HYPERLIPIDEMIAS The Basics I DISTURBANCIES OF LIPID METABOLISM

HYPERLIPIDEMIAS The Basics

I. DISTURBANCIES OF LIPID METABOLISM Essential types of disturbances 1. Hyperlipoproteinemias 2. Hypolipoproteinemias 3. Dyslipidemias 4. Hyperlipidemias

DEFINITIONS Hyperlipoproteinemias : Pathologic process manifested by concentration of one or more types of LPs in the blood Hyperlipidemia ( plasma cholesterol and/or triglyceride) is present in all hyperlipoproteinemias. Hypolipoproteinemias : – Decreased concentration of lipoproteins in the blood (usually VLDL, LDL) Dyslipidemias – disorder in lipid spectrum in blood, usually with increased concentration of
Lipoproteins – spheric particles transporting non-polar lipids (TAGs, cholesterol esters)by bloo Composition")
ESSENTIAL TERMS a)Lipoproteins – spheric particles transporting non-polar lipids (TAGs, cholesterol esters)by bloo Composition and properties – inside of sphere - non-polar lipids – surfice of sphere -polar molecules (phospholipids, non esterified cholesterol- are importan for transport of particles in plasma -apo-LPs - are important for LPs metabolism Different types of LPs differs by their density, by volume of transporting lipids, by size, by amount and kind of apo, by location of their creation, by their metabolism
 – the lowest density, the largest")
CHARACTERISTICS OF MAIN TYPES OF LPS • Chylomicrons(CM) – the lowest density, the largest size • VLDL – smaller and more dense than CM – they transport endogenous TAGs synthetised in liver, mainly • IDL – particles with properties between VLDL and LDL • LDL – contain cholesterol esters, mainly • HDL – the smallest size and the highest density – they are able to transport cholesterol from peripheral tissues to liver (reversal transport of cholesterol)
, it is localised at")
• LDL receptor – it takes up LDL (IDL), it is localised at cells in different types of tissues, predominantly at hepatocytes In predisposed patients – intake of cholesterol down regulation of LDLr in liver uptake of LDL from blood • HDL receptor – it takes up HDL from blood, it is localised predominantly in cells that create steroids
 – uptake the LDL which were not bound by LDLr –")
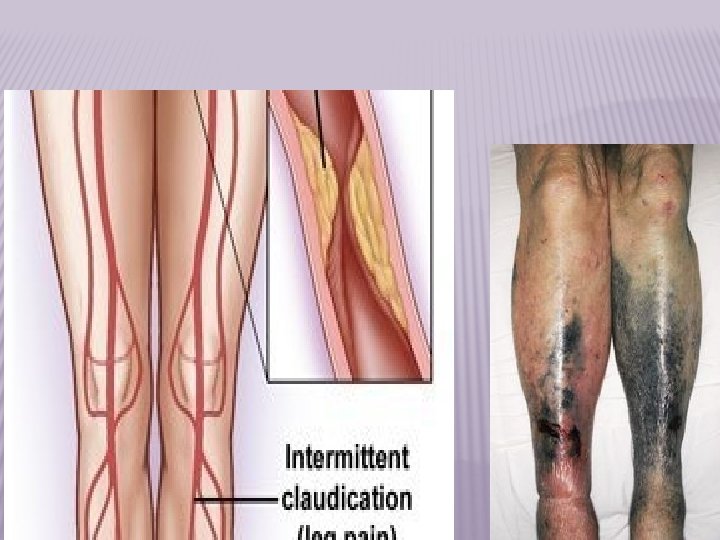
Scavenger receptors (SR) – uptake the LDL which were not bound by LDLr – uptake of oxidized LDL particles – they are present in macrophages, in smooth muscle cells in vessel wall atherogenesis

CHARACTERISTICS THAT MAY IDENTIFY AN INDIVIDUAL WITH A GENETIC PREDISPOSITION TO CARDIOVASCULAR DISEASE Positive Family History Disease in a first-degree relative Parents, siblings Disease in female relatives Disease in the absence of other recognized risk factors Early age-at-onset Genetically determined risk often characterized by an earlier age-at onset Hyperlipidemia resistant to dietary intervention

