hyperkalemia Dr bandar ghazal K level 5 meql

hyperkalemia Dr. bandar ghazal

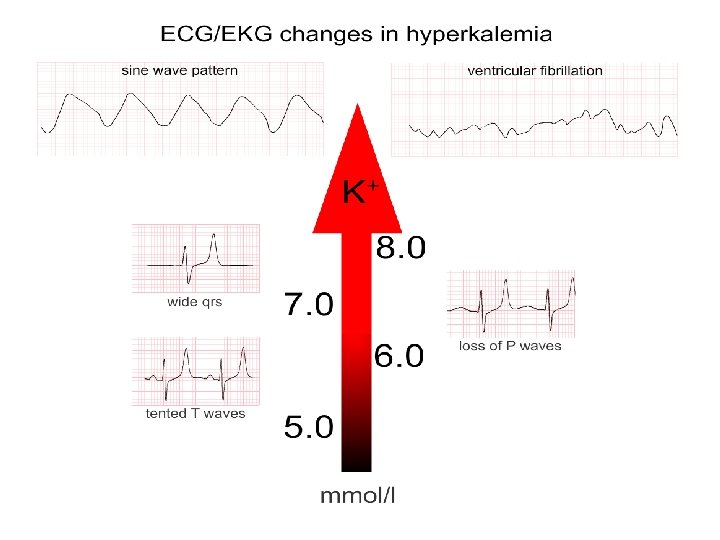
• K level >5 meq/l • Level >6 meq /l can cause fatal arrhythmias. • Slow increase in K is better tolerated. • Signs and symptoms of hyperkalemia : Muscle weakness ECG abnormalities

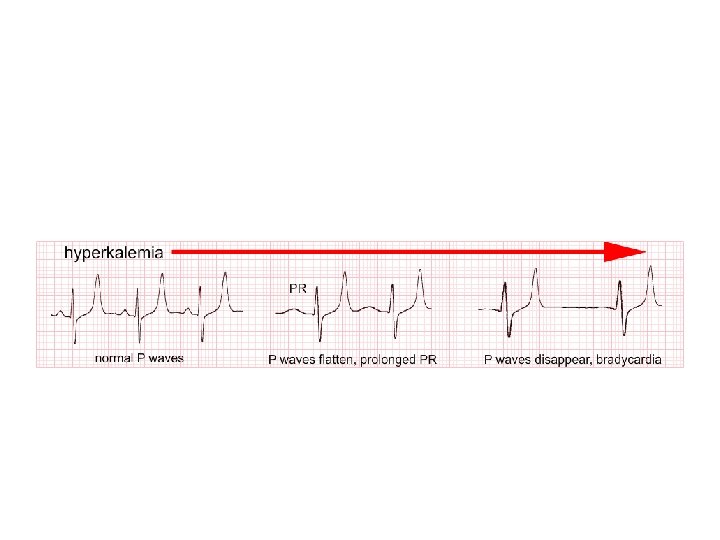
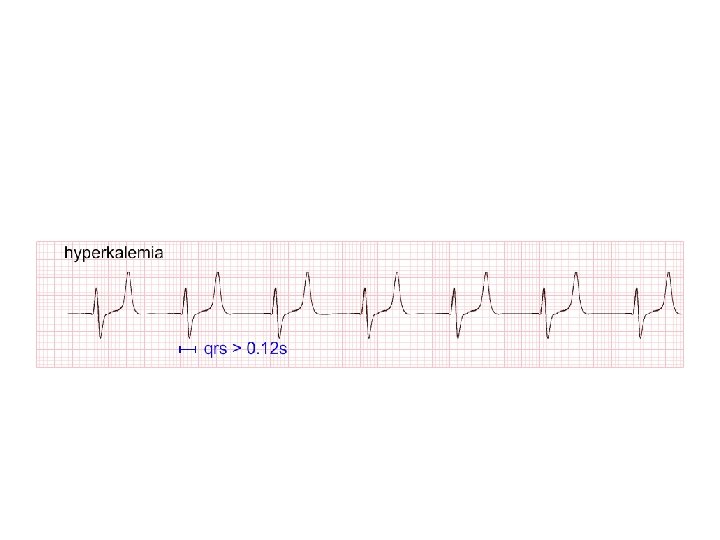
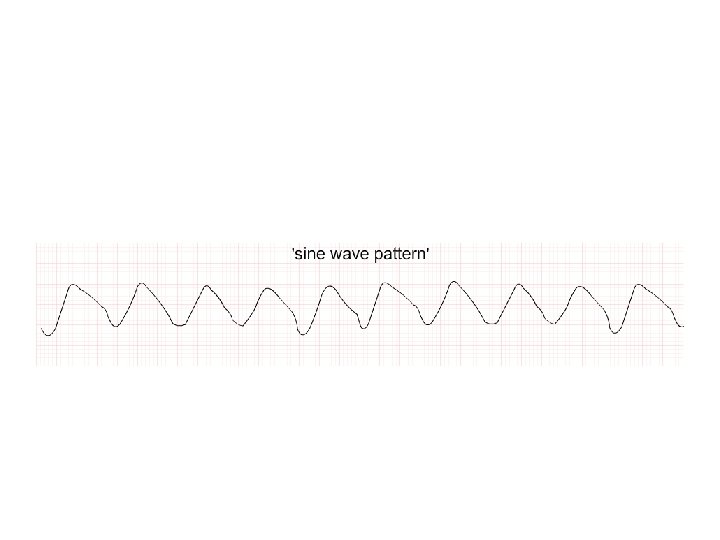
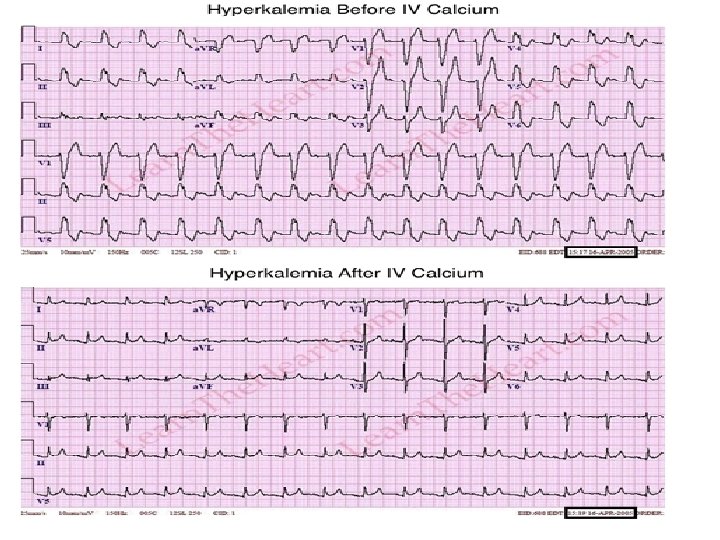
• History , physical examination , review of medications , KFT and ECG. • ECG : Peaked T wave Shortened QT interval More hyperkalemia : Prolongation PR Loss of P wave Widening of QRS Sine wave , V. fib , asystole However ECG findings does not always correlate with severity of hyperkalemia.


