Hydrocephalus Ventriculoperitoneal shunt Diana Tnase Ventricular system Hydrocephalus



 1. obstructive (AKA noncommunicating): block")





 B. Chiari Type")



: 1. beaten")







 shunt: A. most commonly")



: places catheter in frontal horn. The right side is usually")
 or external ventricular drainage (EVD). INSERTION TECHNIQUE The")








 1. flat in bed 2. if peritoneal end is")










- Slides: 48
Hydrocephalus Ventriculo-peritoneal shunt Diana Tănase
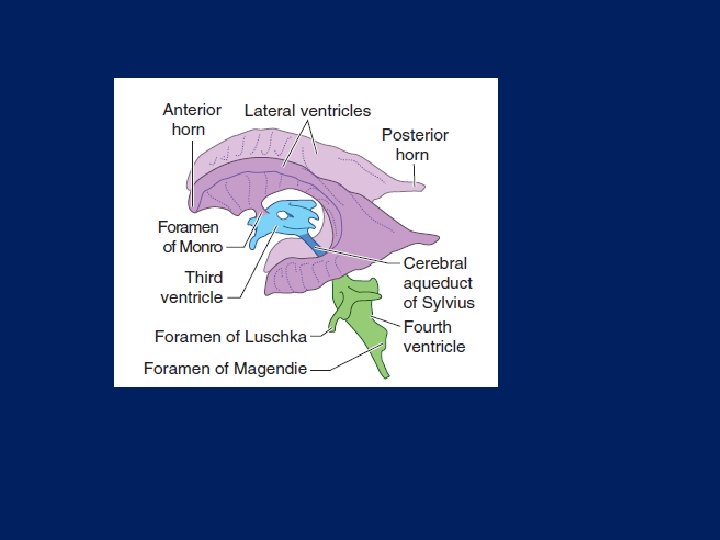
Ventricular system
Hydrocephalus Etiology • subnormal CSF reabsorption • rarely CSF overproduction …which result in accumulation of CSF in the ventricular system
FUNCTIONAL CLASSIFICATION Two main functional subdivisions of hydrocephalus (HCP) 1. obstructive (AKA noncommunicating): block proximal to the arachnoid granulations(AG). 2. communicating (AKA non-obstructive): CSF circulation blocked at level of AG
SPECIAL FORMS OF HYDROCEPHALUS AND "PSEUDOHYDROCEPHALUS" 1. conditions that are not actually hydrocephalus "pseudohydrocephalus" A. hydrocephalus ex vacuo: cerebral atrophy B. otitic hydrocephalus C. external hydrocephalus D. Hydranencephaly 2. normal pressure hydrocephalus (NPH) 3. entrapped fourth ventricle 4. arrested hydrocephalus
Normal pressure hydrocephalus -adult form of hydrocephalus- As originally described, the hydrocephalus of NPH was considered to be idiopathic. "secondary NPH“ causes: 1. post-SAH 2. post-traumatic 3. post-meningitis 4. following posterior fossa surgery 5. tumors 6. also seen in some patients with Alzheimer's disease (AD) 7. deficiency of the arachnoid granulations 8. aqueductal stenosis
Clinical triad Hakim triad 1. gait disturbance 2. dementia: primarily memory impairment with bradyphrenia (slowness of thought) and bradykinesia 3. urinary incontinence
Other clinical features Age usually> 60 yrs. Slight male preponderance. Differential diagnosis - Alzheimer's disease - Parkinson's disease
Hydrocephalus Classification • Congenital • Acquired
Congenital, usually paediatric A. Chiari Type 2 malformation and/or myelomeningocele (MM) B. Chiari Type 1 malformation C. primary aqueductal stenosis of Sylvius aqueduct D. secondary aqueductal gliosis E. Dandy Walker malformation: atresia of foramina of Luschka & Magendie F. X-linked inherited disorder: rare
Acquired A. infectious 1. post-meningitis 2. cysticercosis B. post-hemorrhagic 1. post-SAH 2. post-intraventricular hemorrhage (IVH) C. secondary to masses 1. non neoplastic: e. g. vascular malformation 2. neoplastic: e. g. Medulloblastoma, pituitary tumor D. post-op: following p-fossa tumor removal. E. Neurosarcoidosis F. "constitutional ventriculomegaly": asymptomatic. No treatment required. G. associated with spinal tumors
DIFFERENTIAL DIAGNOSIS OF HYDROCEPHALUS Conditions that may mimic HCP but are not due to inadequate CSF absorption include: 1. atrophy: sometimes referred to as "hydrocephalus ex vacuo" 2. hydranencephaly 3. developmental anomalies where the ventricles appear enlarged: A. agenesis of the corpus callosum B. septa-optic dysplasia
