Hypoparathyroidism Hasan AYDIN MD Endocrinology and Metabolism Yeditepe

Hypoparathyroidism Hasan AYDIN, MD Endocrinology and Metabolism Yeditepe University Medical Faculty

Hypoparathyroidism • Clinically – Symptoms of neuromuscular hyperactivity • Biochemically – hypocalcemia, – hyperphosphatemia, – diminished to absent circulating i. PTH.
 • Familial • Idiopathic • Functional")
Etiology • Surgical (most common) • Familial • Idiopathic • Functional

Etiology Surgical hypoparathyroidism • Most common cause is neck surgery eg. total thyroidectomy Idiopathic hypoparathyroidism • Age of onset is 2 -10 years • Female preponderance • Circulating parathyroid antibodies common

Autoimmune hypoparathyroidism • Component of autoimmune polyglandular syndrome • Associated with primary adrenal insufficiency, mucocutaneous candidiasis • Age of onset 5 -9 years Familial hypoparathyroidism • Autosomal dominant • Mutation in PTH gene leads to defective PTH
 •")
Others • Di George’s syndrome • MEDAC syndrome (multiple endocrine deficiency, autoimmune candidiasis) • HAM syndrome (hypoparathyroidism, Addison's disease, and mucocutaneous candidiasis) • Congenital aplasia of the parathyroids • Iron deposition in the glands • Copper deposition • Aluminum deposition • Infiltration with metastatic carcinoma

Functional Hypoparathyroidism • Long periods of hypomagnesemia – selective gastrointestinal magnesium absorption defects – generalized gastrointestinal malabsorption – alcoholism. • Serum PTH low • Hypocalcemia (Mg is required for PTH release and peripheral action of PTH)

Clinical Features • PTH deficiency leads to hypocalcemia • Effects depend on severity and rate of drop • Neuromuscular features: – Paresthesias (perioral, fingertips) – Muscle weakness and cramps, fasciculations – Tetany (Chvostek’s and Trousseau’s signs)

Signs of Hypocalcemia • Neuromuscular • CNS • CVS • Ophtalmalogical • Skin • Dental • GIS

Neuromuscular Manifestations • Paresthesias • Tetany – Chvostek's sign. – Trousseau's sign • Hyperventilation • Adrenergic symptoms – anxiety, tachycardia, sweating, and peripheral and circumoral pallor • Convulsions – more common in young people: generalized form of tetany followed by prolonged tonic spasms; typical epileptiform seizure • Extrapyramidal signs- Classic parkinsonism

Chvostek’s sign Elicited by tapping over facial nerve causing twitching of ipsilateral facial muscles

Trousseau’s sign Carpal spasm in response to inflation of BP cuff to 20 mm Hg above SBP for 3 min

Clinical Features CNS manifestations – Depression – Irritability – Confusion – Focal or generalized seizures

Clinical Features CVS manifestations – Decreased myocardial contractility – Hypotension – Congestive heart failure • CVS features seen particularly in patients with underlying cardiac disease, or those on digoxin or diuretics • ECG: prolonged QT • Laryngeal or bronchospasm (rare)

Other Clinical Manifestations • Posterior lenticular cataract • Dental manifestations – Abnormalities in enamel formation – Delayed or absent dental eruption – Defective dental root formation with short or blunted roots • Malabsorption syndrome

Diagnosis • Serum Calcium: – Decreased • Serum Phosphorus: – Increased • Serum i. PTH: – Decreased

Serum i. PTH • Increased values in a range appropriate to the degree of hypocalcemia – pseudohypoparathyroidism, vit D deficiency, vit D dependency (end-organ resistance to PTH) – secondary hyperparathyroidism (dietary deficiency of calcium, intestinal malabsorption of calcium, or excessive intake of absorbable phosphate- containing drugs) • Undetectable serum i. PTH – hypoparathyroidism – functional hypoparathyroidism due to hypomagnesemia
 = (measured total calcium")
Laboratory Evaluation • Hypocalcemia – Corrected total calcium (mg/d. L) = (measured total calcium mg/d. L) + 0. 8 (4. 0 - measured albumin g/d. L) • PO 4, Mg, i. PTH, BUN/Cr, 25 (OH) Vit D, 1, 25 (OH) vit D 3, Alk Phos • ECG: prolonged QT interval • Skeletal X-rays • Bone biopsy

Differential Diagnosis Calcium PO 4 PTH 25 -vit D Hypoparathyroidism Normal Pseudohypoparathyroidism Normal /N /N Liver disease Renal disease 1, 25 -Vit D Normal /N

Differential for Hypocalcemia Vitamin D Deficiency – Congenital rickets – Malnutrition – Malabsorption – Liver disease – Renal disease • Acute on chronic RF • Nephrotic syndrome – Hypomagnesemia – Sepsis – Anticonvulsants (phenytoin, primidone) Pseudohypoparathyroidism – PTH resistance Ca Chelation – Hyperphosphatemia – Citrate – Free fatty acids – Alkalosis – Fluoride Poisoning

Treatment • Physiologic replacement of PTH • Pharmacologic doses of vitamin D – (ergocalciferol or its more potent analog dihydrotachysterol, in combination with oral calcium administration) • Diets low in phosphate (restriction of dairy products and meat) and oral aluminum hydroxide gels

