Hypersensitivity Dr S Nishan Silva MBBS HYPERSENSITIVITY REACTIONS
")
Hypersensitivity Dr. S. Nishan Silva (MBBS)

HYPERSENSITIVITY REACTIONS - State of reactivity to antigen that is greater than normal - denotes a deleterious rather than a protective outcome

HYPERSENSITIVITY REACTIONS Type I, III: Ab mediated Type IV: T cell mediated TYPE I : Ig. E-mediated Reactions Immediate hypersensitivity TYPE II: ANTIBODY-MEDIATED CYTOTOXIC Reactions TYPE III: IMMUNE COMPLEX REACTIONS TYPE IV: T-CELL-MEDIATED, DELAYED-TYPE HYPERSENSITIVITY (DTH)
 Electron micrograph of normal mast cell illustrating large monocyte-like nucleus")
FIGURE 14. 1. (A) Electron micrograph of normal mast cell illustrating large monocyte-like nucleus and electron-dense granules. (B) Mast cell that has been triggered and is beginning to release contents of granules, as seen by their decrease in opacity and formation of vacuoles connecting with exterior. (Photographs courtesy of Dr. T. Theoharides, Tufts Medical School. )

FIGURE 14. 2. Mast cell degranulation mediated by antigen cross-linking of Ig. E bound to Ig. E Fc receptors (Fc RI).

FIGURE 14. 3. Induction of mast cell degranulation.

FIGURE 14. 4. Mediators released during activation of mast cells.

FIGURE 14. 5. Late-phase reaction of type I Ig. Emediated hypersensitivity showing some of mediators involved.

FIGURE 14. 6. Overview of induction and effector mechanisms in type I hypersensitivity.

Clinical Aspects of Type I Hypersensitivity Allergic Rhinitis : hay fever, most common Food Allergies: peanuts, egg, fruits, wheal and flare reaction (atopic urticaria) Atopic Dermatitis: in young children Asthma: airborne pollens, dust, viral Ag

TYPE I Hypersensitivity Classic allergy �Mediated by Ig. E attached to Mast cells. �The symptoms resulting from allergic responses are known as anaphylaxis. � Includes: Hay fever, asthma, eczema, bee stings, food allergies.

Allergens �Allergens are nonparasite antigens that can stimulate a type I hypersensitivity response. �Allergens bind to Ig. E and trigger degranulation of chemical mediators.

Allergens In the US --36 million people said to have hay fever!

Characteristics of allergens �Small 15 -40, 000 MW proteins. �Specific protein components �Often enzymes. �Low dose of allergen �Mucosal exposure. �Most allergens promote a Th 2 immune.

Allergens Example: Der P 1 is an enzyme allergen from the fecal pellets of the dust mite. Dermatophagoides pteronyssinus (common dust mite)

Der P 1 Allergen is easily aerosolized and inhaled. Der P 1 breaks down components of tight junctions which helps it to cross mucosa.

Atopy �Atopy is the term for the genetic trait to have a predisposition for localized anaphylaxis. �Atopic individuals have higher levels of Ig. E and eosinophils.
.")
FIGURE 14. 7. Wheal-and-flare reaction (atopic urticaria).
 Early/Late Effect on lung airflow OR Wheezing")
Immediate vs Late Effects (early mediators) Early/Late Effect on lung airflow OR Wheezing

Mechanisms of allergic response Sensitization Repeated exposure to allergens initiates immune response that generates Ig. E isotype. Th 2 cells required to provide the IL-4 required to get isotype switching to Ig. E.

Mechanisms of allergic response Sensitization Th 2/B cell interaction IL-4 R CD 40 Drive B cell Activation and Ig. E isotype switch. Busse and Lemanske NEJM Feb 2001. 344: 350

Mechanisms of allergic response Sensitization �The Ig. E can attach to Mast cells by Fc receptor, which increases the life span of the Ig. E. �Half-life of Ig. E in serum is days whereas attached to Fce. R it is increased to months.

Systemic anaphylaxis �Systemic vasodilation and smooth muscle contraction leading to severe bronchiole constriction, edema, and shock. �Similar to systemic inflammation.

Ex : Insect Sting

Features �Features result from the injection of venom or other substances into your skin. �The venom sometimes triggers an allergic reaction. �Most reactions to insect bites are mild, causing little itching or stinging. � A delayed reaction may cause fever, hives, painful joints and swollen glands. �Only a small percentage of people develop severe reactions (anaphylaxis) to insect venom.