SIGNS AND SYMPTOMS OF ACTIVE HCP In young children 1. cranium enlargement 2. irritability, poor head control, NN 3. fontanelle full and bulging 4. enlargement and engorgement of scalp veins 5. Macewents sign: cracked pot sound on percussing over dilated ventricles 6. 6 th nerve (abducens) palsy 7. "setting sun sign" (upward gaze palsy) 8. hyperactive reflexes 9. irregular respirations with apneic spells 10. splaying of cranial sutures In older children/adults with rigid cranial vault Symptoms of increased ICP, including: - papilledema, - HI A, - NN, - gait changes, - upgaze and/or abducens palsy. Slowly enlarging ventricles may initially be asymptomatic.
CHRONIC HCP Features indicative of chronic hydrocephalus (as opposed to acute hydrocephalus): 1. beaten copper cranium on plain skull x-ray. 2. 3 rd ventricle herniating into sella (seen on CT or MRI) 3. erosion of sella turcica 4. the temporal horns may be less prominent on CT than in acute HCP 5. Macrocrania 6. atrophy of corpus callosum 7. in infants A. sutural diastasis B. delayed closure of fontanelles C. failure to thrive or developmental delay
CT/MRI CRITERIA OF HYDROCEPHALUS Hydrocephalus HCP is suggested when either: A. both TH ≥ 2 mm in width OR B. both TH ≥ 2 mm + ratio FH/ID > 0. 5 TH= temporal horns FH= the largest width of the frontal horns ID= the internal diameter
Other features suggestive of hydrocephalus: 1. ballooning of frontal horns of lateral ventricles ("Mickey Mouse" ventricles) and/or 3 rd ventricle 2. periventricular low density on CT
3. used alone, the ratio FH/ID <40% normal 40 -50% borderline >50% suggests hydrocephalus 4. Evans ratio (or index): ratio of FH to BPD measured in the same CT slice: > 0. 3 suggests hydrocephalus 5. sagittal MRI may show thinning and/or upward bowing of the corpus callosum BPD= maximal biparietal diameter
Treatment of hydrocephalus MEDICAL Acetazolamide may be helpful for temporizing. Diuretic therapy may be tried in premature infants with bloody CSF. This should only be considered as an adjunct to definitive treatment or as a temporizing measure. • acetazolamide (a carbonic anhydrase inhibitor): 25 mg/kg/day • simultaneously start furosemide: 1 mg/kg/day • to counteract acidosis: + tricitrate 4 ml/kg/day + measure serial electrolytes, and adjust dosage to maintain serum HCO 3 > 18 m. Eq/L • watch for electrolyte imbalance and acetazolamide side effects: lethargy, tachypnea, diarrhea, paresthesias (e. g. tingling in the fingertips) • perform weekly U/S or CT scan and insert ventricular shunt if progressive ventriculomegaly occurs. Otherwise, maintain therapy for a 6 month trial, then taper dosage over 2 -4 weeks. Resume 3 -4 mos of treatment if progressive HCP occurs
SPINAL TAPS HCP after intraventricular hemorrhage may be only transient Serial taps (ventricular or LP) may temporize until resorption resumes but LPs can only be performed for communicating HCP. If reabsorption does not resume when the protein content of the CSF is< 100 mg/dl, then it is unlikely that spontaneous resorption will occur (i. e. a shunt will usually be necessary).
