Hypoxic Ischemic Encephalopathy Rand Alshayeb Selena Abboud Definitions

Hypoxic Ischemic Encephalopathy Rand Al-shayeb Selena Abboud
 or complete (Anoxia) lack of oxygen")
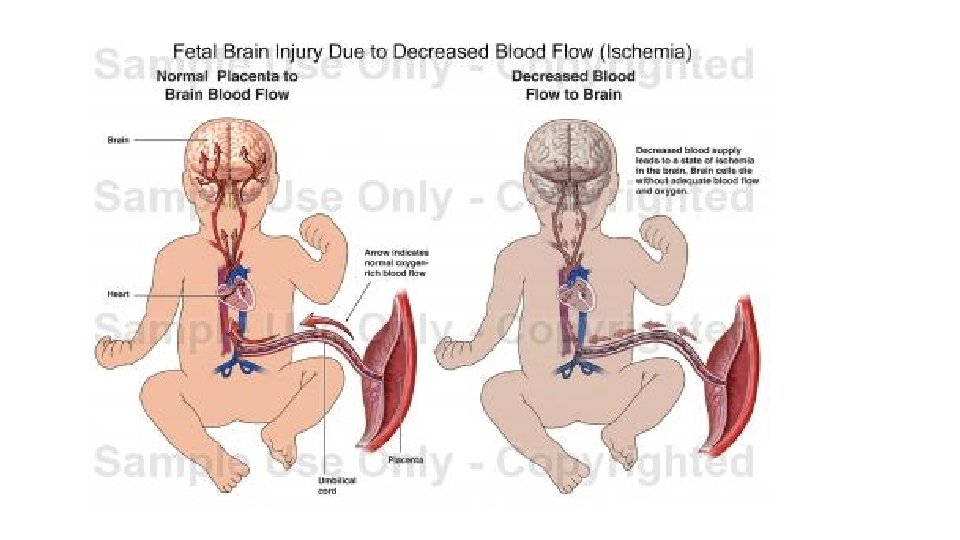
Definitions • Hypoxia or Anoxia: A partial (Hypoxia) or complete (Anoxia) lack of oxygen in the brain or blood. • Hypoxemia: Decreased arterial concentration of Oxygen. • Ischemia: The reduction or cessation of blood flow to an organ which compromises both oxygen and substrate delivery to tissue. • Asphyxia: The state in which placental or pulmonary gas exchange is compromised or ceases altogether. • Hypoxic Ischemic encephalopathy: An acute peripartum or intrapartum event leading to Abnormal neurological behavior in the neonatal period arising as a result of hypoxic ischemic event and The potential for significant mortality and long-term morbidity.

Incidence OF HIE • Occurs in 2 -5 per 1000 live term births in developed countries. (moderate to severe incidence is 1 -2/1000 live births) • 25% die or have multiple disabilities. • 4% have mild to moderate forms of cerebral palsy. • 10% have developmental delay.

Etiology of HIE Maternal • Cardiac arrest • Asphyxiation • Severe anaphylaxis • Status epilepticus • Hypovolemic shock Uteroplacental • Placental abruption. • Cord prolapse. • Uterine rupture. • Hyper stimulation with oxytocic agents. • Amniotic fluid embolism. • • • Fetal Fetomaternal hemorrhage (vasa praevia) Twin to twin transfusion syndrome Severe isoimmune hemolytic anemia Cardiac arrhythmia Intrauterine growth restriction (IUGR)

Pathophysiology The immature brain is in some ways more resistant to hypoxic-ischemic events compared to older children and adult: This may be due to: • Lower cerebral metabolic rate. • Immaturity in the development of the balance of the neurotransmitters. • Plasticity of the immature CNS.

