HYPOTHYROIDISM HYPOTHYROIDISM Etiology Primary Hashimoto thyroiditis radio active






, not liothyronine (T 3) because rapid absorption, short")






 Hakaru Hashimoto (1912) 4 patients chronic disorder of the thyroid")







 antibody Anti-thyroglobulin antibody Positive")




, painless, progressive anterior neck mass, •")

 preceded URT infection, coincidence")











 10 -20% risk of suspicious cytology, therefore")
















- Slides: 60
HYPOTHYROIDISM
HYPOTHYROIDISM Etiology • Primary: Hashimoto thyroiditis, radio active iodine therapy for graves’ disease, subtotal thyroidectomy, subacute thyroiditis, iodide deficiency • Secondary : Hypopituitarism due to pituitary adenoma • Tertiary : Hypothalamic disfunction (rare)
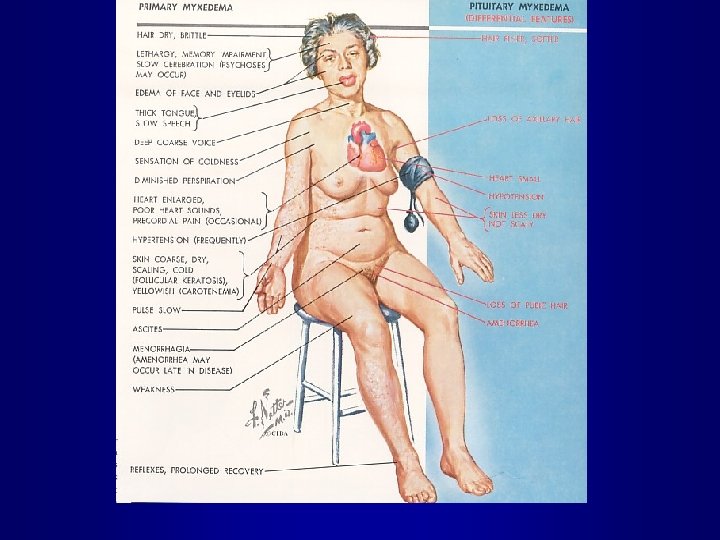
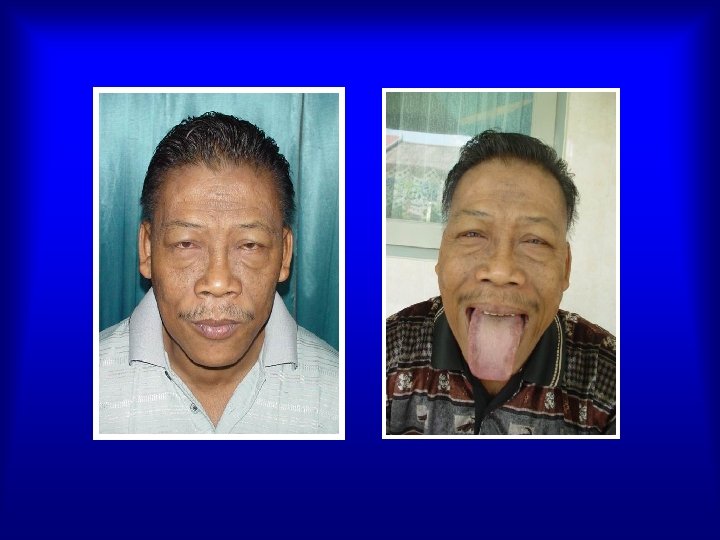
HYPOTHYROIDISM Clinical finding • Incidence : Various causes depending geographic & enviromental factors • Hashimoto thyroiditis the most common cause of hypothyroidism • Newborn infants (Cretinism) • Fatigue, coldness, weight gain, constipation, menstrual irregularities, muscle cramps
HYPOTHYROIDISM • Physical findings: Cool, rough n dry skin, puffy face and hands, hoarse voice, slow reflexes Cardiovascular sign: bradycardia, diminished CO, low voltage QRS, cardiac enlargement Pulmonary function: Respiratory failure Intestinal paralysis slowed , chronic constipation, ileus Renal function: decresed GFR, renal impairement Haematology : anemia, CNS symptoms: fatigue, inability to concentrate
Pituitary- thyroid relationships in primary hypothyroidism TRH Dopamine Hypothalamus Somatostatin TSH Tissues T 3, T 4 THYROID Pituitary
Complication • Myxedema coma end stage of untreated hypothyroidism, cause radiotherapy in Graves’ Disease • Myxedema & Heart disease CAD • Hypothyroidism Neuropsychiatric disease depression, confuse, paranoid, manic
Treatment Hypothyroidism • Levothyroxine (T 4), not liothyronine (T 3) because rapid absorption, short half life, transient effect. Dosage : 1 x in the morning to avoid insomnia 0. 05 mg-0. 2 mg/d • Mixedema coma ICU, intubation & mechanical ventilation, Treat infection, heart failure, IV drips with caution, levothyroxin IV
EXAMPLES OF THYROID DISEASES 1° Hypothyroidism Hyperthyroidism www. hsc. missouri. edu/~daveg/thyroid/thy_dis. html
Definition • Thyroiditis heterogenous group of inflamatory disorders the thyroid gland • Etiologies range from autoimmune to infectious origins • Clinical course Acute, subacute, or chronic. Can be euthyroid, transient phase thyrotoxicosis and / or hypothyroidism. Painless or painfull
Classification of thyroiditis I. Autoimmune thyroiditis Chronic autoimune thyroiditis Hashimoto’s thyroiditis Atrophic thyroiditis Focal thyroiditis Juvenile thyroiditis Silent thyroiditis / Postpartum thyroiditis II. Subacute thyroiditis III. Acute suppurative thyroiditis IV. Riedel’s thyroiditis
Classification of thyroiditis Hystologic classification Synonims Chronic lymphocytic thyroiditis, Hashimoto’s thyroiditis Subacut lymphocytic thyroiditis, Subacute lymphocytic Granulomatous Postpartum thyroiditis, Sporadic painless thyroiditis Subacut granulomatous thyroiditis De Quervains thyroiditis Microbial inflamatory Invasive fibrosis Suppurative thyroiditis Acute thyroiditis Riedel’s struma Riedel’s thyroiditis
