Hyponatremia By Janel Canty RNS Osborn 2010 Objectives
")
Hyponatremia By: Janel Canty RNS (Osborn, 2010)

Objectives �To understand Hyponatremia �To be able to recognize hyponatremia in a clinical setting �Be able to apply to identify what a medical professionals would do with a patient with hyponatremia

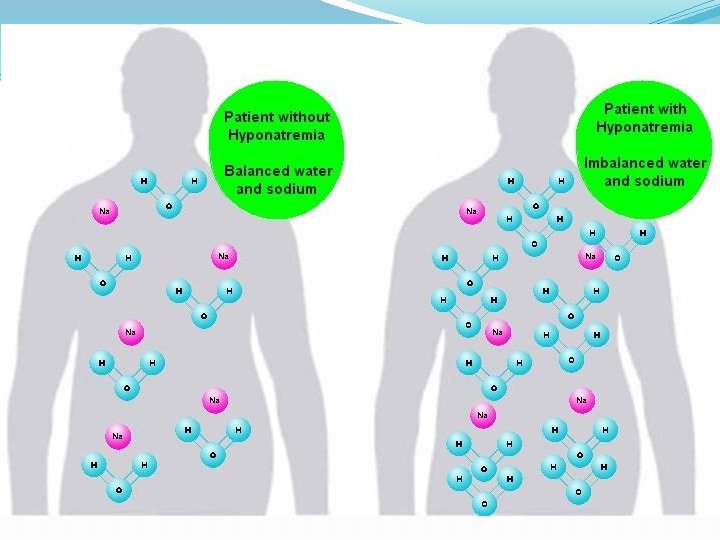
Pathophysiology of hyponatremia This is defined as sodium below the normal range that the human body requires for normal functioning. Sodium is the most numerous cation in the extracellular fluid, it maintains the volume through osmotic pressure, regulates acid-base balance, and conducts nerve impulses. When the sodium balance is off the exchange of electrons between molecules does not take place properly to conduct normal activities. (Osborn, 2010)

What is the range of sodium concentration that the body would like?
 Correct! 135 -145 m. Eq/L")
(Osborn, 2010) Correct! 135 -145 m. Eq/L

Most common Causes �Water excess! �Loss of sodium containing fluids �Ace inhibitors �diuretics �vomiting �diarrhea �Renal failure �Syndrome of inappropriate antidiuretic hormone (Osborn, 2010)

Sign/Symptoms �Initially �Headache, nausea, vomiting �Later stages �Hyponatremic encephalopathy, cerebral edema �May progress to �Hallucinations, lethargy, weakness, bradycardia, ataxia, respiratory depression, seizures, coma, or death �Patients may be asymptomatic Haskal, 2007)

Prevalence � 30% of patients undergoing acute hospital care � 15% of those patients have symptoms �One of the most common electrolyte disorders (Haskal, 2007)

Laboratory test �Urine osmolality �Determines if the kidneys are damaged and can’t dilute the urine � Greater then 100 m. Osm/kg �Serum osmolality �Determines if it hyponatremia or another cause that manifest the same as hyponatremia �Urinary sodium concentration �Determine if the hyponatremia is because of SIADH � Greater then 20 -40 m. Eq/l (Osborn, 2010, medscape)

What population is at risk? �Everyone! �Affects all races the same �Affects both genders the same �Happens at any age � More likely in elderly because of decreased renal function (Osborn, 2010)

Prognosis �In hospitalized patients �Increased association with adverse reactions �Increased mortality �Severe hyponatremia (less than 105 m. Eq/L) �High mortality rate � Over 50% (Nursing central & medscape)

Interventions �Immediately administer one boluses of 2 ml/Kg of 3% Na. Cl IV �Consider other conditions that can cause hyponatremia �Correct underlying cause �Assess for overcorrection of hyponatremia causing hypernatremia �This could cause brain damage �A Bladder catheter should be inserted to monitor the water balance (Overgaard-steensen, 2011)

Patient Scenario �A 46 year old African American male arrived at the emergency room on 9/15 complaining of vomiting for 1 week. Upon arrival the patient had a sodium level of 130 and was admitted for treatment of hyponatremia. Patient was tested and diagnosed with HIV after being admitted. Patient was given Amphotericin B from 916 -2012 until 10 -15 -2012 to treat the HIV.

Interventions for the scenario �The patient was given 3% Na. Cl IV 2 ml/Kg every 6 hours until Sodium levels were in normal range �Patient was started on Amphotericin B �To treat underlying cause of HIV �Patient’s fluids were initially restricted to 1, 000 Ml per day �Patient was on I&O’s

Scenario Outcome �On 10 -16 -2012 the patient’s sodium serum level was 138 m. Eq/l �Within normal range

Nursing Diagnosis �Risk for life-threatening cerebral edema R/T fluid retention or low sodium AEB serum sodium of less than 135 m. Eq/L (Osborn, 2010)

NCLEX! �John came to the ED with a sodium level of 122 m. Eq/L and was treated with 3% Na. Cl IV. When you come to assess John you notice that his level of consciousness has declined. What is this most likely from? �A. Drug use �B. Increasing the sodium levels too quickly �C. hypokalemia �D. infusing the Na. Cl too slowly (Osborn, 2010)

Answer! �John came to the ED with a sodium level of 125 m. Eq/L and was treated with 3% Na. Cl IV. When you come to assess John you notice that his level of consciousness has declined. What is this most likely from? �A. Drug use �B. Increasing the sodium levels too quickly �C. hypokalemia �D. infusing the Na. Cl too slowly (Osborn, 2010)

Nclex �The nurse is caring for a patient and has just received the laboratory data report. Which of the following results cause the most concern? �A. Na+: 115 m. Eq/L �B. K+: 4. 0 m. Eq/L �C. Ca+: 9 mg/d. L �D. Mg+: 2. 0 mg/d. L (Osborn, 2010)

Answer �The nurse is caring for a patient and has just received the laboratory data report. Which of the following results cause the most concern? �A. Na+: 115 m. Eq/L �B. K+: 4. 0 m. Eq/L �C. Ca+: 9 mg/d. L �D. Mg+: 2. 0 mg/d. L (Osborn, 2010)
")
(Osborn, 2010)
. Current issues of nurse practitioners: hyponatremia , 563 -576.")
Work cited �Haskal, R. (2007). Current issues of nurse practitioners: hyponatremia , 563 -576. �Overgaard-steensen, C. (2011). Inital approach to the hyponatremic patient , 139 -145. �Osborn, W. W. (2010). Medical Surgical Nursing. New Jersey: Pearson. �Jensen, S. (2011). Nursing Health Assessment. Philadeplphia: Lippincott Williams and Wilkins. Nusing Central. (2012, 05). (Osborn, 2010)
- Slides: 23