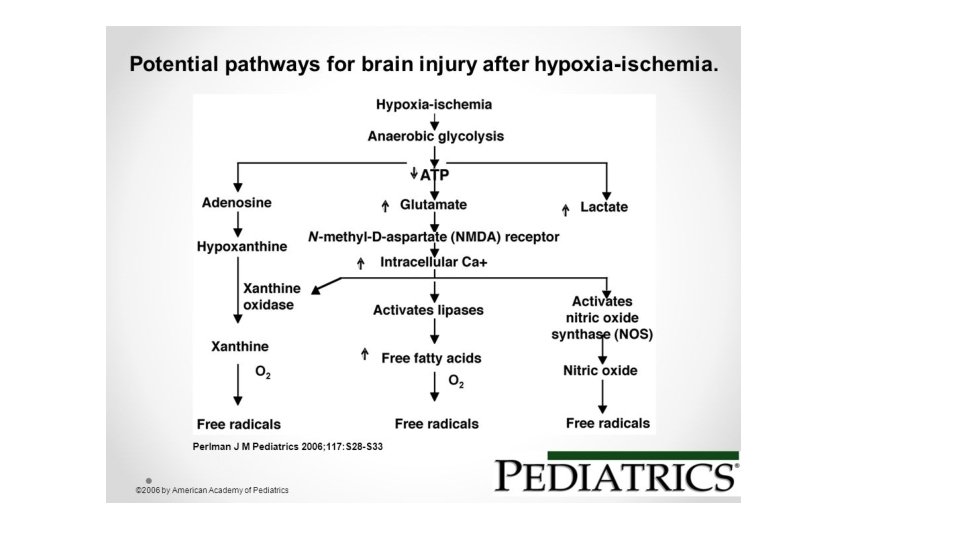
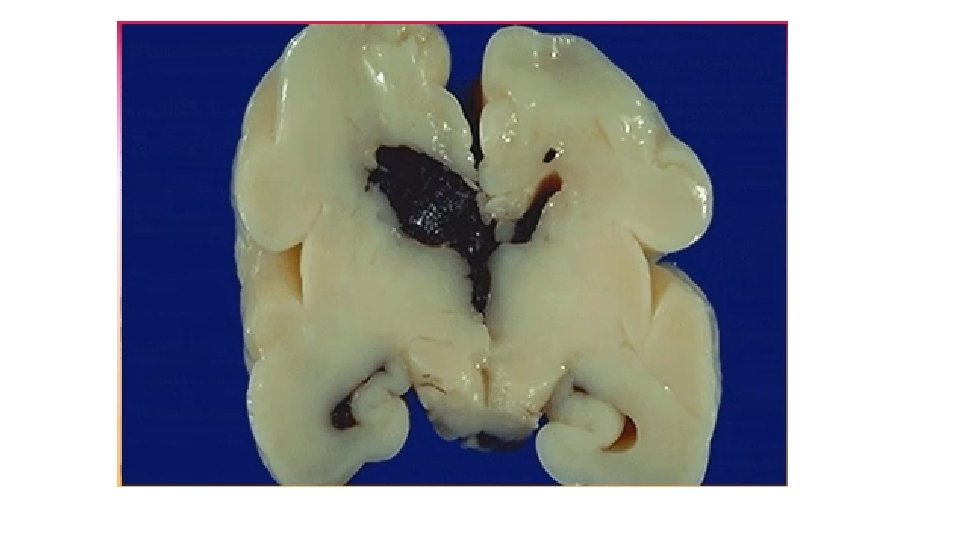
Pathophysiology Acute HIE leads to primary and secondary events: • Primary neuronal damage: (Injury - 6 hrs) • Cytotoxic damage due to failure of microcirculation Inhibition of energyproducing molecular processes ATPas membrane pump failure cytotoxic edema and free radicles formation compromised cellular integrity • [Reduced cerebral perfusion hypoxia and hypoglycemia leading to metabolic acidosis , ischemia and neuronal cell death] • [intracellular derangements increased Intracellular Ca causing edema and cell death. Destruction of protein, membrane lipids and other cellular content leading to neuronal necrosis which can be found hours to days later] • Secondary neuronal damage (6 - 72 hrs) • May extend up to 72 hours or more after the acute insult and results in an inflammatory response and cell necrosis or apoptosis (fueled by reperfusion), reduced growth factor and impairment in protein synthesis, if untreated leads to sustained brain injury.


