of iron deficiency. 3. Describe the clinical features in iron deficiency anaemia. 4. Describe the laboratory findings in a case of iron deficiency anaemia. 5. Describe the management in a case of iron deficiency anaemia. 2 nd year Medicine- May 2008 2

Case Scenario

• A 35 year old woman presented to the outpatient clinic with history of easy fatigability for many months. Recently she has noticed that she is short of breath from even the slightest exertion. She also has experienced periods of lightheadedness, though not to the point of fainting and the fact that her tongue is sore.

• She is now 34 weeks pregnant with her 4 th child in 5 years. She does not see any obstetrician and does not take any vitamins. Lately, she has developed pica for eating ice. She has regular bouts of vomiting due to the gastritis she developed since the beginning of her pregnancy.

Physical examination • Pale conjunctiva, pale gums, red swollen tongue, pale nail beds with mild spooning of nails, tachycardia, and a systolic murmur at the apex of the heart.
. • Blood film (microcytic, hypochromic). • Serum iron")
Investigations • Complete blood count (CBC). • Blood film (microcytic, hypochromic). • Serum iron (↓) and total iron binding capacity (↑). • Serum ferritin (low).
 8.")
Blood Sample Results Red Blood Cell Count 3. 0 million/mm 3 Hemoglobin (Hb) 8. 2 g/dl Hematocrit (Hct) 28% Mean Corpuscular Volume (MCV) 62 fl (normal 80 -95 fl) Mean Corpuscular Hb (MCH) 24 pg (normal 27 -34 pg) Serum Iron low Total Iron Binding Capacity in the Blood (TIBC) high Serum Ferritin low

Blood film

Stool examination • Stools are negative for occult blood, ova & cyst.

Classification of anemia according to red cell size
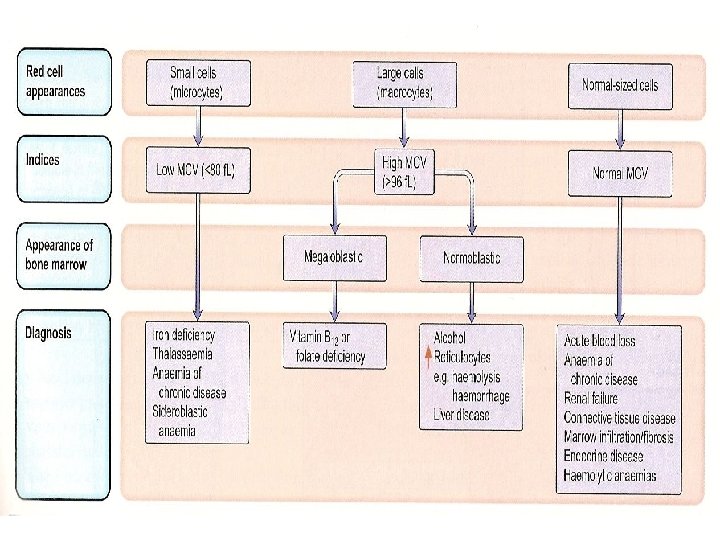

Differential diagnosis of microcytic hypochromic anemia 2 nd year Medicine- May 2008 13
 and how frequently does it occur? • Iron")
What is Iron Deficiency Anemia (IDA) and how frequently does it occur? • Iron deficiency is the most common cause of anemia in every country of the world. • It is the most important cause of a microcytic hypochromic anemia in which the two red cell indices MCV (mean corpuscular volume) and MCH (mean corpuscular haemoglobin) are reduced and the blood film shows small (microcytic) and pale (hypochromic) red cells.

• Iron is one of the most common elements in the Earth’s crust, yet iron deficiency is the most common cause of anaemia, affecting about 500 million people world wide (30% of world’s population).

• This is because of the body’s limited ability to absorb iron and the frequent loss of iron owing to hemorrhage.

IRON METABOLISM

2 nd year Medicine- May 2008 18

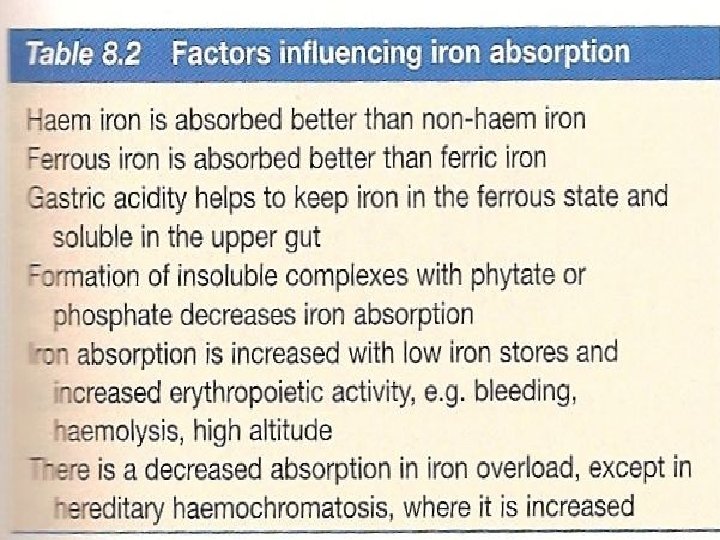
Iron Absorption

Causes of Fe Deficiency anemia • Chronic blood loss: – Uterine – GIT e. g. peptic ulcer, aspirin or other NSAID intake, carcinoma of stomach or colon, hookworm, piles. • Increased demands (growth & pregnancy) • Decreased absorption e. g. enteropathy or gastrectomy • Poor intake 2 nd year Medicine- May 2008 21
 • Presence of blood in")
Clinical History • Dietary intake • Regular self-medication (NSAID) • Presence of blood in feces (piles, Ca colon) • In women: – duration of periods – Occurrence of clots – No. of sanitary pads used (normal 3 -5/day)

