Hyperbilirubinemia SDPA Annual Conference Laurie Hogden MD Assistant

Hyperbilirubinemia SDPA Annual Conference Laurie Hogden, MD Assistant Professor of Pediatrics, Division of Neonatology USD- Sanford School of Medicine

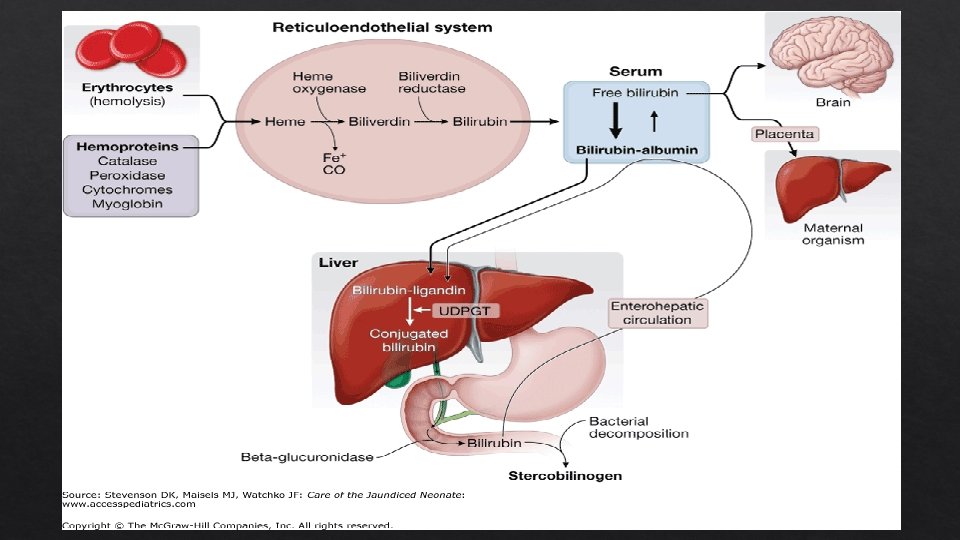
Jaundice and the Neonate 60% of normal newborns become clinically jaundiced in the first week. WHY? Excessive Neonatal What bilirubin formation in newborns liver cannot clear bilirubin from the blood rapidly enough is the significance? Bilirubin is potentially toxic to the central nervous system.
")
Causes of Pathologic Jaundice Increased Blood RBC production of bilirubin group incompatibilities (immune mediated) enzyme deficiencies Structural defects of RBCs Deficiency Impaired All of hepatic uptake conjugation of bilirubin NBs are relatively deficient in UDP glucuronosyltransferase Increased enterohepatic circulation

Risk Factors for Developing Severe Jaundice Decreased risk TSB or Tc. B in low-risk zone • • • Exclusive bottle feeding • • Jaundice observed before discharge Previous sibling with jaundice • Macrosomic infant of diabetic mom • • GA 37 -38 weeks • Black race Discharge from hospital after 72 hrs Major risk factors TSB or Tc. B in the high intermediate zone • Gestational age ≥ 41 weeks • • Minor risk factors Maternal age ≥ 25 years • Male • TSB or Tc. B in high-risk zone Jaundice noted in first 24 hrs Blood group incompatibility with positive DAT or hemolytic dz • • • GA 35 -36 weeks Previous sibling required phototherapy Cephalohematoma/bruising • • Exclusive breastfeeding • East Asian race

Kramer, LJ. Advancement of dermal icterus in the jaundiced newborn. Amer J Dis Child. 1969; 118: 454 -458.

Evaluating your patient Evaluate for jaundice every 8 -12 hours 1. Jaundice in the first 24 hours of life? Measure transcutaneous bilirubin &/or total serum bilirubin & interpret by age in hours & risk level. 2. Jaundice appears excessive for infant’s age? Measure transcutaneous bilirubin &/or total serum bilirubin & interpret by age in hours & risk level. TSB >95 th % Evaluate Treat cause. if criteria met by hour specific phototherapy guidelines. Repeat bili in 4 - 24 hours based on risk assessment.

Subcommittee on Hyperbilirubinemia Pediatrics 2004; 114: 297 -316

Nomograms for Tc. B levels according to gestational age. M. Jeffrey Maisels, and Elizabeth Kring Pediatrics 2006; 117: 1169 -1173 © 2006 by American Academy of Pediatrics

Nomogram risk assessment LOW MEDIUM HIGH > 38 weeks gestation and well 38 weeks with risk factors OR 35 -37+6 weeks with risk factors 35 -37+6 weeks and well RISK FACTORS • Isoimmune hemolytic disease • G 6 PD deficiency • Asphyxia • Lethargy, temp instability, sepsis • Albumin <3 g/d. L

Guidelines for phototherapy in hospitalized infants ≥ 35 weeks’ gestation M. Jeffrey Maisels et al. Pediatrics 2009; 124: 1193 -1198