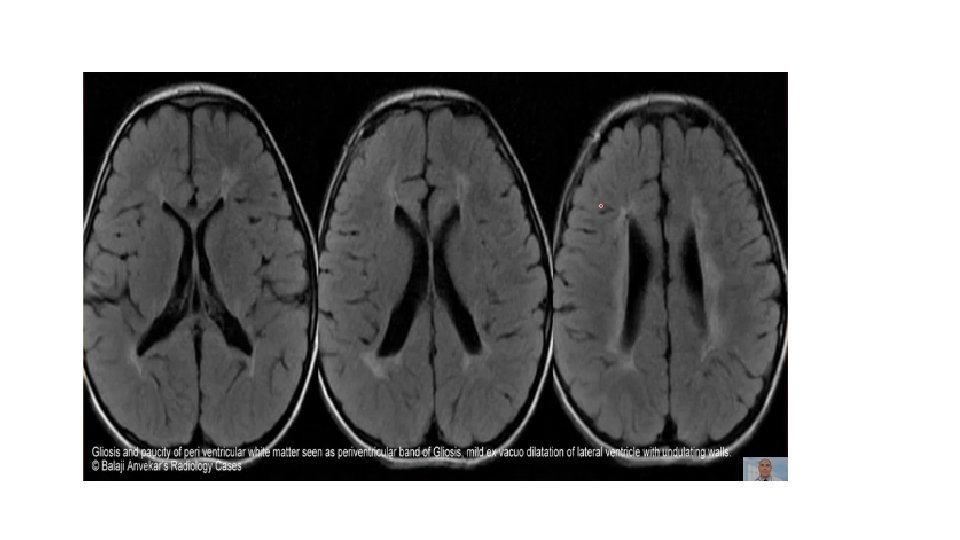
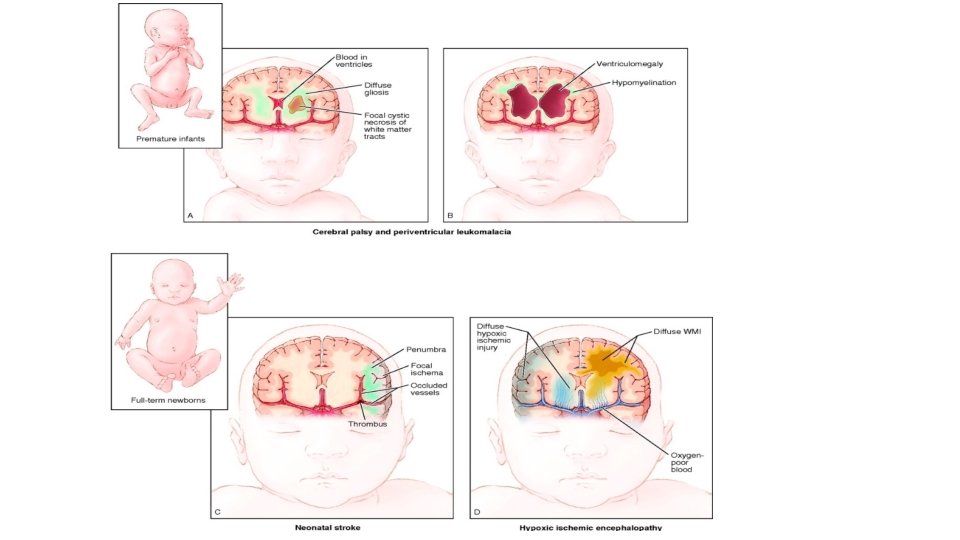
Pathophysiology Gastrointestinal age plays an important role in the susceptibility of CNS structures • < 20 weeks: Insult leads to neuronal hetrotropia or polymicrogyria • 26 -30 weeks: insult affects white matter, leading to polyventricular leukomalacia • Term: Insult affects primarily the gray matter

Pathological correlation of preterm infant with hypoxic ischemic encephalopathy Pathology Clinical sign Periventricular leukomalacia Spastic diaplegia Status marmoratus of basal ganglia Dystonia, choreoathetosis Thalamus Mental retardation Cerebral cortex Mental retardation Pathological correlation of full term infant with hypoxic ischemic encephalopathy Pathology Clinical sign Parasagittal cortical and subcortical neuronal necrosis Spastic quadriplegia, especially arms. Intellectual deficits and cortical atrophy, focal seizures and hemiplegia Cerebellum Ataxia Brain Stem Pseudobulbar palsy

Pathophysiology • CNS factors that influence the distribution of CNS injury • • Cellular susceptibility: (neurons most susceptible) Regional susceptibility: (areas of higher metabolic rate eg. Thalamus) Vascular territories: (watershed areas) Degree of asphyxia