Terminology for Thyroiditis. Type Synonim Hashimoto’s thyroiditis Chronic lymphocytic thyroiditis Chronic autoimmune thyroiditis Lymphadenoid goiter Painless postpartum thyroiditis Postpartum thyroiditis Subacute lymphocytic thyroiditis Painless sporadic thyroiditis Silent sporadic thyroiditis Subacute lymphocytic thyroiditis Painful subacute thyroiditis Subacute thyroiditis de Quervain’s thyroiditis Giant-cell thyroiditis Subacute granulomatous thyroiditis Pseudogranulomatous thyroiditis
Terminology for Thyroiditis. Type Synonim Suppurative thyroiditis Infectious thyroiditis Acute suppurative thyroiditis Pyogenic thyroiditis Bacterial thyroiditis Drug-induced thyroiditis (amiodarone, lithium, interferon alfa, interleukin-2) - Riedel’s thyroiditis Fibrous thyroiditis
Hashimoto’s thyroiditis (Chronic thyroiditis) Hakaru Hashimoto (1912) 4 patients chronic disorder of the thyroid diffuse lymphocytic infiltration, fibrosis, parenchymal atrophy, and eosinophilic change in some acinar cells Dr Hakaru Hashimoto
Hashimoto’s thyroiditis Hashimoto thyroiditis is the most common cause of hypothyroidism & goiter in the United States Statosky J et al. Am Acad of Family physicians 2000; 61: 1054
Hashimoto’s thyroiditis Etiology & pathogenesis HT is immunologic disorder which lymphocytes become sensitized to thyroidal antigens and autoantibodies are performed. Thyroid antibodies in HT are: 1. Thyroglobulin antibody (Tg Ab) 2. Thyroid peroxidase antibody (TPO Ab)-AMA 3. TSH Receptor blocking antibody (TSHR Ab block)
Clinical Manifestation Hashimoto’s Thyroiditis Symptom & Signs HT usually presents with goiter , euthyroid or mild hypothyroidism. Sex distribution : F/M 4: 1 Painless & patients may be anware of the goiter
Laboratory findings • T 4 N/ low, TSH will be elevated. RAIU may be high, normal or low • Tg Ab & TPO Ab positif • Fine needle aspiration biopsy large infiltration lymphocytes Hurtle cells
Diagnostic procedures • Test of thyroid autoimmunity: TPOAb 95% + in Hashimoto thyroiditis & 90% Atrophic thyroiditis Tg. Ab less frequently + Diagnostic specificity of thyroid antibody tests is not absolute. • Test for thyroid function TSH, f. T 4 • RAIU: normal, low or high. • USG: diffusely reduced echogenecity. • FNAB not necessary, excep. rapidly enlarging goiter
Diagnosis of Hashimoto’s thyroiditis Diffuse goiter Anti microsomal (or TPO) antibody Anti-thyroglobulin antibody Positive Negative Hashimoto’s thyroiditis US Biopsy Positive Negative Other diseases* Sign symptom of hypothyroidism *Simple goiter, adenomatous goiter etc
Treatment Hashimotos thyroiditis
Treatment • Goiter small & asymptomatic not require therapy • Levo-thyroxine is given over hypothyroidism to supress TSH & decreased serum thyroid antibody. Levo-thyroxine in euthyroid, still controversial
Treatment • Corticosteroids : regression pain, reduction in size of the goiter, thyroid antibody , not recommended in benign disease. • Surgery indicated pain, cosmetic, or pressure symptoms after levothyroxine and corticosteroid therapy.