Guidelines for exchange transfusion in infants 35 or more weeks’ gestation. Measure transcutaneous bilirubin &/or total serum bilirubin Subcommittee on Hyperbilirubinemia Pediatrics 2004; 114: 297 -316
 transfusion")
Treatment Options Phototherapy Intravenous Exchange Gamma Globulin (IVIG) transfusion

Sister Jean Ward, phototherapy, and jaundice: a unique human and photochemical interaction MJ Maisels Journal of Perinatology (2015) 35, 671– 675; . • First noted that exposure to sunlight caused jaundice to fade. • In the same hospital weeks later, a sample of blood from a jaundiced infant was exposed to sunlight and had become green with a bilirubin content much lower than expected. • Dr. Richard Cremer: “It seems that we had stumbled on something that might have a practical application”!!

Maisels MJ, Mc. Donagh AF. N Engl J Med 2008; 358: 920 -928

Maisels MJ, Mc. Donagh AF. N Engl J Med 2008; 358: 920 -928.

Complications of phototherapy Separation of Mom and Baby Retinal injury “Bronze Baby” effect Infants with cholestasis can develop dark, grayish-brown discoloration of skin, serum and urine Purpura/bullous eruptions Increased melanocytic nevi? Increased risk of childhood cancer? Failure of closure of PDA in preterm infants?

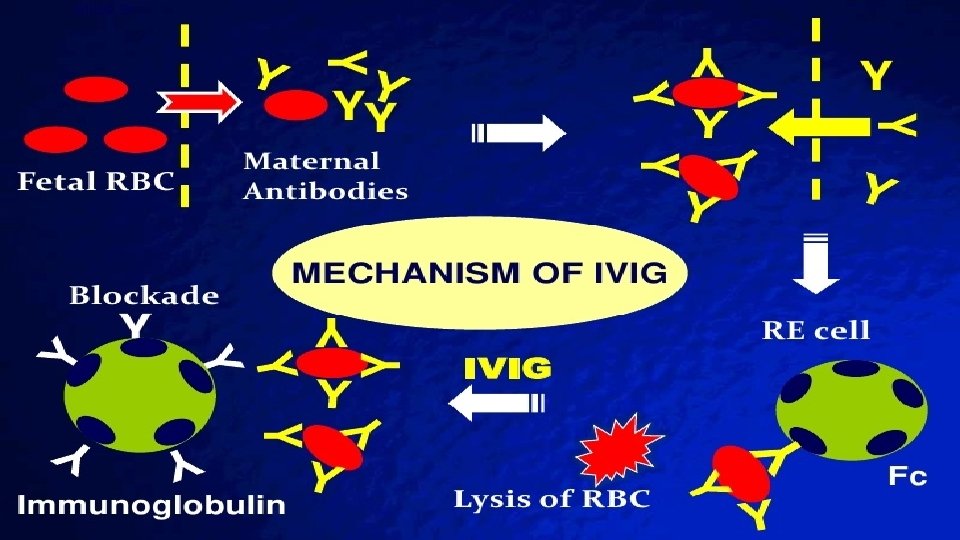
IV Immune Globulin IVIG is a plasma derived, concentrated form of Ig. G antibodies pooled from the donor population IVIG has biologic activity against IMMUNE-MEDIATED hemolysis IVIG reduces the need for exchange transfusion in Rh and ABO hemolytic disease. Presumed to be effective in other types of Rh hemolytic disease such as anti-C and anti-E. IVIG is recommended if TSB is rising despite intensive phototherapy or if the TSB is within 2 -3 mg/d. L of the exchange level. Dose: The 0. 5 -1 g/kg IV over 2 hours infusion can repeated 12 hours later.

Exchange Transfusion Indications Immediate exchange transfusion for jaundiced infants with signs of intermediateadvanced stages of acute bilirubin encephalopathy even if the TSB is falling. Hypertonia, arching, retrocollis, opisthotonos, fever, high pitched cry During birth hospitalization: if TSB rises to exchange level despite intensive phototherapy For readmitted infants: if TSB is above exchange level, provide phototherapy. Consider exchange if the TSB is still above exchange level after intensive phototherapy for 6 hours. Elevated Bilirubin/Albumin Ratio (TSB mg/d. L / Albumin g/d. L) Infants ≥ 38 wks: 8 35 -36+6 wks and well or ≥ 38 wks and high risk: 7. 2 35 -37 +6 wks and high risk or hemolytic disease or G 6 PD def: 6. 8
 crossmatched")
Exchange Transfusion • Double volume exchange uses modified whole blood (RBCs and plasma) crossmatched against mother and compatible with infant. • Term infant blood volume = 80 ml/kg • Volume of blood needed = 160 ml/kg • One or two central catheters are placed. • Small aliquots of blood are removed and replaced with aliquots of donor blood. • Electrolytes and bilirubin should be checked periodically during the procedure.

