HYPERSENSITIVITY DEFINATION Normally immune is protective leading to















")









 • Involved in destruction of target that are too")



















- Slides: 57
HYPERSENSITIVITY
DEFINATION • Normally immune is protective leading to only subclinical or localized response • Sometimes the response becomes exaggerated causing extensive tissue damage • Defined as - Injurious consequences in the sensitised host following subsequent contact with specific antigens.
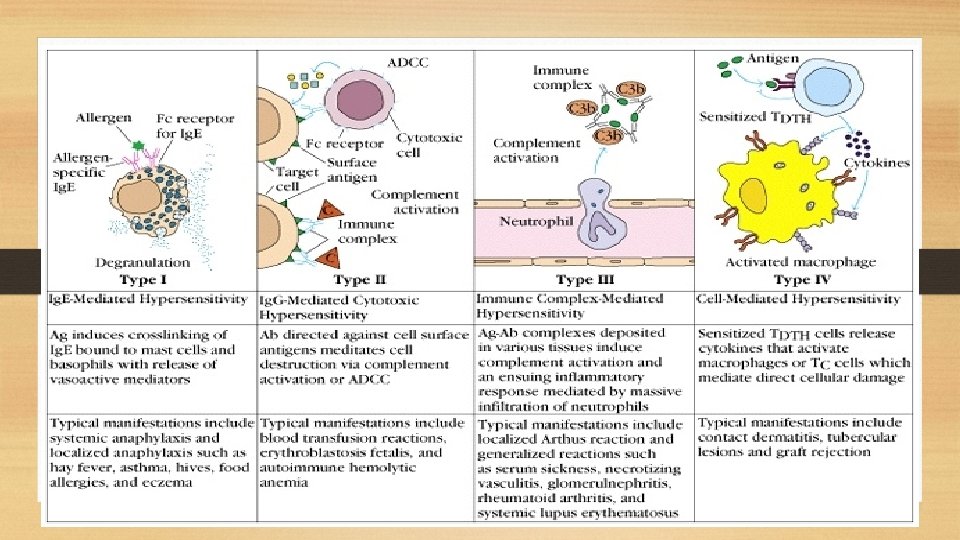
CLASSIFICATION • Following contact HS may occur immediately or after a few days. • It may be due to abnormal humoral or cell mediated immune response. • Gell and Coombs classified hypersensitivity reactions into 4 types. • Later a fifth type was also added k/as stimulatory HS
TYPE I REACTION • Hallmark- production of Ig. E by sensitized B cells after contact with an antigen/allergen. • This in turn leads to degranulation of Mast cells releasing various mediators. • These mediators cause manifestation like Vasodilatation Vascular & smooth muscle contraction Increased vascular permeability
• These changes lead to either a localised response k/as Atopy or a systemic response k/as Anaphylaxis. • The foreign antigens which induce allergy are k/as allergens. • Common allergens associated with type I HS reactions are: 1. Food 2. Plants and Pollens 3. Proteins 4. Drugs 5. products released during insect bite 6. Others like Mould Spores, animal hair & dander.