CAUSES Transcellular shift DECREASE RENAL PSEUDOHYPERKALEM IA And increase turn over of cells Hemolytic sample When draw sample of blood , during clotting process , k will be released as result of cell disruption and destruction. Tight tourniquet , may increase local k at area. Repeat k level EXCRETION State of hypoglycemia Oliguric AKI CKD with GFR < Use of B 2 20 ml/min/1. 73 m 2 adrenergic blocker , as it alter K distribution Hypoaldosteronism Adrenal insuffiency Rapid breakdown of cells such as rhabdomyolysis or in tumor lysis syndrome from treatment of leukemia , lymphoma. MEDICATIONS K sparing diuretics (spironolactone , triamterne , amiloride. Trimethoprime (by blocking epithelial Na channel ) NSAIDS (dec. Renin ) Heparin RTA 4 ( DM nephropathy)

Management : • K> 6. 5 meq/l or 6 with ECG changes should be treated urgently To stabilize cardiac membrane Shifting k into cells Removing K from the body Ø Ca gluconate 100 mg over 10 min IV Quickly antagonize the effect of hyperkalemia on cardiac membrane. Its has short time of action , so its never a definitive treatment

Ø do serum glucose level if > 250 mg / dl Give insulin IV. Or give IV dextrose 10% with insulin This procedure can be repeated as needed Shift K into cells Its effective up to 6 hours Ø high dose of nebulized albuterol Can be repeated as needed with intervals

Ø Na bicarbonate can be given but its least effective because it does not promote shifting of K. Ø Loop diuretic : remove K from the body Ø K binders : sodium polystyrene sulfonate Controversial Limited effect , due to side effect May cause intestinal necrosis Effects usually take hours Patiromer

Ø Hemodialysis : Treatment of choice in PT with sever hyperkalemia and oliguric kidney disease

• In chronic hyperkalemia : Limit K intake Thiazide or loop diuretics In hypoaldosteronism : fludrocortisone will normalize K. But it may cause HTN and edema. Patiromer Newer K binder
- Slides: 15