BIND: Bilirubin-Induced Neurologic Damage v Spectrum of subtle neurologic findings which can manifest as disorders of vision, hearing, gait, speech/language and cognition. v ACUTE Bilirubin Encephalopathy: acute neurotoxicity seen in the first weeks after birth. v 3 phases 1. Early with subtle signs: sleepy, mild-moderate hypotonia, high pitched cry. 2. Intermediate phase: febrile, poor suck, lethargy or irritable/jittery, shrill cry, backward arching neck and trunk. 3. Advanced: apnea, poor feeding, fever, seizure, semicomatose/coma. Kernicterus: chronic and permanent sequelae of BIND. v Choreoathetoid CP, sensorineural hearing loss, paralysis of upward gaze, dental enamel dysplasia.

Relationship of Albumin-Bound and Unbound Bilirubin Levels in the Vascular Space to the Entry and Clearance from the Central Nervous System (CNS). Watchko JF, Tiribelli C. N Engl J Med 2013; 369: 2021 -2030

Cell Types and Metabolic Processes Affected by Bilirubin in the CNS. Watchko JF, Tiribelli C. N Engl J Med 2013; 369: 2021 -2030

BIND score Scores Mental status 0 1 2 3 Muscle tone 0 1 2 Clinical sign Normal Sleepy, poor feeding Lethargic, irritable, jittery Unable to feed, apnea, seizures, coma fisting, Normal flexed tone (awake) Hypertonia alternating with hypotonia Neck stiffness, flexor spasm, beginning of neck and back arching, hypertonia Persistent retrocollis and opisthotonos, bicycling, twitching of hands and feet, severe hypotonia with limp posture Cry pattern 0 1 2 3 Total score Normal High pitched cry Shrill cry even if intermittent Weak or absent cry. Inconsolable cry Sum of highest score in each category 3 El Houchi SZ et al J Pediatr 2017; 183: 51

Relationship of neurologic and auditory outcomes to BIND scores 3 -5 mo Neurologic follow-up findings AABR follow -up HIGHEST BIND SCORES Normal REFER BIND (0) BIND (1 -3) 2 BIND (4 -6) BIND (7 -9) 32 71 Subtle 0 1 CBE 0 1 Bilateral PASS 32 71 15 3 6 15 0 0 16 0 Conclusions: BIND score is a strong predictor of neurologic sequelae. Infants with BIND score of 3 -4 or greater, irrespective of TSB, should received immediate intensive phototherapy and preparations made for exchange should phototherapy fail to decrease TSB rapidly. 0 9 16
 Underlying etiology: Idiopathic: G 6 PD 19 patients")
KERNICTERUS Pilot Kernicterus Registry (61 patients) Underlying etiology: Idiopathic: G 6 PD 19 patients deficiency: 19 patients Hemolysis Bruising (non G 6 PD): 10 patients from birth trauma: 6 patients Infection: 4 patients Crigler-Najjar or galactosemia: 3 patients All but one was breastfed. 16 of the patients lost >10% of birthweight at readmission. Johnson LH et al. J Pediatr

What about REBOUND? AAP recommends discontinuing phototherapy when TSB <14 for readmitted infants, but gives no specific recommendations for the birth hospitalization. Chang et al devised a Prediction Rule for Rebound Hyperbilirubinemia following inpatient phototherapy. (Pediatrics, March 2017). Probability of rebound hyperbilirubinemia by score: Score = 15 (if gestational age <38 weeks) − 7 × (age in days at phototherapy initiation) − 4 × (AAP phototherapy threshold − TSB at phototherapy termination) + 50. Probability of rebound <10% with score <30 Probability of rebound <4% with score <20

Probability of rebound hyperbilirubinemia by score. Pearl W. Chang et al. Pediatrics 2017; 139: e 20162896

Evolutionary considerations? What evolutionary advantage is there for the human body to convert biliverdin (water soluble) to bilirubin and then back to a water soluble form for excretion via an energy dependent process? Low concentrations of bilirubin may have some antioxidant benefits, suggesting it should not be completely eliminated. Antioxidant defense in the neonate is poorly developed. SO… should we consider hyperbilirubinemia a transitional mechanism in the neonatal circulation, whereby high bilirubin levels provide “back up” to the neonate with a weak immune system and antioxidant defense?

In conclusion… For 1. 2. 3. 4. every infant: Promote and support successful breastfeeding. Perform a systematic assessment before discharge for the risk of severe hyperbilirubinemia. Obtain a pre-discharge screening TSB or transcutaneous bilirubin and provide early, focused follow-up based on the risk assessment. When indicated, treat newborns with phototherapy or exchange transfusion to prevent the development of severe hyperbilirubinemia and BIND.
- Slides: 31