Some - NO reactions…

Some – Moderate reactions

Some – SEVERE reactions

Signs and symptoms of a severe reaction �Nausea �Facial swelling �Difficulty breathing �Abdominal pain �Deterioration of blood pressure and circulation (shock)
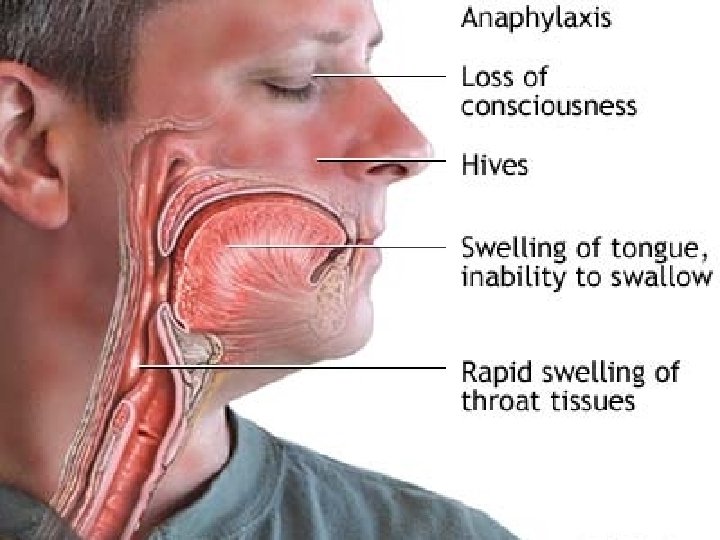

Severe reaction : Pathophysiology

For mild reactions…. �Move to a safe area. �Remove the stinger. �Apply a cold pack �Apply hydrocortisone cream (If necessary). �Take an antihistamine �Allergic reactions may include mild nausea and intestinal cramps, diarrhea, or swelling.

For severe reactions. . � � � If possible give adrenaline. Have the person take an antihistamine pill if he or she is able to do so without choking. Have the person lie still on his or her back with feet higher than the head. Loosen tight clothing and cover the person with a blanket. Don't give anything to drink. Turn the person on his or her side to prevent choking if there's vomiting or bleeding from the mouth. Begin CPR if there are no signs of circulation, such as breathing, coughing or movement.

Risk of allergy: Family 50 40 percent of children with atopy 30 20 10 0 none both number of parents with history of allergy

Risk of allergy: Ig. E Levels 100 Percent of subjects 80 60 40 20 0 <60 60 -200 200 -450 >450 % of population with given Ig. E concentration % of subjects with that Ig. E concentration who are atopic

FIGURE 14. 8. Destruction of worm by eosinophils that have migrated to area and been activated following Ig. E- and antigen-mediated mast cell degranulation.

Type II hypersensitivity Figure 15. 1 Schematic illustration of three different mechanisms of antibody- mediated injury in type II hypersensitivity
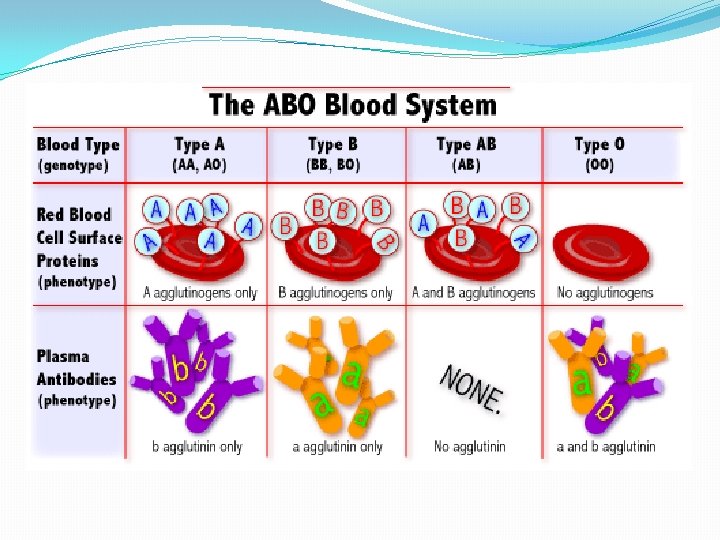

ABO Blood Group Antigens A NAG Fuc H NAG Gal Precursor oligosaccharide Gal NAc. GA NAG Gal A antigen Fuc B antigen H antigen NAc. GA (N-acetylgalactoseamine) Gal (galactose) NAG B Gal Fuc Gal
 ABO in serum A AA,")
ABO Blood Group Reactivity blood groupgenotypesantigens antibodies to (phenotype) ABO in serum A AA, AO A anti-B B BB, BO B anti-A AB AB A and B none O OO H anti-A/B
 first birth post partum subsequent Rh.")
Rh Incompatibility Reaction (Hemolytic Disease of the Newborn) first birth post partum subsequent Rh. D negative mother Rh. D positive red cells Rh. D positive fetus B cell anti-Rh. D Lysis Of RBC’s Rh. D positive fetus