SURGICAL Goals of therapy: Normal sized ventricles is not the goal of therapy. Goals are optimum neurologic function and a good cosmetic result. Options include: 1. choroid plexectomy: for communicating hydrocephalus May reduce the rate but does not totally halt CSF production (only a portion of CSF is secreted by the choroid plexus, other sources include the ependymal lining of the ventricles and the dural sleeves of spinal nerve roots). 2. eliminating the obstruction: e. g. opening a stenosed sylvian aqueduct. 3. third ventriculostomy 4. shunting
Third ventriculostomy Indications: - used in patients with obstructive HCP - an option in managing shunt infection - an option for patients who developed subdural hematomas after shunting - for slit ventricle syndrome. Contraindications: Communicating hydrocephalus Complications: 1. hypothalamic injury 2. transient 3 rd and 6 th nerve palsies 3. uncontrollable bleeding 4. cardiac arrest 5. traumatic basilar artecy aneurysm Success rate: ~56% Highest maintained patency rate is with previously untreated acquired Aq. S. There is a low success rate (only ~20% of TVs will remain patent) if there is pre-existing pathology including: 1. tumor 2. previous shunt 3. previous SAH 4. previous whole brain radiation 5. adhesions
TYPES OF SHUNTS SHUNT TYPE BY CATEGORY 1. ventriculoperitoneal (VP) shunt: A. most commonly used shunt B. lateral ventricle is the usual proximal location 2. ventriculo-atrial (VA) shunt ("vascular shunt"): A. ventricles -> jugular vein -> superior vena cava B. treatment of choice when abdominal abnormalities are present 3. Torkildsen shunt: A. shunts ventricle to cisternal space B. rarely used C. effective only in acquired obstructive HCP
TYPES OF SHUNTS 4. miscellaneous: used historically or in patients who have had significant problems with traditional shunt locations: A. pleural space (ventriculopleural shunt): not a first choice, but a viable alternative if the peritoneum is not available. B. gall bladder C. ureter or bladder: causes electrolyte imbalances 5. lumboperitoneal (LP) shunt - only for communicating HCP 6. cyst or subdural shunt: from arachnoid cyst or subdural hygroma cavity, usually to peritoneum
Shunts Ventricular catheterization Most common insertion sites: 1. occipital-parietal region: commonly used for CSF shunt A. entry site: a number of means have been described, including: 1. Frazier burr hole: placed prophylactically before p-fossa crani for emergency ventriculostomy in event of postop swelling. Location: 3 -4 cm from midline, 6 -7 cm above inion 2. parietal boss 3. follow point from mid-pupillary line parallel to sagittal suture until it intersects line extending posteriorly from the top of the pinna 4. ~3 cm above and ~3 cm posterior to top of pinna B. trajectory: insert the catheter parallel to skull base: - aim for middle of forehead C. insertion length: ideally, the tip should be just anterior to the foramen of Monro in the frontal horn.
3. Dandy's point: 2 cm from midline, 3 cm above inion (may be more prone to damage visual pathways than above) 2. Keen's point (posterior parietal): (placement in trigone) 2. 5 -3 cm posterior and 2. 5 -3 cm superior to pinna
4. Kocher's point (coronal): places catheter in frontal horn. The right side is usually used. Commonly employed for ICP monitors A. entry site: 2 -3 cm from midline which is approximately the mid-pupillary line with forward gaze, 1 cm anterior to coronal suture (to avoid motor strip) B. trajectory: direct catheter perpendicular to surface of brain, aiming in coronal plane towards medial canthus of ipsilateral eye and in AP plane towards EAM C. insertion length: advance catheter with stylet until CSF is obtained (should be < 5 -7 cm depth; this may be 34 cm with markedly dilated ventricles). Advance catheter without stylet 1 cm deeper. CAUTION: if CSF is not obtained until very long insertion length (e. g. ≥ 8 cm) the tip is probably in a cistern (e. g. prepontine cistern) which is undesirable
Ventriculostomy/ICP monitor AKA intraventricular catheter (IVC) or external ventricular drainage (EVD). INSERTION TECHNIQUE The right (non-dominant) side is preferred. Five minute Betadine prep. Site: approximately Kocher's point. To avoid motor strip, enter 1 -2 cm anterior to coronal suture *estimated position of coronal suture: follow line up midway between lateral canthus and EAM, and to avoid the sagittal sinus, 2 -3 cm lateral to midline. Incision oriented in sagittal plane; elevate periosteum; place self-retaining retractor; make twist drill hole. Bone-wax edges to stop bone bleeding; cauterize dura with bipolar coagulator; incise dura in cruciate fashion with #11 scalpel blade; cauterize incised dural edges and then pia/arachnoid with bipolar.