Demonstration of type I hypersensitivity reactions • P-K reaction • Schultz Dale phenomenon • Theobald Smith Phenomenon
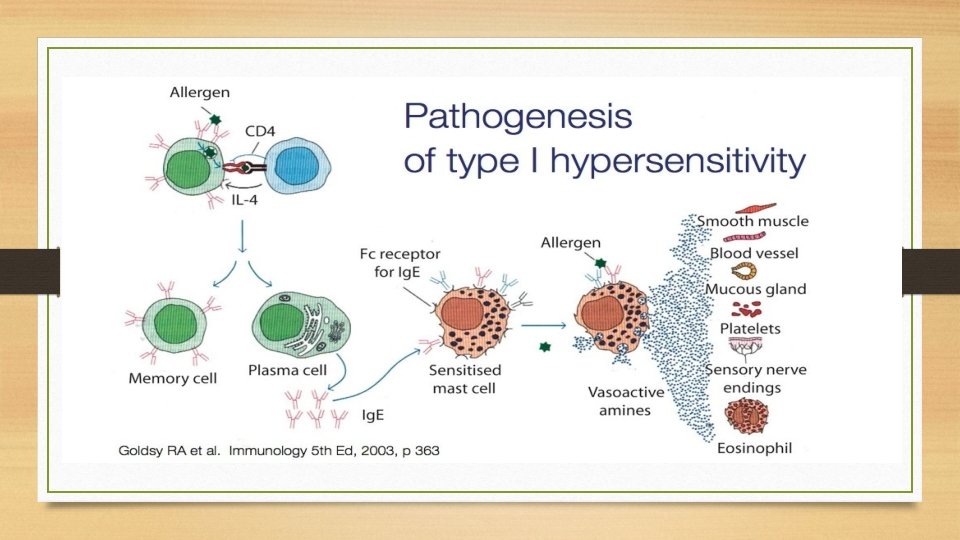
Mechanism of type I reaction • Occurs in two phases: 1. Sensitization phase- occurs when first exposure to antigen occurs 2. Effector phase- occurs during subsequent exposures to same antigen. • Sensitisation can occur by any route but more effective when introduced parenterally. • Allergen is processed by antigen presenting cells (APC)
• Antigenic peptides are presented to the CD 4 helper T cells. • Activated TH cells differentiated into TH 2 cells which secrete IL-4 • IL-4 induces B cells to differentiate into Plasma cells and Memory cells. • Ig. E secreted by plasma cells migrates to target sites and coats on surface of mast cells and basophils. • Fc region of Ig. E binds to Fc receptors on mast cells. • Such Mast cells are k/as sensitised Mast cells and interact with antigen on subsequent exposure.
• Allergen attaches to the Fab region of Ig. E coated on mast cells. • Ig. E cross linkages initiates degranulation of mast cells and results in release of chemical mediators. • Two type of mediators: 1. Primary mediators- preformed, already synthesized by mast cells, released immediately. Eg. Histamine- vascular permeability, ECF-A, NCF-A, Proteasesbronchial mucous secretion 2. Secondary mediators- synthesised by mast cells and released Eg. Prostaglandins and Leukotrienes, PAF, Bradykinin, Cytokines.
HISTAMINE • Most important vasoactive amine in human anaphylaxis • Found in granules of mast cells, basophils and platelets • Released into skin • Burning and itching sensation • Vasodilation and hyperemia (flare effect) • Odema – increasing capillary permeability (wheal effect) • Smooth muscle contraction – various organs
Manifestations • Immediate • Late
IMMEDIATE • Systemic anaphylaxis- medical emergency c/by sever dyspnea, hypotension and vascular collapse leading to death at times • Occurs within minutes of exposure. • Wide range of allergens responsible. Eg. Venom fron bee, drugs, antitoxins, seafoods and nuts • DOC- Epinephrine
• Loclised Anaphylaxis limited to target site, mostly epithelial surfaces at site of entry • These run in families and are inherited. • They are collectively k/as ATOPY. • Eg’s. Allergic rhinitis/hay fever Asthma Food allergy Atopic dermatitis Drug allergy
LATE MANIFESTATIONS • Immediate response followed 4 -6 hrs later by inflammatory response which leads to tissue damage
Factors influencing type I HS reactions 1. Genetic make up 2. Allergen dose 3. Th 1 vs Th 2 response
Detection of type I HS response • Skin prick test • Radioimmunosorbent test (RIST) • Radioallergosorbent test (RAST)
Treatment • • Avoiding contact with knowm allergen Hyposensitization Monoclonal anti Ig. E Drugs like antihistamines, epinephrine, cortisone, theophylline.
TYPE II HYPERSENSITIVITY REACTION • Host injury mediated by antibodies which interact with various types of antigens. Eg’s: 1. host cell surface anigen 2. Extracellular matrix antigen 3. Exogenous antigens absorbed on host cells • The antibody associated is mostly Ig. G & rarely Ig. M.
• Ag-Ab bind, Fc region of antibody initiates the reaction by the following 3 broad mechanisms: 1. Complement dependent reactions 2. Antibody dependent cellular cytotoxicity (ADCC) 3. Autoantibody mediated OR Antibody dependent cellular dysfunction
COMPLEMENT DEPENDENT REACTIONS • The Fc region of bound antibody activates classical complement pathway and leads to host cell injury mediated by following mechanisms: 1. Complement dependent cytolysis- MAC(C 5 -C 9) formed during activation of classical pathway, produces pores which lead to lysis of target cells. 2. Complement dependent inflammation- Byproducts of complement pathway like C 3 a & C 5 a which act as chemoattractants, induces inflammatory response leading to tissue injury. 3. Opsonisation- Byproducts like C 3 b & C 4 b acts as opsonins. They get deposited on target cells. These complement coated target cells are engulfed by macrophage and neutrophil.
