Human Sexuality Sexual Health Objectives n Define sexual

Human Sexuality/ Sexual Health

Objectives n Define sexual health including dimensions of sexual health n Explain the etiology, pathophysiology, manifestations, complications & collaborative care of clients with common sexually transmitted diseases: gonorrhea, Chlamydia, syphilis, genital herpes & HPV (warts)

Discuss sexual assault including risk factors, injuries, complications, collection of evidence, prevention and nursing care in cases of assault. n Discuss the etiology, pathophysiology, manifestations, complications & collaborative care of clients with common female reproductive disorders: menstrual & uterine disorders, menopause. n Discuss the etiology, pathophysiology, manifestations, complications & collaborative care of clients with common male reproductive disorders: BPH, prostatitis, prostate cancer, testicular disorders, penile disorders. n

Learning Activities n In your text readings: Chapter 46, 47 & 49. n Society of Obstetricians & Gynecologists of Canada n Public Health Agency of Canada n Canadian Justice System n BPH

General Concepts n n n n Human sexuality Sexually transmitted diseases Sexual assault & family violence Prostatic & scrotal disorders Testicular & penile disorders Menstrual disorders Menopause Uterine disorders

Things to Think About…. n n n n What is Sexuality/Sexual Health? Define In what ways does sexuality impact health? (POSITIVE AND NEGATIVE) What role do nurses play in sexual health? What strategies can nurses use, individually and as a group, to ensure sexuality is part of care provided? How good a job are nurses doing in addressing the last question? What can we do differently? How does the media impact on sexual health?

Human Sexuality is complex, multidimensional phenomenon, and changes that occur in one area may occur in another n A basic human drive (Oncology Nursing Society) n It involves the physical, psychological, social emotional and spiritual components of an individual n WHO defines sexuality using a holistic approach “positive integration of somatic, emotional, intellectual, & social aspects of being sexual beings in ways that are positively enriching & that enhance personality, communication & love” n

Human Sexuality Other components of sexuality are freedom from shame, fear, guilt & misconceptions, & other psychological factors that inhibit sexual responses. n An important component of sexuality is freedom from organic diseases & disorders that may interfere with sexual responses & reproduction (WHO). n

Our Views About Human Sexuality Are Determined By: n Social rules n Genetic endowment n Cultural rules n Biology – sexual orientation n Psychology – upbringing, values/morals, influences

Human Sexuality Each society has rules governing sexual behavior & there is no universal agreement on what is considered normal.

Sexual Orientation Various theories have proposed differing sources for sexual orientation, including genetic or hormonal factors & life experiences during early childhood n However many scientists share the view that sexual orientation is shaped for most people at an early age through complex interactions of biological, psychological & social factors n

“Psychologists, psychiatrists and other mental health professionals agree that homosexuality is not an illness, mental disorder or emotional problem. Much objective scientific research over the past 35 years shows us that homosexual orientation, in and of itself, is not associated with emotional or social problems”.

Sexual Health n Health is not just absence of illness. It includes positive striving for wellness & taking responsibility for the early detection of potential problems & their treatment n Sexual health must be addressed by HCP n The relationship between self-esteem & bodyimage is involved in how we monitor our health & act promptly on signs of illness

Three Dimensions of Sexual Health n Sexual function n Sexual self-concept/gender identity: gender identity (psychological sense of being male or female) n Sexual relationships/social sex role: adherence to cultural norms for feminine & masculine behavior)

Sexual & Reproductive Health Basic Premises: n Each individual is responsible n Preventing is always better than treating a condition n Seek early diagnosis and treatment