Riedel’s thyroiditis • Rare 1, 06/100. 000, middle age or elderly women • Etiology unknown (autoimmune process or primary fibrotic disorder) • Characterized fibrosis replaces normal thyroid parenchyma, 1/3 cases multifocal fibrosclerosis
Riedel’s thyroiditis • Thyroid fibrosis (stony hard, woody), painless, progressive anterior neck mass, • Generalized fibrosing (1/3 patients), pressure symptoms laryngeal nerve paralysis or hypoparathyroidism (rare) • Usually euthyroidism, hypothyroidism (30%) • Laboratorium : non spesific • USG/CT-Scan inconclusive • Difinitive diagnosis open Biopsy
Riedel’s thyroiditis • Treatment: Corticosteroids medical treatment of choice Tamoxipen, methotrexate inhibitor fibroblast proliferation ( early stages) Levothyroxine hypothyroidism Surgical care diagnosis, relieving tracheal compression • Mortality asphyxia (6 -10%), extrathyroidal fibrotic lesions may complicate the prognosis
Subacute thyroiditis • Cause unknown ( viral infection (? ) preceded URT infection, coincidence viral disease (mumps, measles, Echo virus, adeno virus, epst. Barr virus, influenza) • Women : Men (3 -5: 1) • Onset: 20 -60 yr • Summer
Subacute thyroiditis • Palpation thyroid: enlarged, asymetrical, nodul, firm, tender & painful. • Thyrotoxicosis during inflamatory phase euthyroidism hypothyroidism euthyroidism (4 th phases) • Laboratorium: ESR increase, leukocyt N/ increase, f. T 4, , TSH, RAIU • Recovery 4 -6 months, spontaneous remitting
Changes in serum T 4 & Radiactive iodine uptake in patients with subacute Thyroiditis 24 -hour 131 I uptake % T 4 ug/d. L 20 T 4 40 15 30 10 20 5 10 0 Phase : Weeks: 131 I Hyper 1 0 Eu 4 Hypo 11 Eu - Woolf PD, Daly R : Am J Med 197; 60: 73
Laboratory findings during different phases of subacute thyroiditis Phase T 4 &/T 3 Level TSH level RAIU value Thyrotoxicosis High Low <5% Hypothyroid Low Normal, or high Normal to high Recovery Normal High to normal
Treatment Subacute thyroiditis • Symptomatic: Acetaminophen 4 X 0, 5 g, NSAID or glucocorticoid (prednison 3 X 20 mg (7 -10 days) • Betablockers symptoms of thyrotoxicosis • L-thyroxine 0. 1 -0. 15 mg /daily hypothyroid phase. Long-term L-thyroxine permanent hypothyroidism (10%) • Antibiotics no value • Thyroidectomy rarely
Clinical Differentiating of the Subtype Thyroiditis NECK PAIN N 0 YES PRESENTING SYMPTOMS RAIU INCREASED MICROBIAL INFLAMMATORY THYROIDITIS HYPERTHYROIDISM DECREASED SUBACUTE GRANULOMATOUS THYROIDITIS RAIU GRAVES DISEASE HYPOTHYROIDISM CHRONIC LYMPHOCYTIC THYROIDITIS SUBACUT LYMPHOCYTIC THYROIDITIS Statosky J et al. Am Acad of Family physicians 2000; 61: 1054
Acute suppurative thyroiditis • Rare, serious, bacterial inflamatory disease, children, 20 -40 yr, sex ratio 1: 1 • Etiologi: Infectious: Staph. aureus, strep. pyogenes, strep. pneumonia, esch. coli, pseudomonas aeruginosa • Infection by hematogenous, direct trauma
Symptoms & signs • Neck pain, warm, tenderness, the neck unable to extend • Dysphagia, dysphonia, referred to ear, mandibula, lymphadenopathy • Systemic manifestation: fever, chills, tachycardia, malaise • Palpation: unilateral, erythematous