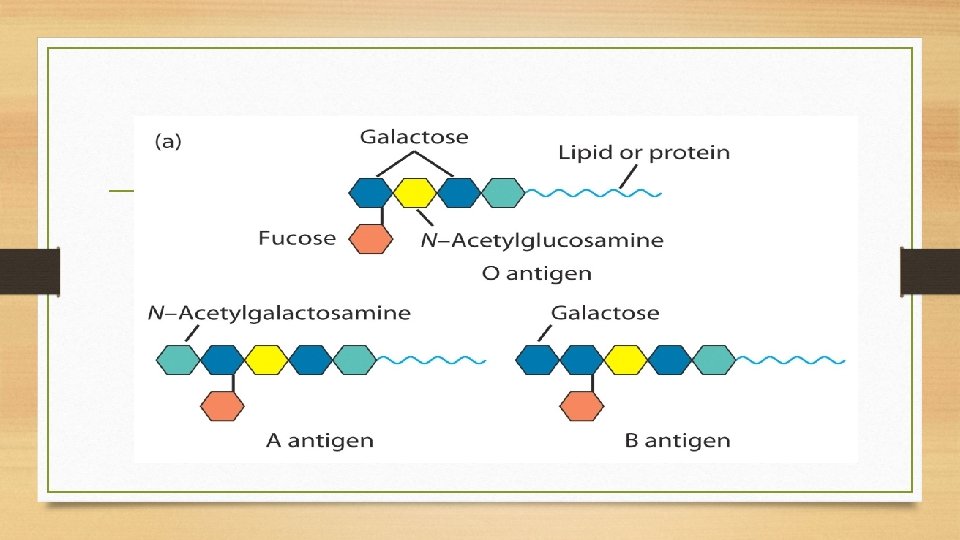
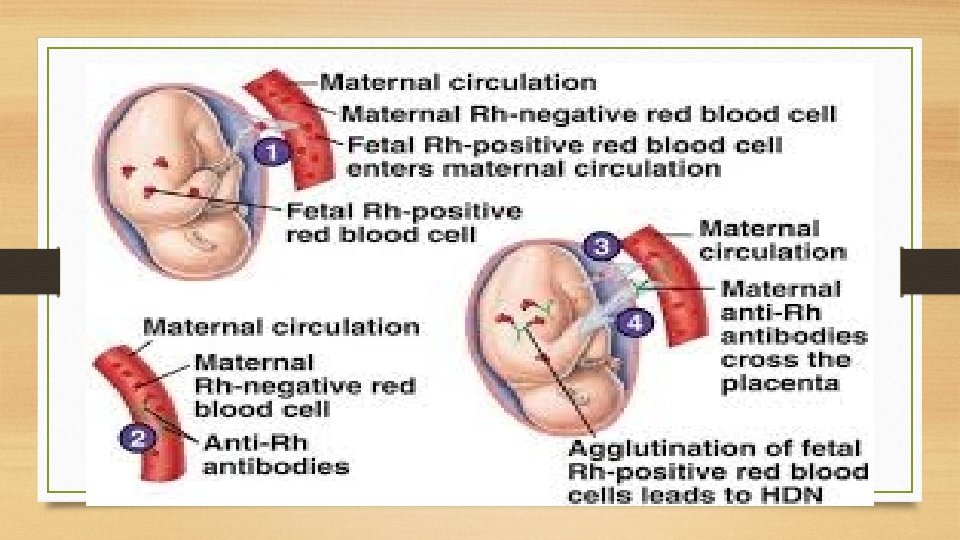
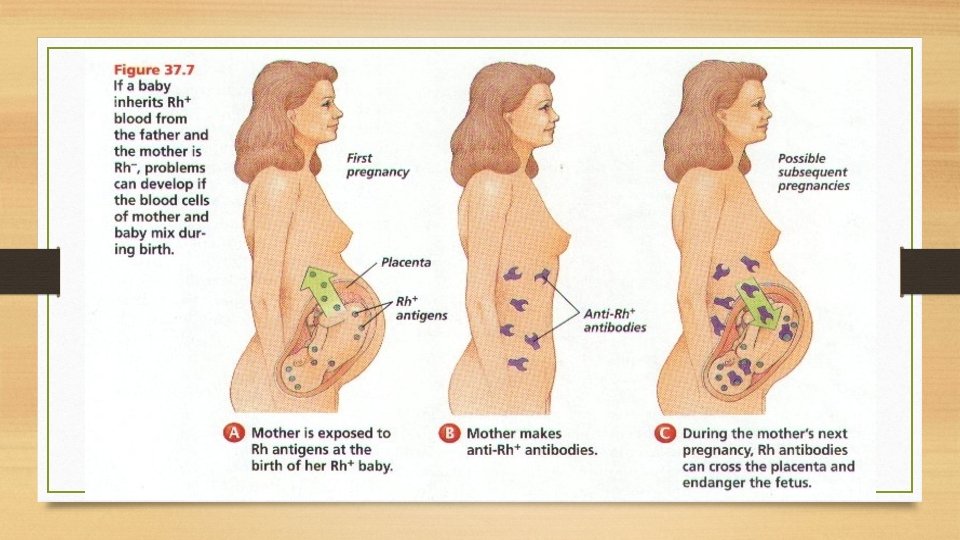
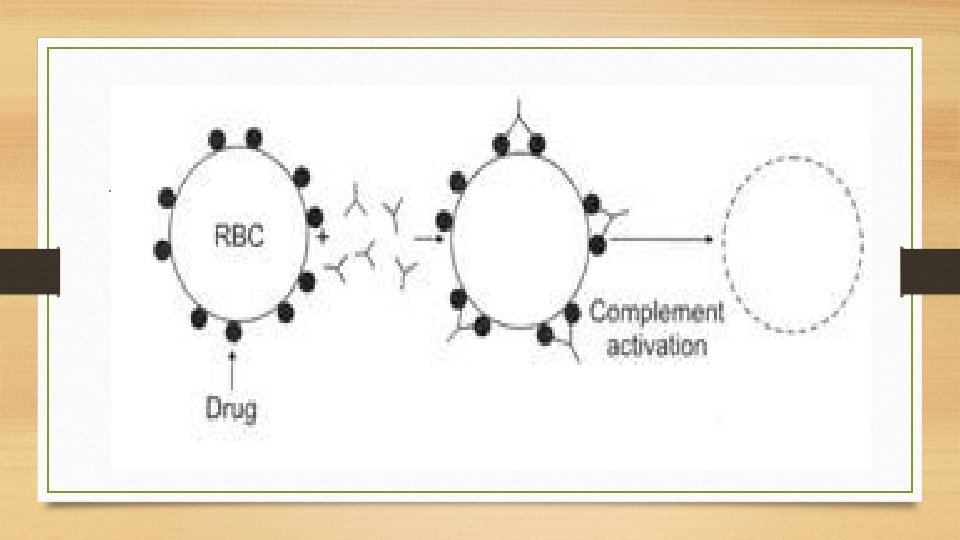
• Clinical conditions in which type II hypersensitivity: 1. ABO incompatibility/ Transfusion reaction 2. Erythroblastosis fetalis/ Rh incompatibility 3. Autoimmune haemolytic anaemia- due to production of autoantibodies to individuals own membrane antigens of RBC’s/granulocytes/platelets. 4. Drug induced haemolytic anaemia- drug or its metabolized product gets adsorbed onto RBCmembrane. If antibodies against drug are formed, they will bind to the adsorbed drug and cause complement mediated lysis of RBC’s. eg. Quinine, penicillin. 5. Pemphigus vulgaris- autoantibodies against desmosomal protein result in disruption of epidermal intracellular junction.
ABO Blood Groups Antibody against rbc antigen binds and mediates killing of rbcs via C’or ADCC causes systemic inflammation.
ERYTHROBLASTOSIS FETALIS
Autoimmune Hemolytic Anemia
DRUG INDUCED HEMOLYTIC ANAEMIA
ANTIBODY DEPENDENT CELLULAR CYTOTOXICITY (ADCC) • Involved in destruction of target that are too large to be phagocytosed • Typically mediated by Ig. G but rarely by Ig. E. • Ig. G coat on target cells by interacting with surface antigen through Fab region. • Fc portion binds to receptors on various cells and results in destruction of target cells.