Drug-Induced Reactions: Adherence to Blood Components blood cell adsorbed drug or antigen drug metabolite antibody to drug complement Heamolysis

Type III Hypersensitivity Diseases associated with immune complexes • Persistent infection – microbial antigens – deposition of immune complexes in kidneys • Autoimmunity – self antigens – deposition of immune complexes in kidneys, joints, arteries and skin • Extrinsic factors – environmental antigens – deposition of immune complexes in lungs

characteristics Free Ag + Primed Ab blood vessel wall n Larger immune complex Deposit in tissue or Inflammatio

Mechanism of type III hypersensitivity Formation of the intermediate immune complex Deposition of the intermediate immune complex Tissue injury by the immune complex

Figure 15. 2 Schematic illustration of the three sequential phases in the induction of systemic type III (immune complex) hypersensitivity

Disease Models • Serum sickness • Arthus reaction

Serum Sickness

Arthus Reaction
 Gross appearance, showing hemorrhagic appearance")
Figure 15. 5 Type III hypersensitivity Arthus reaction. (A) Gross appearance, showing hemorrhagic appearance (purpura); (B) Histologic features of Arthus reaction showing neutrophil infiltrate

Figure 15. 3 Ribbon-like deposit of antibody along the basement membrane revealed by fluorescent antibodies to human Ig

16. HYPERSENSITIVITY REACTIONS: T-CELLMEDIATED, DELAYED-TYPE HYPERSENSITIVITY Introduction General Characteristics Gross Appearance and Histology of the Reaction Mechanism of DTH Consequences of DTH Variants of DTH Treatment of Cell-Mediated Immunity

Figure 16. 1 The DTH reaction
 Type IV contact sensitivity reaction. gross appearance of reaction to")
Figure 16. 3 (A) Type IV contact sensitivity reaction. gross appearance of reaction to poison ivy. (poison ivy dermatitis) (B) Type IV contact hypersensitivity reactionhistologic appearance showing intraepithelial blister formation and mononuclear infiltrate in the dermis. (C) Cutaneous basophil reaction showing basophils and some mononuclear cells 24 hours after skin test
 Type IV delayed-type hypersensitivity reaction gross appearance showing induration and")
Figure 16. 4 (A) Type IV delayed-type hypersensitivity reaction gross appearance showing induration and erythema 48 hours after tuberculin test. (B) Type IV delayed-type hypersensitivity reaction histologic picture showing dermal mononuclear cell infiltrate and perivascular cuffing.

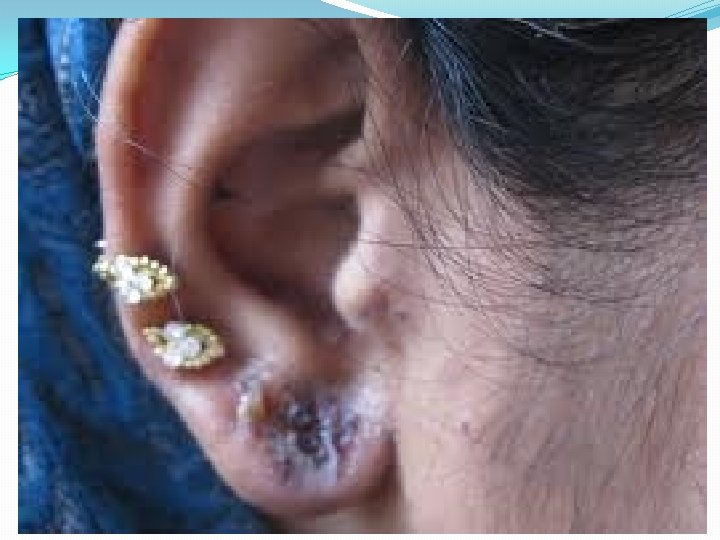
Type IV DTH Contact dermatitis �The response to poison oak is a classic Type IV. �Small molecules act as haptens and complex with skin proteins to be taken up by APCs and presented to Th 1 cells to get sensitization. �During secondary exposure Th 1 memory cells become activated to cause DTH.

Contact dermatitis




Gel and Coombs classification of hypersensitivities. Type III Type IV Ig. E Mediated Ig. G/Ig. M Mediated Ig. G Mediated T cell Immune complex Disease Delayed Type Hypersensitivity Classic Allergy rbc lysis

- Slides: 64