Acute suppurative thyroiditis • Thyroid function : Euthyroidism • Laboratorium : TPO antibodies absent, ESR high, PMN leukocytosis • 24 -hour 123 I uptake normal • FNA Biopsy: purulent material • Treatment: antibiotics or surgical drainage
Chronic-pyogenic thyroiditis • Etiology : Salmonella typhosa, syphilis, tuberculosis, echinococcus, actinomyces • Symptoms: Suppurative, non suppurative • Treatment: antibiotic, drainage
Thyroid nodules & Thyroid cancer
Thyroid nodules - prevalence • Thyroid nodules common, increase with age • 30 -60% of thyroids have nodules at autopsy • Palpation: 5 -20% ( > 1 cm ) • USG : 15 -50% ( >2 mm )
Diagnostic approach • Fine Needle Aspiration (FNA) 10 -20% risk of suspicious cytology, therefore thyroid surgery 95% of histology will be benign, and surgery “unnecessary” • Isotop Scann(CT) rarely used for evaluation 80% of nodules are “cold” small cold nodules may be missed COLD nodules may be malignant • Ultrasonography (USG)
Diagnostic approach - ultrasound Identifies solid vs cystic nodules Identifies MNG May aid FNA Does not exclude malignancy
Diagnostic approach - other tests Calcitonin very high results diagnostic for MTC risk of borderline false positives not for routine use Thyroglobulin not helpful for exclusion of carcinoma: overlap with benign disease best for follow-up after thyroidectomy
Thyroid nodules & Thyroid cancer • In 95% of cases , thyroid cancer presents as a nodule or lump in the thyroid nodul thyroid. • Thyroid nodule extremely common, particularly women. Prevelance in USA 4% in adult population. F: M ratio 4: 1. • Thyroid cancer rare. Incidence 0. 004% per year
Diffrentiation benign & Malignant lesions • History : Family history of goiter suggests benign disease, endemic goiter • Physical characteristics: Benign: older age, woman, soft nodule, multi nodular goiter. Malignant: Children, young, male, solitary, firm nodule, vocal cord paralysis, firm lymph nodes, distant metastasis
Malignant thyroid Carcinoma • • • Papillary Carcinoma Folliculare Carcinoma Medullary Carcinoma Anaplastic Carcinoma Lymphoma 75 % 16 % 5% 3% 5 -10 %
Management of the solitary nodule
Treatment • Thyroidectomi • Jodium 131 Radioactive • Thyroxine supression
FNA POSITIF MALIGNANCY Differenteated Under 2 cm, no invasion Lobectomy and isthmusectomy Levothyroxine for life Undifferenteated Over 2 cm, or multicentric, or invasive Near total thyroidectomy and modified neck dissection Liothyronine, 75 -100 mcg/d for 3 mos, discontinue 2 week. Low iodine diet Scan with 2 -5 m. Ci 131 I Negatitive scan Levothyroxine for life No recurence cure Recurrence + - Scan Local removal to prevent obstruction (palliative therapy) X-ray therapy or chemotherapy (or both) plus levothyroxine replacement therapy Repeat after 12 months Positive scan 50 -150 m. Ci 131 I (therapeutic dose) X Ray therapy or chemo therapy (or both)
Treatment of thyroid cancer • Papillary cancer – < 1. 5 cms – > 1. 5 cms Lobectomy & isthmusectomy Total thyroidectomy • Follicular cancer • Hurthle • Medullary Total thyroidectomy & central neck dissection