Mortality/Morbidity: If uncontrolled, there is a higher mortality from cardiovascular and cerebrovascular disease. Age: It may be present in children and young adults but is seen more frequently in later life. The secondary form is caused by other diseases, such as: diabetes mellitus, pancreatitis, renal disease, or hypothyroidism.
 Type lipoprotein lipid 1 CM")
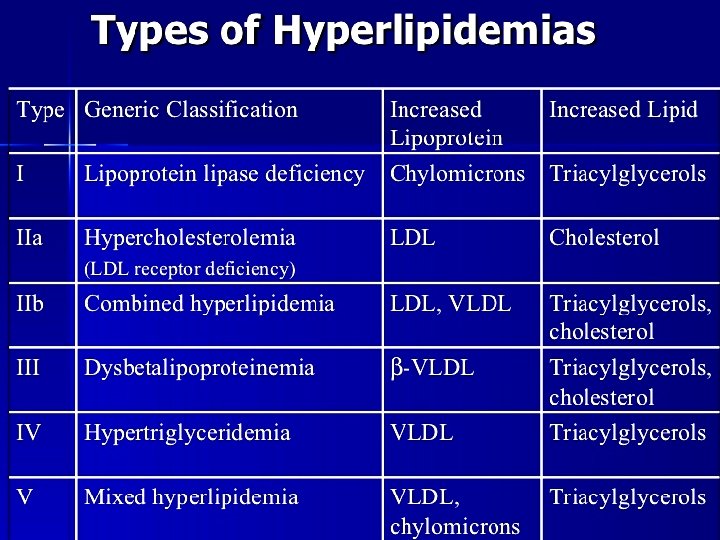
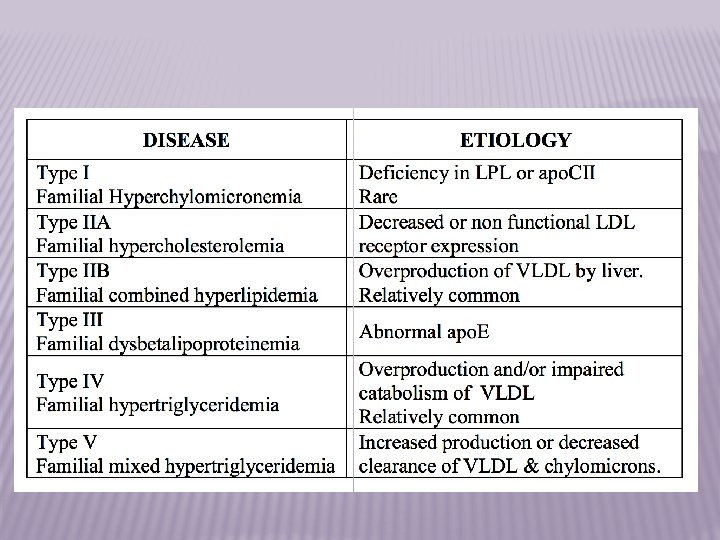
Classification of hyperlipoproteinemias (according Necas et al. , 2000) Type lipoprotein lipid 1 CM TAG 2 a LDL cholesterol 2 b LDL, VLDL cholesterol, TAG 3 IDL, CM- remnants TAG, cholesterol 4 VLDL TAG 5 VLDL, CM TAG, cholesterol
")
Five classes of LDL-R mutations 1 2 3 4 5 Null (no protein synthesis) Transport defect (Golgi) LDL binding defect Internalization-defective Recycling-defective LDL-R bind LDL particles and endocytoses them via clathrin-coated vesicles LDL-R is recycled
 A. Primary 1. Familial combined HLP – it is")
Main types of hyperlipoproteinemias (HLP) A. Primary 1. Familial combined HLP – it is the most frequent genetic HLP – it manifests most likely in phenotypes 2 a, 2 b, 5 – it is the strong risk factor for development of atherosclerosis and ischemic heart disease Mechanisms involved in development HLP secretion • genetic predisposition • acquired (due to environmental factors) of VLDL by liver
 – it manifests predominantly by phenotype 2 a – it")
2. FAMILIAL HYPERCHOLESTEROLEMIA (FH) – it manifests predominantly by phenotype 2 a – it leads to significant acceleration of atherosclerosis development – myocardial infarction in 4 th decade of life – xantomatosis of tendons and arcus lipoides corneae Mechanisms involved in FH development – mutation of LDL receptor decreased uptake of LDL concentration of LDL in blood
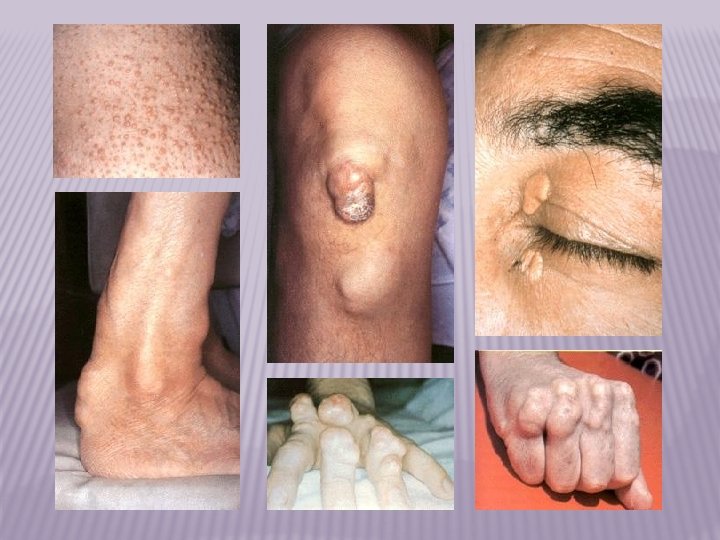