Emergency Measures for Tetany • Intravenous calcium (10 -20 ml of a 10% solution of calcium gluconate (40 mg elemental calcium per 10 m. L) • Vitamin D • Oral calcium 200 mg of elemental calcium (as the carbonate salt) every 2 hours and gradually increasing to 500 mg every 2 hours if necessary. • Continuous calcium infusion (500 ml of 5% glucose and water containing 10 ml of 10% calcium gluconate is given over 6 hours initially) • Anticonvulsive agents (phenytoin, phenobarbital)
.")
Severe Hypocalcemia • Hypocalcemia may be profound and resistant to treatment (“bone hunger” syndrome). • 10 g of elemental calcium IV infusion over 24 hours • 1, 25(OH)2 D 3 (calcitriol [Rocaltrol]) in doses ranging from 0. 5 to 2 µg daily

Marked Hypoparathyroidism • Long-term vitamin D treatment – dihydrotachysterol ( 1 mg is equivalent to about 120, 000 units or 3 mg of vitamin D 2), 4 mg/d as a single dose for 2 days, then 2 mg/d for 2 days, then 1 mg/d – Ergocalciferol (vitamin D 2 40, 000 units/mg). – Cholecalciferol metabolites calcifediol and calcitriol • Calcium- total (dietary and supplemental) intake of 1 g or more of the element daily in patients under age 40 and 2 g in patient over age 40.

Complications • Hypercalcemia • Hypercalciuria

PTH Resistance Syndromes

Pseudohypoparathyroidism • Abnormal target tissue responses – receptor binding of the hormone – final expression of the cellular actions of PTH • Resistance to several other hormones (vasopressin, glucagon). • Secretion of a biologically inert form of PTH, • Circulating inhibitors of PTH action, • An intrinsic abnormality of PTH receptors, • Autoantibodies to the PTH receptor,

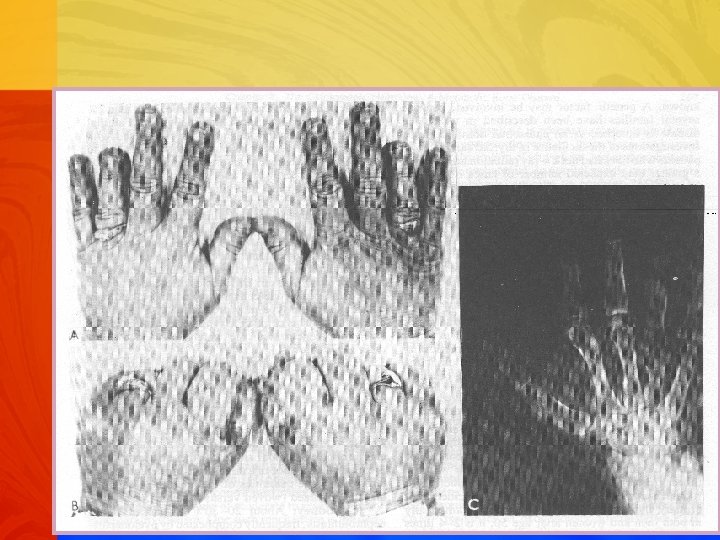
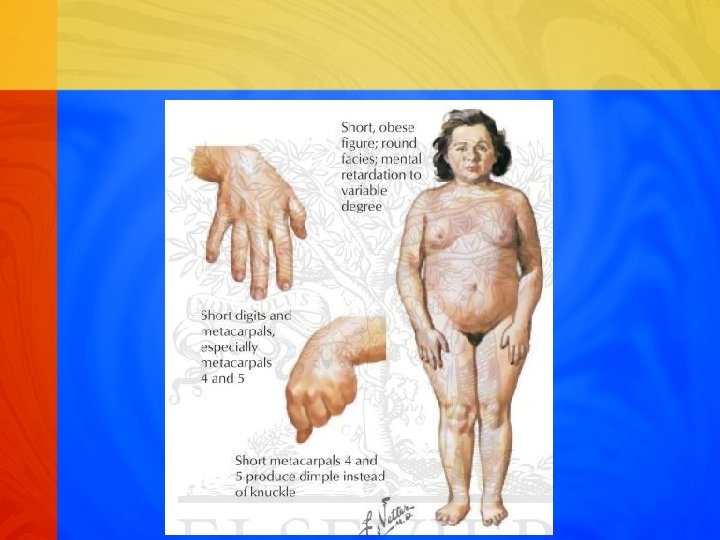
Pseudohypoparathyroidism • Rare familial disorder • Target tissue resistance to PTH • Hypocalcemia, hyperphosphatemia • Increased parathyroid gland function • Short stature and short metacarpal and metatarsal bones.

Pseudopseudohypoparathyroidism • Developmental defects without biochemical abnormalities of pseudohypoparathyroidism. • Lack evidence of PTH resistance • 50% reduction in Gs alpha function • Autosomal dominant
 • Hypoparathyroidism, short stature, round facies, obesity, brachydactily,")
Ps. HP Type Ia (Albright Syndrome) • Hypoparathyroidism, short stature, round facies, obesity, brachydactily, neck webbing, sc calcifications • Defect in the function of Gs protein • TSH, Glucagon, Gonadotropin resistance • Autosomal dominant • Intermittant hypocalcemia, elevated PTH, low urine Ca

Diagnosis • Developmental abnormalities • Serum calcium and phosphorus normal pseudohypoparathyroidism • Hypocalcemia and hyperphosphatemia pseudohypoparathyroidism • Increased serum i. PTH and markedly diminished phosphaturic and nephrogenous c. AMP responses to PTH distinguish • Serum phosphorus normal, low in a hypocalcemic patient secondary hyperparathyroidism due to vitamin D or dietary calcium deficiency and intestinal malabsorption of calcium

Thank you!
- Slides: 34