Clinical staging of HIE Sarnat grading scale Good outcome Disability 30% 100% Death 10% 60%

Diagnosis Intrauterine • Growth restriction and • Increased vascular resistances may be the 1 st manifestation of fetal hypoxia. Intrapartum events Absence of an intrapartum sentinel event does not exclude the diagnosis of HIE. -A significant peripartum or intrapartum hypoxic-ischaemic event including: • Uterine rupture • Placental abruption • Cord prolapse • Amniotic fluid embolism • Fetal exsanguination from a vasa praevia or massive feto-maternal hemorrhage

During labor • Variable or late deceleration pattern of continuous heart rate recording, fetal heart rate slows down, and beat-to-beat variability declines. • Fetal scalp blood analysis may show a p. H <7. 20. These signs should lead to the administration of high concentrations of 1. Oxygen to the mother and 2. Immediate delivery to avoid fetal death or CNS damage. At delivery • The presence of yellow, meconium-stained amniotic fluid is evidence that fetal distress had occurred.

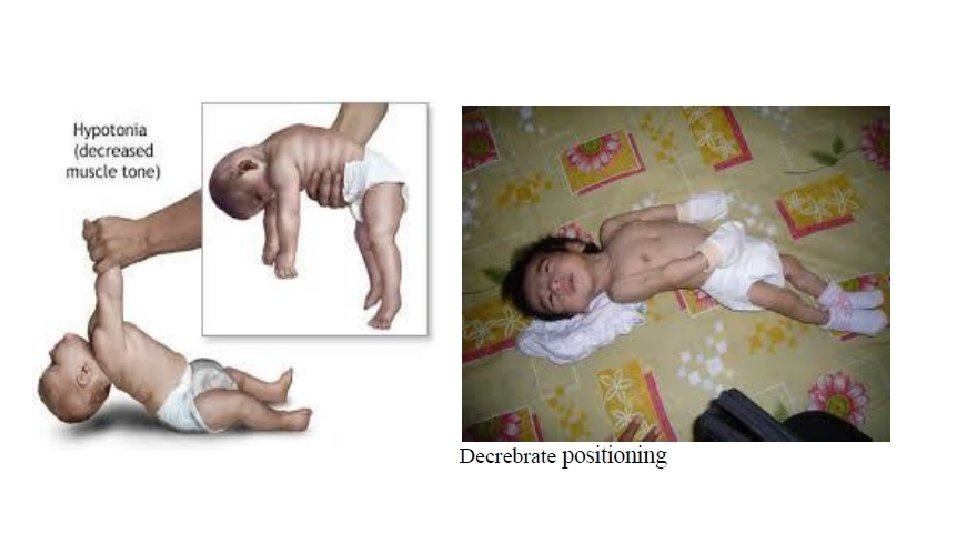
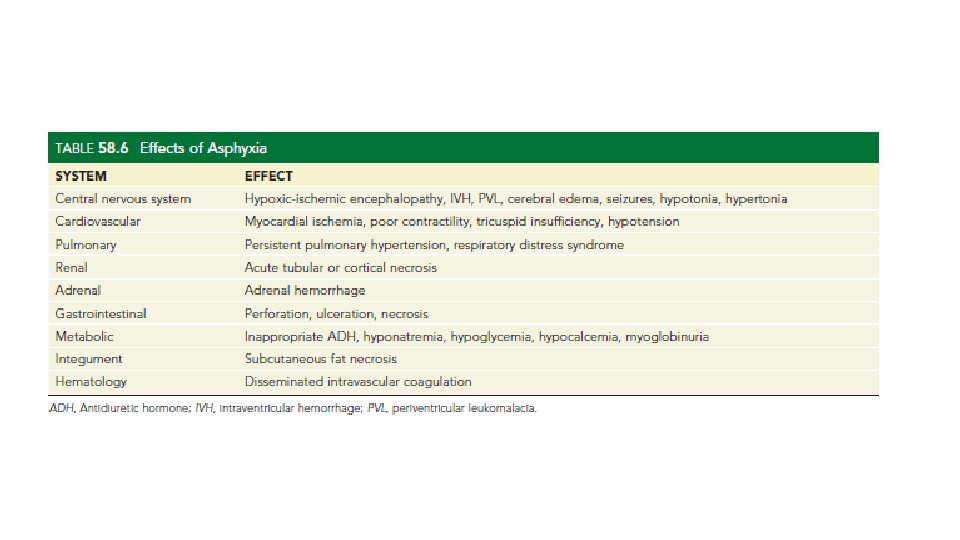
At birth these infants are • Frequently depressed and fail to breathe spontaneously. During the ensuing hours, they • May remain hypotonic or change from hypotonic to hypertonic, or their tone may appear normal. • Pallor, cyanosis, apnea, a slow heart rate, and unresponsiveness to stimulation. Later • Cerebral edema may develop during the next 24 hr and result in profound brain stem depression. During this time, seizure activity may occur; it may be severe and refractory to the usual doses of anticonvulsants. • In addition to CNS dysfunction, systemic hypoperfusion occurs in 80% of cases including; • Heart failure and cardiogenic shock, hypotension, persistent pulmonary hypertension, respiratory distress syndrome, gastrointestinal perforation, hematuria, and acute tubular or cortical necrosis, subcutaneous fat necrosis • Adrenal hemorrhage, inappropriate secretion of antidiuretic hormone, and metabolic derangements, DIC.