Symptoms • • Fatigue Headaches Faintness Breathlessness Palpitations Angina Intermittent claudication

Signs General: • Pallor • Tachycardia • Systolic flow murmur Specific (epithelial changes due to inadequate • • iron in cells): Brittle nails Spoon-shaped nails (koilonychia) Angular stomatitis Glossitis

Pallor
")
Spooning of nails (Koilonychia)

Spooning of nails

Brittle nails

Angular Stomatitis 2 nd year Medicine- May 2008 29

Angular Stomatitis & Glossitis


Investigations • • • CBC Blood film Serum iron and total iron binding capacity Serum ferritin Other investigations: to determine the cause of the iron deficiency.

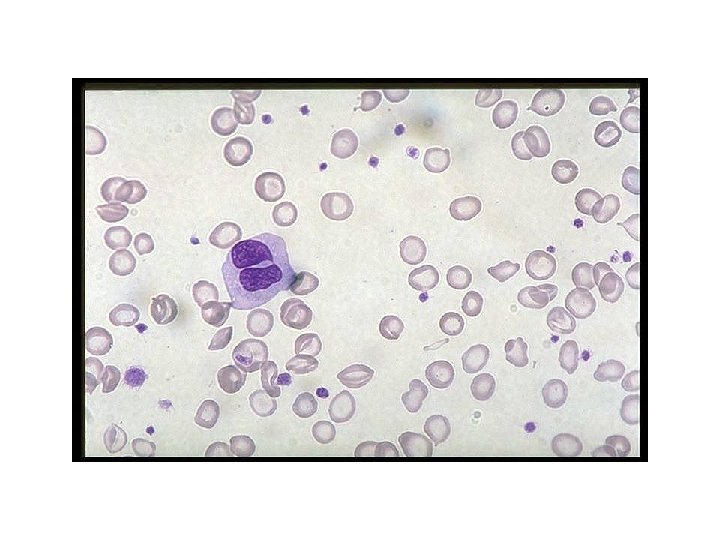
Normal peripheral blood smear showing a small lymphocyte. Normal RBC is about the size of a small lymphocyte
 and pale (hypochromic) RBC")
Blood film showing small (microcytic) and pale (hypochromic) RBC

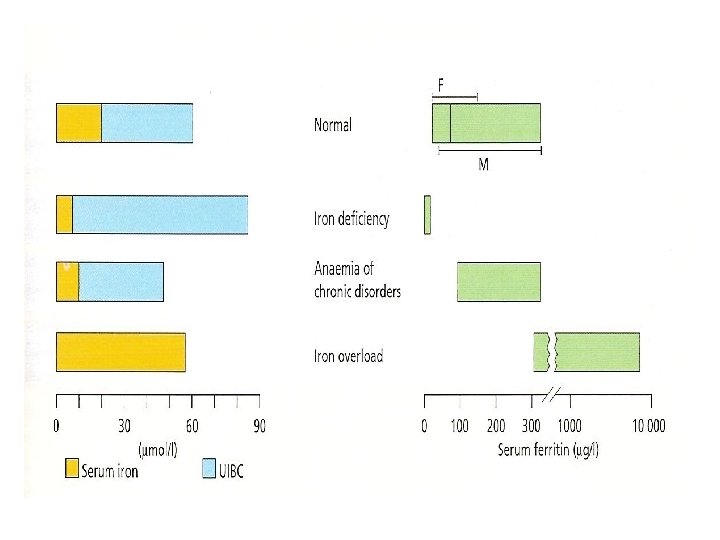
Serum iron and iron binding capacity • Serum iron falls. • Total iron binding capacity increases

Serum ferritin • The level of serum ferritin reflects the amount of stored iron. • Low serum ferritin confirms the diagnosis of iron deficiency.

• What treatment would you prescribe for this patient? How soon should you expect a response?

Treatment • Ferrous sulphate given as a tablet containing 200 mg of the salt (60 mg ferrous iron) t. d. s. • A small proportion of patients develop nausea, constipation or diarrhea.

• A response to oral medication usually appears in under 2 weeks. • The haemoglobin should rise by 1 g /dl every 710 days. • If no response is seen, it may be that the patient is not taking the tablets. • A check may be made by examining the stool which will be grey or black if the patient is ingesting iron. • Iron should be continued for 3 -6 months after the Hb has returned to normal to replenish iron stores.

Parenteral iron therapy • This is suitable for those very few patients: – who have general intolerance of oral preparations even at low doses. – Who are unable to absorb iron because of some disorder of the gastrointestinal tract. – In the late stages of pregnancy.

SUMMARY

2 nd year Medicine- May 2008 44
 is not a diagnosis per se.")
Take home message • Iron deficiency anemia (IDA) is not a diagnosis per se. • The correct management of IDA is to find and treat the underlying cause, and to give iron to correct the anemia and replace iron stores.
- Slides: 45