Antibody dependent cellular dysfunction • Autoantibodies bind and disturb the normal function of self antigens • Anti receptor antibody. Eg’s Graves disease, Myasthenia grevis • Other examples: good pasture, pernicious anaemia, rheumatic fever.
Autoantibody mediated cellular dysfunction
TYPE III HYPERSENSITIVITY REACTIONS • Result of excess formation of immune complexes, which initiate inflammatory response through activation of complement. • Can involve exo or endogenous antigens • Under normal conditions immune complexes rapidly cleared. • In some conditions immune system exposed to excess antigen over long period of time. This leads to excessive formation of immune complexes.
Mechanism of tissue injury 1. Classical complement activation- C 3 a, C 5 a act as anaphylotoxin & chemoattractant. Also neutrophils play a role. 2. Platelet activation- IC bind t Fc receptor platelets and activates them. Aggregation and vasoactive amines released cause tissue ischaemia. 3. Activation of Hageman factor leads to activation of kinin causing vasodilation and oedema
Localised Arthus Reaction • Localised area of tissue necrosia due to vasculitis. • Seen following insect bite, during allergic desensitization • Also occurs due to inhalation of bacteria fungi, spores. Eg’s Farmer’s lung, Bird fancier’s disease
Generalised reaction • Occurs in 2 phases: formation of small sized soluble IC and induction of inflammatory immune response. • Prototype is serum sickness
Disease associated with generalised type III reactions • • SLE RA PAN Parasitic diseases PSGN M. leprae HBV, HCV, IM, Dengue Graft rejection
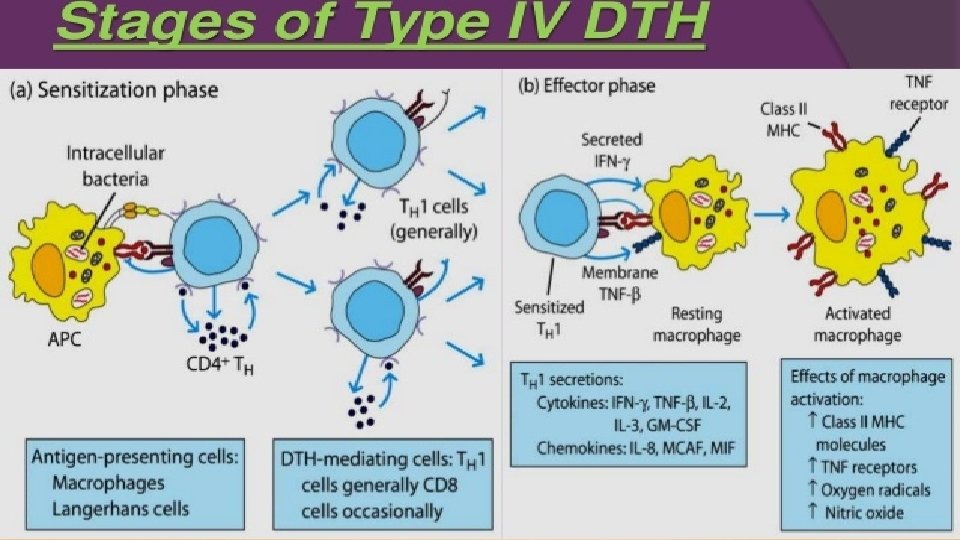
TYPE IV HYPERSENSITIVITY REACTIONS • Also k/as “Delayed Hypersensitivity type of reaction” occurs 48 -72 hrs after Ag exposure • Its cell mediated: TDTH (delayed type hypersensitivity cells) are the main mediators • Tissue injury predominantly due to activated Macrophages
Mechanisms of Type IV reactions • 2 phases • Sensitization phase: Initial 1 -2 weeks following Ag exposure APCs present antigen along with MHC II to helper T cells These differentiate to form TDTH cells
Effector phase: TDTH cells on subsequent contact with the Ag secrete variety of CYTOKINES Attract & recruit macrophages, inflammatory cells to site of reaction INF-γ: activates Macrophages for microbial killing IL: 2 stimulates proliferatio of TDTH cells Monocyte chemotactic factor
