Hypertensive emergencies in obstetrics DR A VENKAT DEPT

Hypertensive emergencies in obstetrics DR. A. VENKAT DEPT OF CRITICAL CARE 1/6/17

Hypertensive emergency A severe elevation in blood pressure with evidence of acute, ongoing target organ damage.

• Preeclampsia is a unique disorder of pregnancy, marked by: • endothelial dysfunction, • hypertension and proteinuria that • typically occurs after 20 weeks of gestation.

Risk factors 1. History of preeclampsia in a prior pregnancy 2. Women younger than 20 years or older than 35 years, 3. Multiple gestations, 4. Obesity, 5. Underlying chronic hypertension or 6. Chronic renal insufficiency, 7. and connective tissue disorders.

Criteria for Severe preeclampsia 1. Blood pressure of > 160 systolic or > 110 diastolic on two occasions 6 hours apart 2. Proteinuria of >5 g in a 24 hour urine specimen (or 3+ on random urine dip on two occasions at least 4 hours apart) 3. oliguria (>500 m. L in 24 hours) 4. Neurologic or visual disturbances (including headache) 5. Pulmonary edema 6. Epigastric or right upper quadrant pain 7. Elevation in transaminases 8. Thrombocytopenia 9. Fetal growth restriction 10. Eclampsia—new onset grand mal seizures in a woman with preeclampsia.
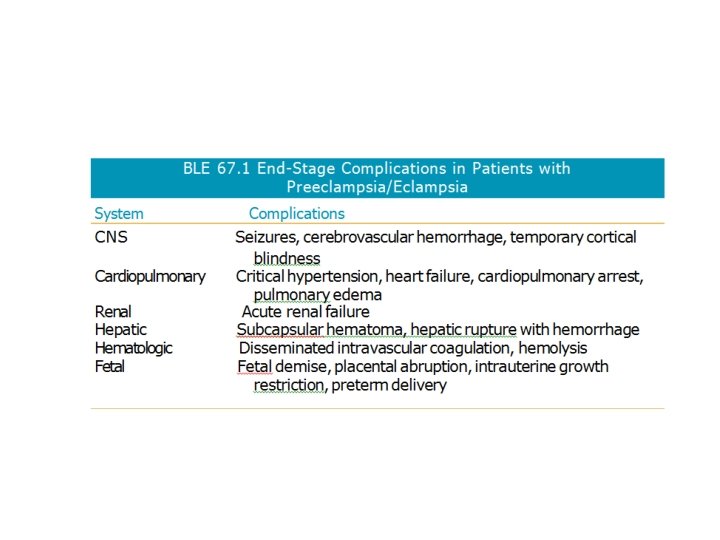

PATHOPHYSIOLOGY BY ORGAN SYSTEM Vascular • Hemoconcentration and hypertension. • intense vasospasm and intravascular contraction. • Alterations in plasma oncotic pressure can cause third spacing of fluid manifested as edema. Hematologic • Hematocrit may be increased secondary to hemoconcentration. • In HELLP syndrome, hematocrit may be low due to hemolysis along with Thrombocytopenia. Hepatic • Elevation of transaminases is often seen in severe preeclampsia. Central Nervous System • Temporary blindness, headache, blurred vision, scotomata, and hyperreflexia are also CNS signs and symptoms of severe preeclampsia. Renal • Vasospasm in preeclampsia causes oliguria and increased creatinine. Fetal • Intrauterine growth restriction, oligohydramnios, and placental infarctions may be seen as manifestations of preeclampsia

TREATMENT GUIDELINES FOR PATIENTS WITH SEVERE PRE ECLAMPSIA/ ECLAMPSIA

TREATMENT • The definitive treatment of severe preeclampsia, and HELLP syndrome is deliv ery if > 36 weeks gestation • Corticosteroids if between 24 34 weeks gestation

TREATMENT GUIDELINES FOR PATIENTS WITH SEVERE PRE ECLAMPSIA/ ECLAMPSIA

• Magnesium sulfate is the preferred antiseizure drug in the setting of preeclampsia/eclampsia and should be given until 24 hrs after delivery • It is provided as an initial intravenous load of 4 to 6 g over 20 minutes, followed by continuous infusion of 1 2 g/hr.

• Meticulous attention to pulmonary status and deep tendon reflexes on clinical examinations should be used in women on magnesium sulfate infusions to prevent magnesium intoxication, which in the most severe form can cause cadiorespiratory collapse. • Because magnesium undergoes renal clearance, serum levels should be assessed in any woman with evidence of impaired renal function and the dose adjusted as needed to sustain a blood level between 4 and 7 m. Eq/L (4. 8 to 8. 4 mg/d. L, 2 to 4 mmoll. L). • Phenytoin may be used in women with impaired renal function or compromised cardiopulmonary function.

• During seizures, the patient's airway should be protected and adequate oxygena tion ensured. If seizures recur while the patient is receiving magnesium, a repeat (4 g) bolus of magnesium may be given. • Other alternatives: include intravenous administra tion of amobarbital or benzodiazepines (lorazepam or diazepam).

TREATMENT GUIDELINES FOR PATIENTS WITH SEVERE PRE ECLAMPSIA/ ECLAMPSIA

• Antihypertensive drugs, including hydralazine, or labetalol, are generally administered for the treatment of BP> 170/110 • CCB are the 2 nd line agents(oral nifedipine) • There is no clear evidence that one of these antihypertensive agents is superior to the others for improving maternal and/or fetal outcomes

• LABETELOL: 10 20 mg i/v loading , then 20 80 mg i/v every 20 30 min until the BP is controlled continouse infusion of 1 2 mg/ min until BP is controlled. • HYDRALAZINE: 5 mg i/v loading dose then 5 10 mg i/v every 20 40 min until bp is controlled.

• Diuretics should be used with caution as they aggrevate the reduction of intra vascular volume that is often seen in pre eclampsia

TREATMENT GUIDELINES FOR PATIENTS WITH SEVERE PRE ECLAMPSIA/ ECLAMPSIA

• intrahepatic hemorrhage with subcapsular hematoma: administration of blood products, and directed con trol of liver hemorrhage. • Embolization of the hepatic artery is often successful, but evacuation of the hematoma and packing of the liver may be required.

TREATMENT GUIDELINES FOR PATIENTS WITH SEVERE PRE ECLAMPSIA/ ECLAMPSIA

• Surveillance: Measure blood pressure at least every 2 hours • Frequent measurement of serum creatinine, hemoglobin, platelets, and liver function tests Fetal ultrasound and cardiotocography • Most women with preeclampsia/eclampsia are expected to have a full recovery after delivery and removal of trophoblastic tissue.

Chronic hypertension • Complicates 5% of pregnancies. • Increased risk for adverse maternal and perinatal outcomes and increased risk for superimposed pre eclampsia • Hypertension antedate the pregnancy or be evident before 20 wks of gestation or if HTN persists beyond 12 wks post partum. • Risk factors : older maternal age, • African, american race and • Obesity.

• Initiation of anti HTN medications is indicated only if BP is 160/105 or above or if there is evidence of end organ damage. • Methyldopa, nifedipine and labetelol are the agents of choice when initiating therapy in pregnancy. • Care should be taken to maintain uteroplacental perfusion. • nitroprusside is relatively contraindicated and ACE inhibitors and ARB`s are absolutely contraindicated in all trimesters.

THANK YOU
- Slides: 25