Diagnosis • There is no clear diagnostic test. • Abnormal findings on neurological examination in the first few days after birth is the most useful predictor that the brain insult has occurred in the perinatal period. • Essential criteria for diagnosis of HIE: • Fetal umbilical artery acidaemia: p. H less than 7 and/or base excess worse than or equal to minus 12 mmol/L. • Apgar score of less than or equal to 5 at 5 and 10 minutes. • Examination consistent with mild, moderate or severe encephalopathy. • Onset of multisystem organ failure which may include renal injury, hepatic injury, hematologic abnormalities, cardiac dysfunction, metabolic derangements, and gastrointestinal injury.

APGAR SCORE The scores are broken down as follows: • 1 -3 points: Critically low • 4 -6 points: Below normal • 7+ points: Normal APGAR score

Laboratory studies

Neuroimaging • Cranial Ultrasound: not the best in assessing abnormalities in term infants, echogenicity develops gradually over days. • Convenient, noninvasive, low-cost and non –radiation screening examination of the hemodynamically unstable neonate at the bedside/ preterm infant. • Doppler study and resistive index (RI) provide additional information on cerebral perfusion. • To rule out hemorrhagic lesions.

• CT: least sensitive for detecting changes in HIE because of poor parenchymal contrast resolution due to: -High water content in the neonatal brain. -High protein content of the cerebrospinal fluid. Diffuse cortical swelling and hypoattenuation in the white matter • To rule out focal hemorrhagic lesions or large arterial ischemic strokes. • When MRI is not available or prevented due to clinical disability. Loss of gray white differentiation and injury to basal ganglia is detected in severe HIE

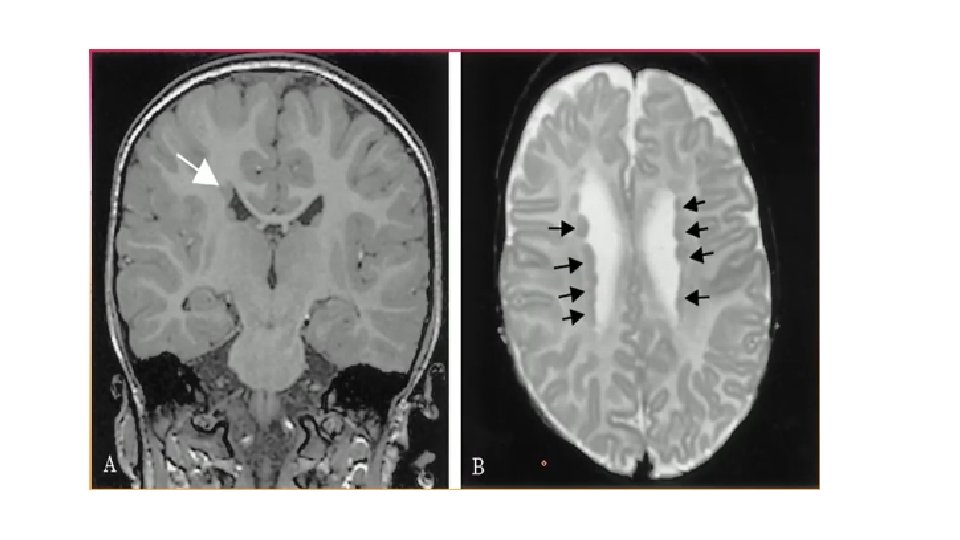
• MRI: Most appropriate technique and is able to show different patterns of injury. • Presence of signal abnormality in the internal capsule later in the first week has a very high predictive value for neurodevelopmental outcome. • Ischemic injury generally results in T 1 hypointensity &T 2 hyperintensity (white matter)due to ischemia induced edema.