For ventriculostomy: insert catheter perpendicular to brain surface to a depth of 5 -7 cm. With any ventricular enlargement, CSF should flow at least by 3 -4 cm depth. If no CSF is encountered here and the catheter is passed further until CSF is obtained, it is unlikely to be due to catheterization of frontal horn of lateral ventricle. If unsuccessful after a maximum of three attempted passes, then place a subarachnoid bolt or intraparenchymal monitor.
REMOVAL Patients receiving anticoagulants need to have normal coagulation and platelet function before discontinuing the catheter to reduce the risk of intracranial hemorrhage. For heparin and LMW heparin, stop the drug 24 hours prior to discontinuing the drain. SUMP DRAINAGE The tip of a 25 gauge butterfly may be bent at a 90° angle, and inserted into a subcutaneous reservoir for prolonged ventricular drainage. The use of a one-way valve, continuous antibiotics (ampicillin and cloxacillin) and meticulous technique was credited for the lack of infection.
Ventricular shunts 1. position: supine with shoulder roll 2. Implants 3. equipment: A. C-arm for ventriculo-atrial shunts B. endoscopic display (e. g. If Neuro. Pen is used) C. image guided navigation system (infrequently used) 4. consent (in lay terms for the patient- not all-inclusive): A. procedure: surgery to insert a permanent drainage tube from the brain to the abdomen, outside of the lungs, vein near the heart (as appropriate) to drain excess cerebrospinal fluid B. alternatives: nonsurgical management (rarely effective for hydrocephalus), third ventriculostomy (for certain cases) C. complications: infection, suboptimal position which might require re-operation, failure to relieve hydrocephalus/symptoms, subdural hematoma, bleeding in the brain, shunts are mechanical devices and will eventually fail (break, block up, move. . . ) and need repair/replacement (sometimes sooner rather than later). Abdominal shunts: risk of bowel injury (which could require further surgery)
Ventricular catheter Occipital burr hole is used in most cases for insertion site of ventricular catheter. Some prefer a frontal burr hole (Kocher's point) citing a lower incidence of failure from choroid plexus occlusion. An inverted "J" shaped incision is used to keep hardware from lying directly under the skin incision (minimizes risk of skin breakdown and also creates additional barrier to infection of subjacent hardware). CSF should be sent for culture at the time of insertion since it has been estimated that in 3% of patients the CSF is already infected. 4 mg of preservative-free gentamicin may be instilled into the ventricular catheter by the technique of barbotage. If you think the catheter is in the ventricle, but you don't get CSF flow, it may be due to low pressure, you can compress the jugular veins or lower the head of the bed to try and induce CSF flow. Connectors If a connector must be used near the clavicle, placing it below the clavicle increases the risk of disconnection vs. placing the connector above the clavicle.
DISTAL CATHETER PLACEMENT The general order of preference for distal catheter placement: 1. peritoneal cavity 2. pleural space 3. right atrium or superior vena cava 4. less frequently used distal shunt sites A. gall bladder B. internal jugular vein C. superior sagittal sinus
VENTRICULOPERITONEAL SHUNT Peritoneal catheter For small children, use at least 30 cm length of intraperitoneal tubing to allow for continued growth (120 cm total length of peritoneal tubing recommended). A silver clip is placed at the point where the catheter enters the peritoneum so that the amount of residual intraperitoneal catheter can be determined on later films. Distal slits on the peritoneal catheter may increase the risk of distal obstruction, and some authors recommend that they be trimmed off.
