Hypersensitivity Pneumonitis HP By ziba Loukzadeh M D
 By : ziba Loukzadeh, M. D Occupational Medicine department Yazd University")
Hypersensitivity Pneumonitis (HP) By : ziba Loukzadeh, M. D Occupational Medicine department Yazd University of Medical Sciences
 response Extrinsic allergic alveolitis: granulomatous, interstitial, bronchiolar and alveolar-filling")
Definition n n Immune (hypersensitive) response Extrinsic allergic alveolitis: granulomatous, interstitial, bronchiolar and alveolar-filling lung diseases caused by repeated exposure and subsequent sensitization to a variety of organic and chemical antigens

Etiology n Microbial n Animal n Low agents proteins molecular weight chemicals

Microbial agents n Bacteria -Farmer’s lung -Bagassosis -Mushroom worker’s lung n Fungi -Wood pulp worker’s lung -Cheese washer lung n Ameba -Humidifier lung

Bacteria cause occupation Agent source Major antigen Farmer's lung Agriculture worker Moldy hay thermoactinomycet Mushroom worker's Mushroom worker Compost thermoactinomycet Bagassosis Bagass worker Moldy sugarcane thermoactinomycet

Animal proteins n Avian proteins : Bird breeder’s lung n Urine , Serum , Pelts : Animal handler’s lung n Wheat weevil : Wheat weevil lung

Chemicals n Isocyanate n HP TDI , MDI , HDI n TMA HP n Trimellitic anhydride
 influx")
Pathogenesis n Immunology n Repeated inhalation of antigens sensitization immunology response(type III, IV) influx of neutrophiles shift T lymphocytes (~70%)(predominantly of CD 8) Antibodies in HP are Ig. G class n Response delay by 3 -8 hours n
 n Host factors -Non smokers > smokers -Polymorphism in TNF-α gene -No")
Pathogenesis (cont’) n Host factors -Non smokers > smokers -Polymorphism in TNF-α gene -No association with HLA
 n Exposure factors: -Ag concentration -Duration of exp. -Frequency & intermittency of")
Pathogenesis (cont’) n Exposure factors: -Ag concentration -Duration of exp. -Frequency & intermittency of exp. -Particle size -Use of respiratory protection n Farmer's lung disease: winter Bird breeder's lung: summer Indirect exposure n n

Clinical features n Acute HP : fever , chill , myalgia , cough & dyspnea + basilar rales in Ph/E (412 h after heavy exp. ) Recurrent febrile episodes (most frequent presentation) n Subacute & chronic HP : insidious onset of respiratory symptoms , malaise , fatigue , weight loss + basilar rales , wheezing cyanosis , right sided HF in Ph/E
 n immunologic disease (Asthma) n infection")
DDx n Inhalation fevers n others granulomatous disorder(Sarcoidosis) n immunologic disease (Asthma) n infection n fibrotic lung disease (IPF)

Comparison HP& Inhalation fever Feature HP Inhalation fever Example Farmer`s lung disease Metal fume fever Etiology Thermoactinomyces Zinc fume fever pathophysiology Hypersensitive reaction Cytokine- mediated Exposure dose Low dose (? ? ) High dose Sensitization required Yes No
 Feature HP Fever Yes Inhalation fever Yes Flu-like syndrome")
Comparison HP& Inhalation fever (cont´) Feature HP Fever Yes Inhalation fever Yes Flu-like syndrome Cough Yes Expected Not necessary Dyspnea Yes Not typically Chest exam Rales normal
 Feature CXR HP Inhalation fever Chronic sequle Alveolar No")
Comparison HP& Inhalation fever (cont´) Feature CXR HP Inhalation fever Chronic sequle Alveolar No infiltration Decreased Minimal change DLCO&volum s Lymocytosis Inincreased Neutrophiles ~yes None Natural Hx Reccurent or PFT BAL Complete recovery

Lab. studies n Precipitin n Ab: Helpful but not specific, not sensitive, not hallmark n Leukocytosis , mild elevation of ESR , CRP , Ig. G , Ig. A , Ig. M , ACE , ANA
 n Restrictive n Obstructive n Mixed n decreased DLCO")
PFT Normal (early dis. ) n Restrictive n Obstructive n Mixed n decreased DLCO (most sensitive physiologic test in early HP ) n