• Diffusion weighted sequences obtained in the first 3 -5 days following a presumed sentinel event are optimal for identifying acute injury.

Standard EEG • Generalized depression of the background rhythm and voltage with varying degrees of superimposed seizures are early findings. • EEG characteristics associated with abnormal outcomes include: A) Background amplitude of Less than 30 MV. B) Interburst interval of more than 30 seconds. C) Electrographic seizures. D) Absence of sleep-wake cycle at 48 hours.
 • When performed early, it may reflect dysfunction rather than")
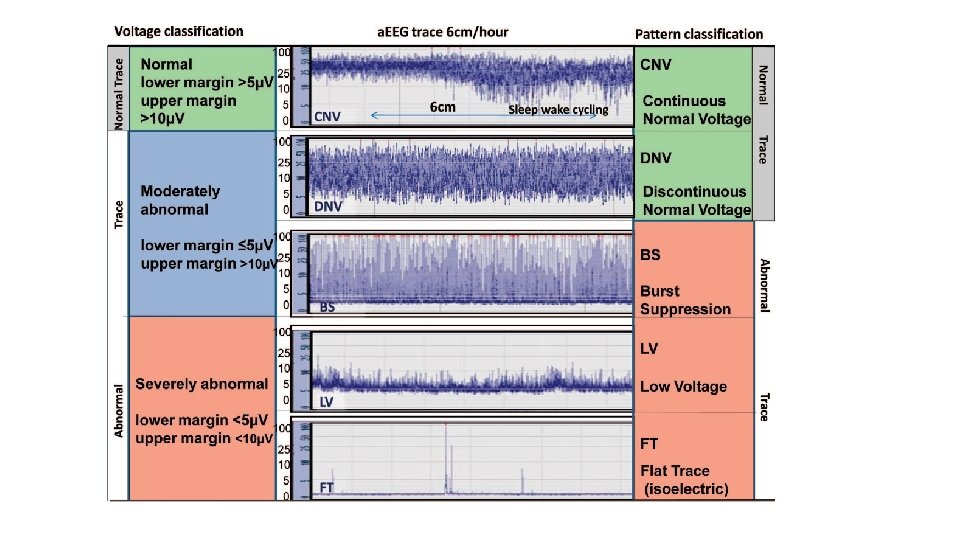
Amplitude-integrated EEG (a. EEG) • When performed early, it may reflect dysfunction rather than permanent injury. • Most useful in infants who have moderate to severe encephalopathy - Discontinuous tracing characterized by a lower margin below 5 m. V and an upper margin above 10 m. V - Burst suppression pattern characterized by a background with minimum amplitude (0 -2 m. V) without variability and occasional high voltage bursts (>25 m. V) - Continuous low voltage pattern characterized by a continuous low voltage background (< 5 m. V) - Inactive pattern with no detectable cortical activity - Seizures usually seen as an abrupt rise in both the lower and upper margin • Marginally abnormal or normal a. EEG is very reassuring of good outcome. • Severely abnormal a. EEG in infant with moderate HIE raises the probability of death or severe disability from 35% to 75%.

Evoked Potentials • Brainstem auditory evoked potentials, visual evoked potentials and somatosensory evoked potentials can be used in full-term infants with HIE. • More sensitive and specific than a. EEG alone. • However, not as available as a. EEG and there is a lack of experience among neurologists • Therefore a. EEG is preferred because of easy access, application and interpretation

Histology • Watershed infarctions secondary to global hypoperfusion.