Open technique: A vertical incision lateral and superior to the umbilicus is one of several choices. Layers 1. subcutaneous fat 2. anterior rectus sheath 3. abdominis rectus muscle fibers: should be split longitudinally 4. posterior rectus sheath 5. preperitoneal fat 6. peritoneum
Trocar technique: 1. place a Foley catheter to decompress the bladder 2. 1 cm skin incision above and lateral to the umbilicus 3. pull abdominal skin anteriorly (away from patient) 4. insert trocar aiming toward the ipsilateral iliac crest 5. feel 2 "pops" of penetration: 1 = anterior rectus sheath, 2 = posterior rectus sheath/peritoneum 6. peritoneal catheter should feed easily through trocar
VP SHUNT, POST-OP ORDERS (ADULT) 1. flat in bed 2. if peritoneal end is new or revised, do not feed until bowel sounds resume (at least 24 hrs) 3. shunt series (AP & lateral skull, and chest/ abdominal x-ray) as baseline for future comparison
Disadvantages/complications of various shunts Those that may occur with any shunt: A. obstruction: the most common cause of shunt malfunction - proximal: ventricular catheter (the most common site) - valve mechanism - distal B. disconnection at a junction, or break at any point C. infection D. hardware erosion through skin, usually only in debilitated patients E. seizures (ventricular shunts only) Seizure risk is questionably higher with frontal catheters than with parieto-occipital. F. act as a conduit for extraneural metastases of certain tumors (e. g. medulloblastoma). Low risk. G. silicone allergy: rare. May require fabrication of a custom silicone-free device (e. g. polyurethane)
Disadvantages/complications of VP shunts: A. inguinal hernia B. need to lengthen catheter with growth C. obstruction of peritoneal catheter D. peritonitis from shunt infection E. hydrocele F. CSF ascites
G. tip migration - into scrotum - perforation of a viscus: stomach, bladder - through the diaphragm H. intestinal obstruction (as opposed to perforation): rare I. volvulus J. intestinal strangulation K. overshunting: more likely than with VA shunt. Some recommend LP shunt for communicating hydrocephalus.
MISCELLANEOUS SHUNT HARDWARE 1. tumor filter: used to prevent peritoneal or vascular seeding in tumors that may metastasize through CSF (e. g. medulloblastoma, PNETs, ependymoma); may eventually become occluded by tumor cells and need replacement; 2. antisiphon device: prevents siphoning effect when patient is erect 3. "horizontal-vertical valve" (H-V valve) used with LP shunts to increase the valve resistance when the patient is vertical to prevent overshunting 4. variable pressure valves that may be externally programmed 5. on-off device: used to open or occlude shunt system by external manipulation of shunt
Programmable shunt valves – Components • Inlet occluder • Reservoir • Outlet occluder One-way valve Pressure settings
Shunt problems • Problems associated with shunt insertion • Problems in patients with established CSF shunt
Problems associated with shunt insertion 1. intraparenchymal or intraventricular hemorrhage 2. Seizures 3. malposition A. of ventricular catheter B. of distal catheter 4. infection
Problems in patients with established CSF shunt Shunt "problems" usually involve one or more of the following: 1. Undershunting 2. infection 3. overshunting: slit ventricle syndrome, subdural hematomas 4. seizures 5. problems related to the distal catheter A. peritoneal B. atrial 6. skin breakdown over hardware: infection or silicone allergy 7. hemorrhage at time of insertion: uncommon in pediatrics
Overshunting -slit ventricles- -subdural hematomas-
TAPPING A SHUNT aka aspirating a shunt Indications to tap a shunt or ventricular access device include: 1. to obtain CSF specimen A. to evaluate for shunt infection B. for cytology C. to remove blood 2. to evaluate shunt function A. measuring pressures B. contrast studies: 3. as a temporizing measure to allow function of a distally occluded shunt 4. to inject medication A. antibiotics: for shunt infection or ventriculitis B. chemotherapeutic (antineoplastic) agents 5. for catheters placed within tumor cyst (not a true shunt): A. periodic withdrawal of accumulated fluid B. for injection of radioactive liquid (usually phosphorous) for ablation