Hypothalamic Anovulation By Dr Mohammad Wali Naseri MD

Hypothalamic Anovulation By : Dr Mohammad Wali Naseri MD Associate Prof of Internal Medicine, Division of Endocrinology Metabolism and Diabetes, Kabul University of Medical Sciences

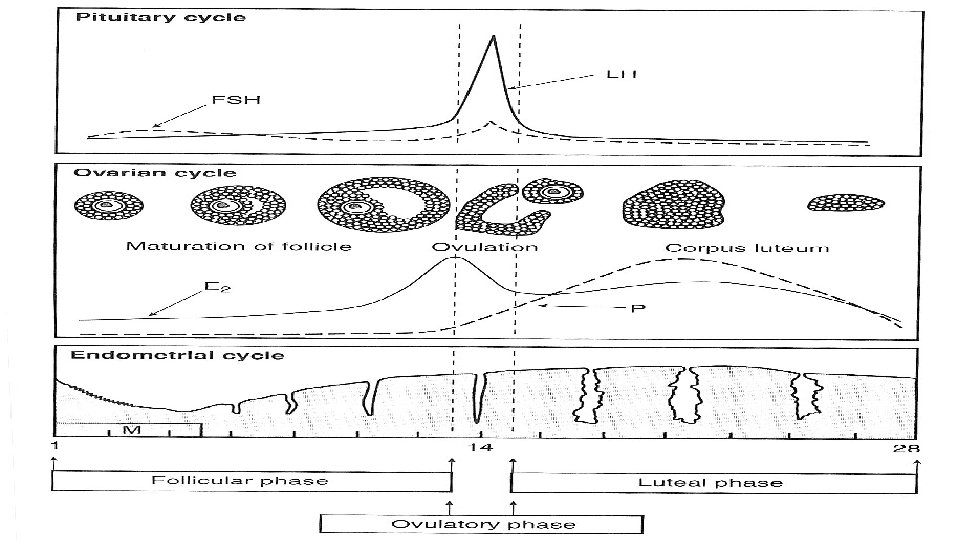
Hypothalamic pituitary gonadal axis

Hypothalamic pituitary gonadal axis

WHO Classification of ovulation disorders Group 1 Hypothalamic pituitary failure (hypothalamic amenorrhea or hypogonadotropic hypogonadism) • This group of disorders is characterized by low gonadotrophins, normal prolactin and low estrogen, and it accounts for about 10% of ovulatory disorders

WHO Classification of ovulation disorders Group 2 Hypothalamic pituitary dysfunction • This group, which is characterized by gonadotrophin disorder and normal estrogen, accounts for about 85% of ovulatory disorders

WHO Classification of ovulation disorders Group 3 Ovarian failure • This group, which is characterized by high gonadotrophins with hypogonadism and low estrogen, accounts for about 4– 5% of ovulatory disorders

Background Definition: Infertility: 1 year unprotected coitus without conception 10 -15% couples affected Etiology Couples: ○ ○ ○ 35% Tubal and pelvic pathology 35 % Male problems 15% Ovulatory dysfunction 10% Unexplained 5% unusual causes

Background • Etiology • Women: • • 40% Tubal and pelvic pathology 40% Ovulatory dysfunction 10% Unexplained Infertility 10% Unusual causes • Normal couple: • 25 -30% chance of pregnancy per ovulatory cycle • Fertility decreases with age

Infertility Time of Exposure 3 months 6 months 1 year 18 months % Pregnant 60% 70% 85% 90%

Approach to Infertility • DDX • Tests/Inv • Dx • Rx
")
Female Infertility • Fecundability: probability of achieving a pregnancy within 1 menstrual cycle (25%) • Fecundity: ability to achieve a live birth within 1 menstrual cycle (6%)

Pathophysiology • Production • Storage • Delivery

Pathophysiology • Production: • Hypothalamus • Pituitary • Ovary

Hypothalamic-Pituitary-Gonadal Axis

Causes • Hypothalamus: • • • Stress Exercise Eating disorders Psychogenic Congenital/genetic: Kallman’s syndrome (hyposmia & hypoplasia olfactory lobes of brain) Starvation/stress or severe illness Tumors (craniopharyngioma, metastatic tumor) Head injury Inflammation (sarcoidosis) Infection (tuberculosis) XRT Drugs

Evaluation History: Age GTPAL Regulatory of period Prolactin S/S Thyroid S/S Infections, Surgeries Medication, Smoking, Ethanol Medical history Previous investigations
 Abdomen (masses, scars) Vaginal")
Physical Examination: • • • Visual Field Thyroid Breast (milk) Abdomen (masses, scars) Vaginal (abnormalities) Bimanual (Uterus, masses)

Lab Investigations Blood work: TSH PRL D 3 FSH D 3 LH Luteal phase Progesterone Imaging: Pelvic Ultrasound HSG Diagnostic Laparoscopy (later)

Treatment • Treat the underlying cause • Medical • Surgical

Treatment of WHO Group I ovulation disorders Treatment options include: • Lifestyle interventions (normalizing weight and exercise) • Pulsatile gonadotrophin-releasing hormone (Gn. RH) (‘Gn. RH pump’) • Gonadotrophins (human menopausal gonadotrophin [h. MG]).

Treatment of WHO Group II ovulation disorders Options for treatment include: • Weight loss • Medical treatment • Second-line treatments including laparoscopic ovarian diathermy (LOD) and injectable gonadotrophin ovulation induction • Assisted conception (usually in vitro fertilization [IVF])

Take Home Points • DDx – Hx – Px – Inv - Rx • Age is important factor female • Hypothalamic-Pituitary-Gonadal axis central in working up both male and female infertility • Investigations: • Male: Sperms • Female: Tubes (HSG) + Ovaries (FSH, LH, PRL, TSH)

Thank You
- Slides: 25