Complications • Brain injury • Stroke • Cerebral palsy • Epilepsy, seizures • Severe hearing impairment • Blindness and vision impairment • Problems in learning, thinking and speaking/ cognitive deficit • Problems in walking and coordination/ developmental delay

Management
")
Initial Resuscitation and Stabilization • Delivery room management follows standard Neonatal Resuscitation Program (NRP) guidelines. Pay attention to appropriate oxygen delivery, perfusion status, and avoidance of hypoglycemia and hyperthermia. • Resuscitation with room air versus 100% oxygen in the delivery room. • International Liaison Committee on Resuscitation (ILCOR) recommendations include initiating neonatal resuscitation with concentrations of oxygen between 21100%

Supportive Care • Most infants with severe hypoxic-ischemic encephalopathy need ventilatory support during first days of life. • The role of mechanical ventilation is to maintain the blood gases and acidbase status in the physiological ranges and prevent hypoxia, hypercapnia, and hypocapnia. • Infants with hypoxic-ischemic encephalopathy are also at risk for pulmonary hypertension and should be monitored. Nitric oxide (NO) may be used according to published guidelines.
 above 35 -40")
Perfusion and Blood Pressure Management • A mean blood pressure (BP) above 35 -40 mm. Hg is necessary to avoid decreased cerebral perfusion. • Hypotension is common in infants with severe hypoxic-ischemic encephalopathy and is due to myocardial dysfunction, capillary leak syndrome and hypovolemia. • Dopamine or dobutamine can be used to achieve adequate cardiac output in these patients. (Avoiding iatrogenic hypertensive episodes is also important. )

Fluid and Electrolytes Management • Prophylactic theophylline given early after birth helps in reducing renal dysfunction. • A single dose of theophylline (5 -8 mg/kg) given within 1 hour of birth resulted in: (1) Decreased severe renal dysfunction (2) Increased creatine clearance (3) Increased glomerular filtration rate (GFR) (4) Decreased b 2 microglobulin excretion. • Avoid hypoglycemia and hyperglycemia because both may accentuate brain damage.
 • Single or 2 channel (right and")
Start CFAM ( Cerebral function analysis monitoring) • Single or 2 channel (right and left hemispheres) machines available • Display raw EEG and a compressed amplitude integrated recording • Pattern of EEG is used for classification of background activity • Normal CFAM (EEG) recording (term infants): Lower margin <= 5 when awake , upper margin >=10 Evidence of sleep wake cycling , no seizures.

Treatment of Seizures • Hypoxic-ischemic encephalopathy is the most common cause of seizures in the neonatal period. • Phenobarbital has been shown to be effective in only 29 -50% of cases. (20 mg/kg) • Benzodiazepines particularly lorazepam may offer some additional efficacy. (0. 1 mg/kg)
 • Has become standard of care. • Cooling is achieved")
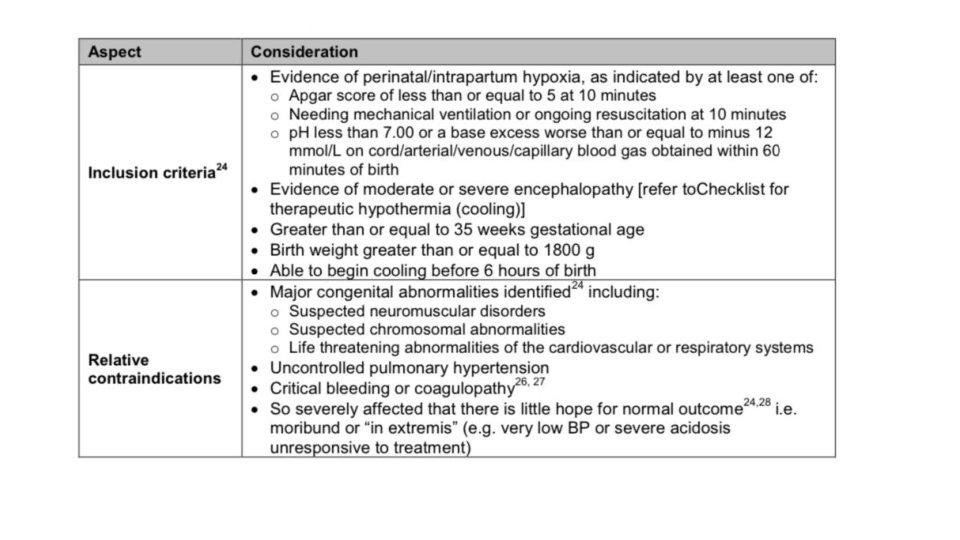
Therapeutic hypothermia (avoid hyperthermia) • Has become standard of care. • Cooling is achieved using a temperature controlled mattress or wrap. • Eligible infants have their core(rectal) temperature lowered to 33 -34 C within 6 h of insult. • Hypothermia is maintained for 72 h before re-warming.