TENDON XANTHOMAS tendon xanthomas of the achilles and elbow

TENDON XANTHOMAS tendon xanthomas of the hand

CUTANEOUS XANTHOMAS
 in")
HYPERLIPIDEMIA SIGNS � Xanthoma- plaques or nodules composed of lipid-layden histiocytes (foamy cells) in the skin, especially the eyelids

FAMILIAL HYPERCHOLESTEROLEMIA FINDINGS IN HOMOZYGOTES left coronary artery narrowing supravalvar lipid deposition

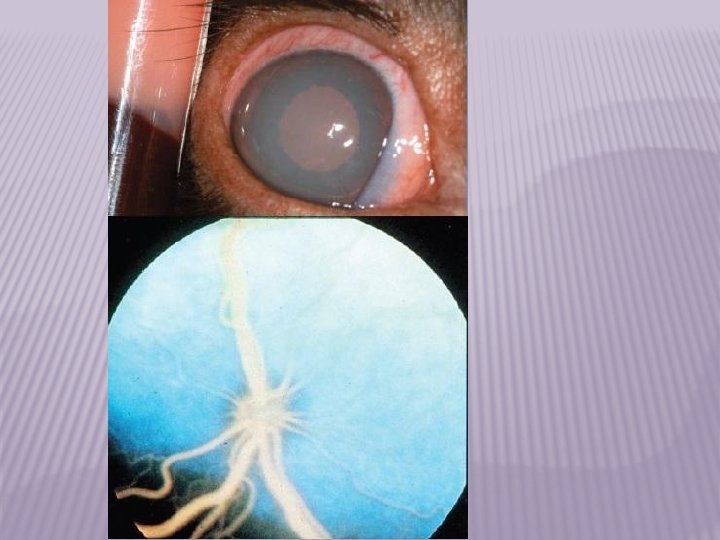
EYE FINDINGS IN FAMILIAL HYPERCHOLESTEROLEMIA Early corneal arcus Cholesterol deposits in retinal fundus

CORNEAL ARCUS � Lipid deposit in cornea

SECONDARY DISORDERS OF LIPID METABOLISM Secondary Disorder Clinical Feature Obesity Increased TG, decreased HDL-C Diabetes mellitus Increased TG and TC, decreased HDL-C Chronic renal failure Increased TG and TC, decreased HDL-C HIV/AIDS wasting Increased TG and TC, decreased HDL-C and LDL-C Hypothyroidism Increased TG, TC and LDL-C Nephrotic syndrome Increased TC and LDL-C Obstructive liver disease Increased TC Medications Variable C = Cholesterol; HAART = Highly-active antiretroviral therapy; HDL = High-density lipoprotein; LDL =Low-density lipoprotein; TC = Total cholesterol; TG = Triglyceride.


THANKS FOR NOT SMOKING
- Slides: 29