Examples of DTH Intracellular pathogens inducing DTH Intracellular bacteria: • M. Leprae • M. Tuberculosis • Listeria monocytogenes • Brucella abortus • • • Intracellular viruses • HSV, Smallpox virus • Measles virus Other examples of DTH • Multiple sclerosis • Hashimotos thyroiditis • Chronic transplant rejection Intracellular fungi: Pneumocystis jerovecii Candida albicans Histoplasma capsulatum Crytococcus neoformans Contact dermatitis: following exposure to nickel, poison ivy
Role of DTH: protective Vs tissue damage • Through DTH host attempts to provide protection • Protective response: Pathogens usually cleared with little tissue damage by macrophages • Tissue damage response: when IC pathogens escape macrophage killing, enhanced phagocytic activity & release of lytic enzymes : tissue damage
Pathology of DTH reaction: Granuloma formation • Continuous DTH response for killing persistent /non degradable Ags leads to granuloma formation (TB, Leprosy) Macrophages transform into flat epithelioid cells Epitheiliod cells fuse : multinucleated giant cells (IFN-γ) Granuloma: inner zone: epithiliod cells, surrounded by lymphocytes rim of fibroblasts
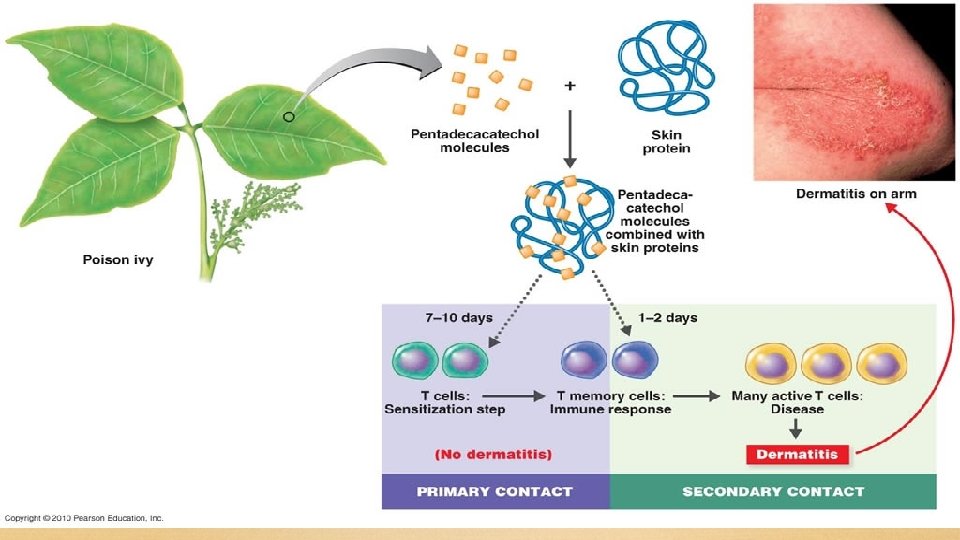
Clinically important Delayed Hypersensitivity reactions. A. Contact dermatitis: • Cell mediated hypersensitivity occurs after contact with simple chemicals like nickel, formaldehyde, plant materials – poison ivy, poison oak, topically applied drugs like sulfonamides, neomycin, sometimes cosmetics, soaps and others.
• Most of these are haptens, attach to skin proteins to become complete antigen: immunogenic • Hapten alters the skin protein & immune system starts recognizing it as foreign: internalized by APCS presented to T-helper cells: induce DTH • Activated macrophages: release lytic enzymes : skin lesions
B. TUBERCULIN TEST • A patient previously exposed to M. tuberculosis is injected with a small amount of Tuberculin (PPD) intra-dermally. • Local reaction develops gradually (induration and redness) 48 -72 hours, suggestive of a Positive test.
• A positive skin test indicates the person has been infected with the agent but it does not confirm the presence of current disease. • But if skin test converts from negative and positive, it suggests that the patient has been recently infected.
• Infected persons need not always have a positive skin test. E. g. overwhelming infections, disorders which suppresses Cell Mediated Immunity like uremia, measles, Sarcoidosis, lymphoma and AIDS or administration of immune-suppressive drugs like corticosteroids, anti-neoplastic agents can cause anergy.
A positive skin test response assists in diagnosis – supports chemoprophylaxis or chemotherapy Examples • 1. Leprosy – Lepromin test • Positive test indicates Tuberculoid type with competent CMI. • Negative test indicates Lepromatous leprosy with impaired CMI.