• Head cooling is not used anymore
 Reduced metabolic rate and energy depletion (2) Decreased excitatory transmitter release")
Hypothermia principles (1) Reduced metabolic rate and energy depletion (2) Decreased excitatory transmitter release (3) Reduced alterations in ion flux (4) Reduced apoptosis due to hypoxic-ischemic encephalopathy (5) Reduced vascular permeability, edema, and disruptions of blood-brain barrier functions
")
Diet • In most cases the infant is restricted to nothing by mouth (NPO) during the first 3 days of life or until the general level of alertness and consciousness improves. NPO due to risk of necrotizing enterocolitis because of ischemia. • Infants undergoing hypothermia therapy should remain NPO until rewarmed. Enteral feeds should be carefully initiated and the use of trophic feeds is initially advisable (about 5 m. L every 3 -4 h). • Infants should be monitored carefully for signs and symptoms of necrotizing enterocolitis for which infants with perinatal asphyxia are at high risk.

Surgical care • In cases of posterior cranial fossa hematoma, surgical drainage may be lifesaving if no additional pathologies are present. Further Inpatient Care • Close physical therapy and developmental evaluations are needed prior to discharge in patients with hypoxic-ischemic encephalopathy (HIE).

Further Outpatient Care • Follow-up is to detect impairments and promote early intervention for those infants who require it. • Growth parameters including head circumference should be closely monitored in all infants with hypoxic-ischemic encephalopathy. • In infants diagnosed with moderate-to-severe hypoxic-ischemic encephalopathy with either abnormal neurologic examination findings or feeding difficulties, intensive follow-up is recommended. include follow-up by developmental pediatrician and pediatric neurologic. • Follow up in the first two years to monitor complications, cooling effectiveness and development.
, neuroprotective qualities, such as affecting other")
New in treatment • Xenon Gas (inhaled anesthetic), neuroprotective qualities, such as affecting other ion channels and reducing neurotransmitter release in general. Approved and used with cooling. • Erythropiotine Neuroprotection against apoptosis and anti-inflammatory effect (not approved yet. ) • Melatonin Anti-inflammatory effect (no studies yet) • Stem cell transplant May increase levels of brain trophic factors and anti-apoptotic factors, decrease inflammation, preserve endogenous tissue, support replacement of damaged cell (no studies yet)

Differential diagnosis: • • Metabolic Abnormalities Congenital Abnormalities Meningitis Hypoglycaemia Hyperbilirubinaemia Chronic Placental Insufficiency Other Causes Of Seizures/Encephalopathy In Neonates Include Intracranial Haemorrhage, Perinatal Stroke, Drug Withdrawal

Prognosis • Depends on the severity of injury and gestational age of the infant. • Term infants with mild encephalopathy generally have good prognosis and show complete recovery, 20% of infants may die in the neonatal period and 25% may develop significant neurological deficit. • EEG at about 7 days that reveals normal background activity is a good prognostic sign. • Persistent feeding difficulties due to abnormal tone of the muscles of sucking and swallowing also suggest significant CNS damage. • Poor head growth during the postnatal period and the first year of life is a sensitive finding predicting higher frequency of neurologic deficits.
 10 minute apgar score Need for")
Poor predictive variables for death/disability Low (0 -3) 10 minute apgar score Need for CPR in the delivery room Delayed onset >= 20 minutes of spontaneous breathing Severe neurological signs (coma, hypotonia, hypertonia) Seizure onset <= 12 hours or difficult to treat Severe prolonged (7 day) EEG findings including burst suppression pattern, Increase lactate on MRS within 24 hours of life • Prominent MRI basal ganglia/ thalamic lesions • Abnormal neurologic exam >= 14 days • Oliguria or anuria > 24 hours • • •

THANK YOU • https: //www. bing. com/videos/search? q=HIE&&view=detail&mid=BF 949 E 82 E 173 CE 7 E 03 F 8&&FORM=VRDGAR
- Slides: 54