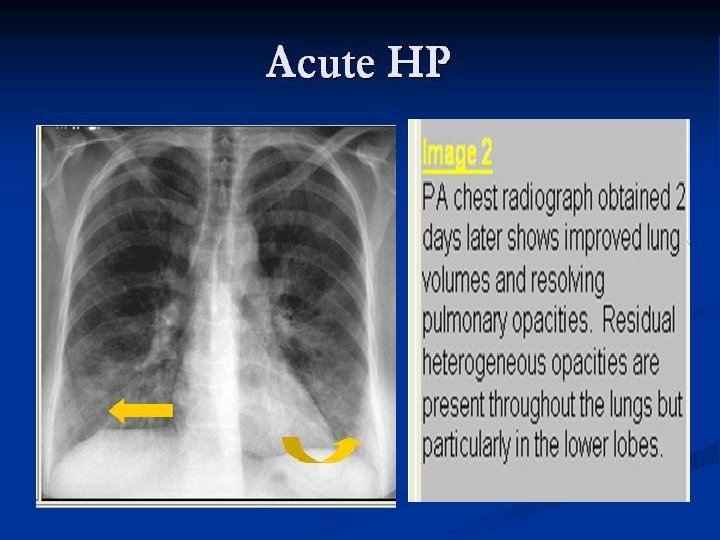
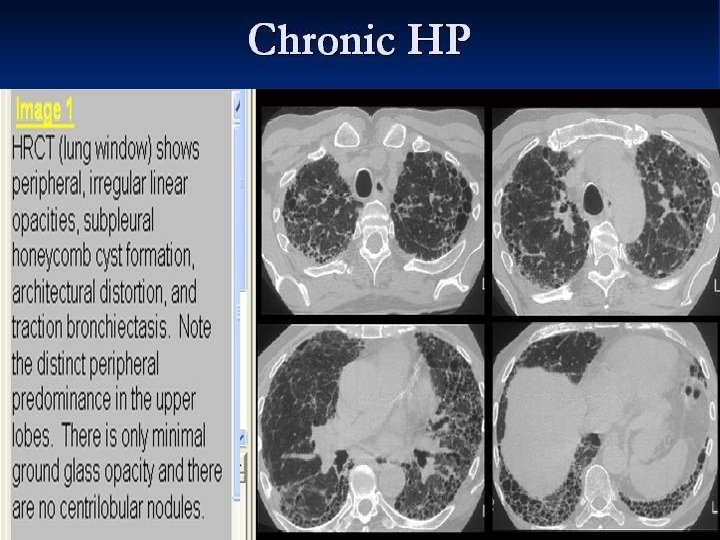
CXR n Acute : diffuse ground glass , fine nodular or reticulonodular pattern (lower lung ) n Subacute n Chronic : reticulonodular pattern : fibrosis , reticular opacity, honey combing n mediastinal lymphadenopathy (up to

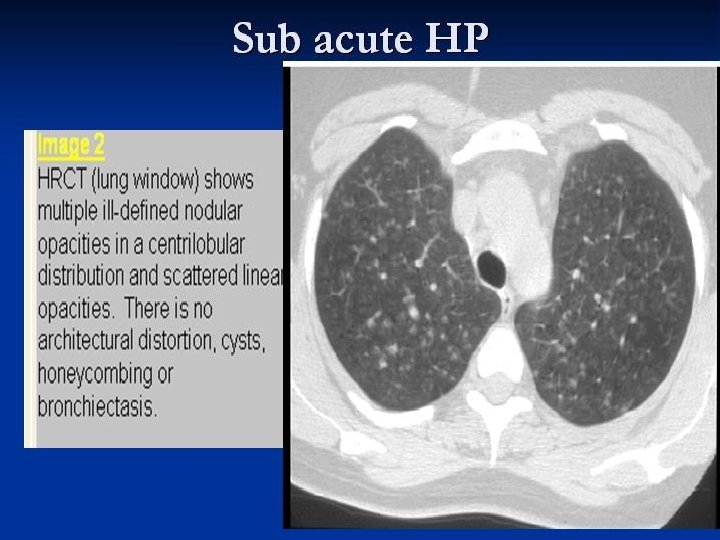
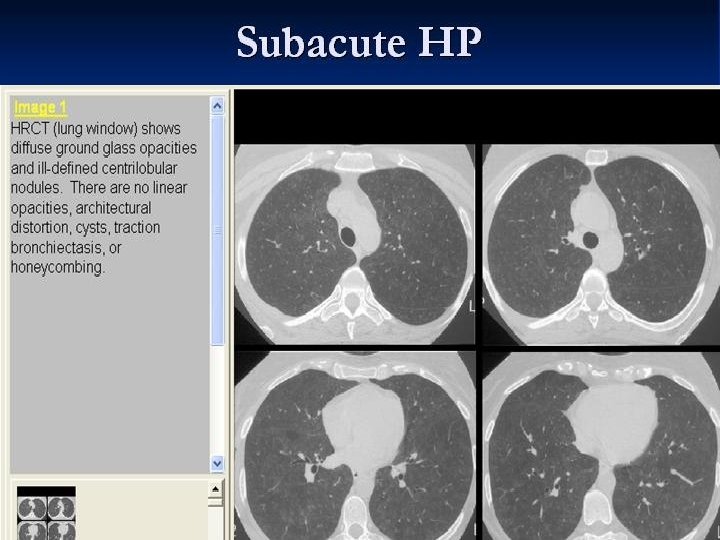
HRCT n Ground glass n Centrilobular nodules n Airspace consolidation n Mosaic patten n Fibrosis n Emphysema

Normal CXR



Histopathology n Classic n cellular n n triad : bronchiolitis lymphoplasmocytic interstitial infiltration non-necrotizing granuloma

diagnosis n Temporal relationship between symptoms and certain activities is often the first clue to the diagnosis of HP

diagnosis n environmental history: pets and other domestic animals n hobbies such as gardening and lawn care n recreational activities, for example, use of hot tubs and indoor swimming pools n use of humidifiers, cool mist vaporizers, and humidified air conditioners n moisture indicators such as leaking, flooding, or previous water damage to carpets and furnishings n

Diagnostic criteria n Required appropriate exposure dyspnea on exertion inspiratory crackles lymphocytic alveolitis n Supportive recurrent febrile episodes infiltrative on CXR decreased DLCO precipitating antibodies granulomatous on lung biopsy improvement with contact avoidance

Treatment n Best treatment : Removal from exp. n Preferred approach : Elimination of Ag. n Oral corticosteroid : in severe or progressive disease n O 2 , inhaled steroid & B-agonist in airflow limitation

- Slides: 33