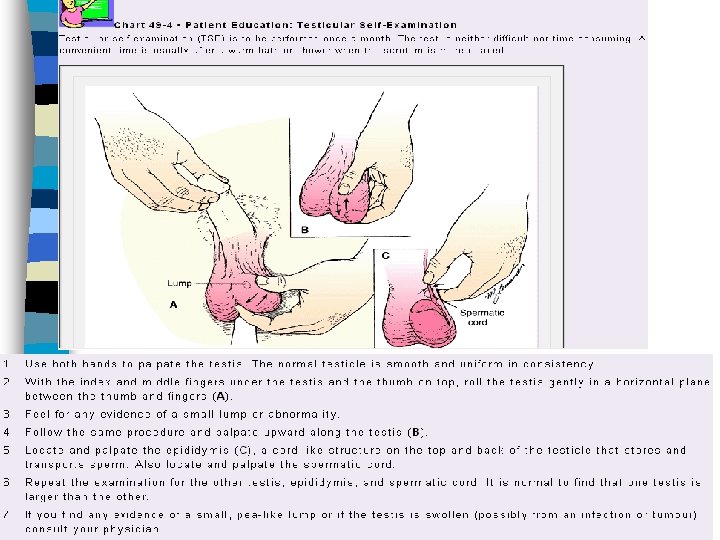
Common Examinations : Sexual/ Reproductive Health • • • Breast self-examination Breast examination by physician/nurse Pap smear & Mammograms Testicular self examination Testicular examination by physician DRE for prostate assessment
 Test n n n Begin at age 18 (earlier if sexually active)")
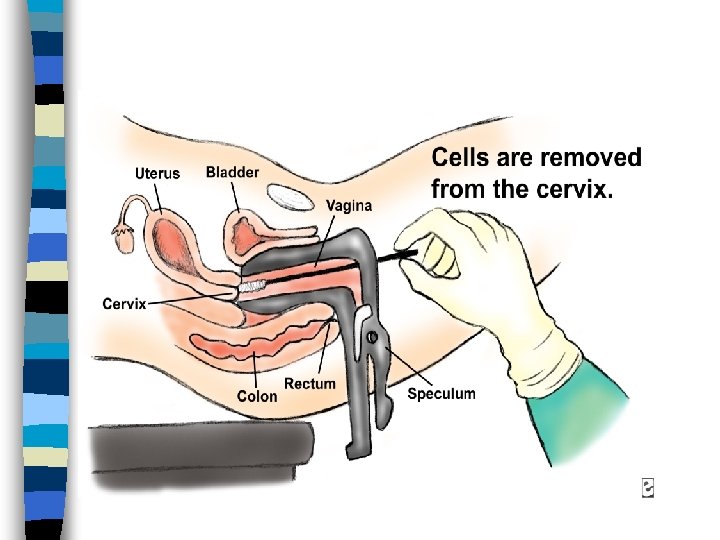
Papanicolaou (Pap) Test n n n Begin at age 18 (earlier if sexually active) Schedule test for 1 - 2 weeks after LMP Abstain from sexual intercourse 24 -48 hrs before test Do not use douching, vaginal medicines or spermicidal foams, creams, or jellies 48 hrs before test Inform HCP if HPV or STI

Pap Test: Saves LIVES!!!! n The pap smear test is the only screening test that causes a decrease in occurrences and deaths from cancer

Testicular Self Examination n n Examine each testicle separately & in comparison to the other Best to do after warm bath/shower Be aware of the epididymus (slightly tender & tube like body behind the testicle is normal) Should be done monthly Most common cancer between 20 -34

Sexually Transmitted Infections
")
Sexually Transmitted Infections Any infection contracted through sexual activities or contact (oral, anal, vaginal) n More than 50 organisms can spread via sexual contact n 5 common STI: Gonorrhea Syphilis Chlamydia Genital Herpes Genital HPV (Warts) n

STI’s share the following Characteristics: Transmitted by any sexual activity between opposite-sex or same–sex partners 1. Having one STI confers no immunity on future reinfection with that STI or with any other STI 2. Sexual partners of clients need to be assessed for treatment 3. STI’s affect people from all socioeconomic classes, cultures, age groups 4. Women bear a disproportionate number of the effects of STI’s 5. Frustration, anger, fear, shame & guilt are emotions associated with STI’s 6. STI’s frequently coexist in the same client (Gonorrhea & Chlamydial)

Etiology STI’s Caused by : 1. Bacteria: Gonorrhea, Chlamydia, Syphilis, Bacterial Vaginosis, Nongonococcal Urethritis 2. Viruses: AIDS, Genital herpes & genital warts, Hep A, B, C 3. Protozoa: Trichomoniasis 4. Yeast: Vulvovaginal candidiasis 5. Ectoparasites: Scabies & Pediculosis pubis

Risk Factors for Acquiring STI’s Sexual contact with an infected person n – A new sexual partner or more than two sexual partners in the past year n – Previous sexually transmitted infections (STIs) n – Vulnerable populations (e. g. , injection drug users, incarcerated individuals, sex trade workers, street youth etc. ) n–

STI Prevention Health promotion & prevention should focus on 5 major concepts: 1. Education 2. Early Detection 3. Effective DX & RX 4. Evaluation & treatment sexual partners 5. Pre-exposure vaccination if available

Prevention & Management STI’s n n n Assessing the reason for a consultation. Knowing about STI risk factors and epidemiology. Performing a brief client history and STI risk assessment. Providing client-centred education and counselling. Performing a physical examination. Selecting appropriate screening/testing. Diagnosing by syndrome or by organism and posttest counselling. Treating. Reporting to public health and partner notification. Managing co-morbidity and associated risks. Following up.

Assessment should consist of: 1. General health & examination 2. Sexual history, preferences & practices 3. Previous history STI’s 4. Specific complaints (60 -80% asymptomatic) 5. Genital health practices (douching) 6. Contraceptive history 7. Infection barriers used

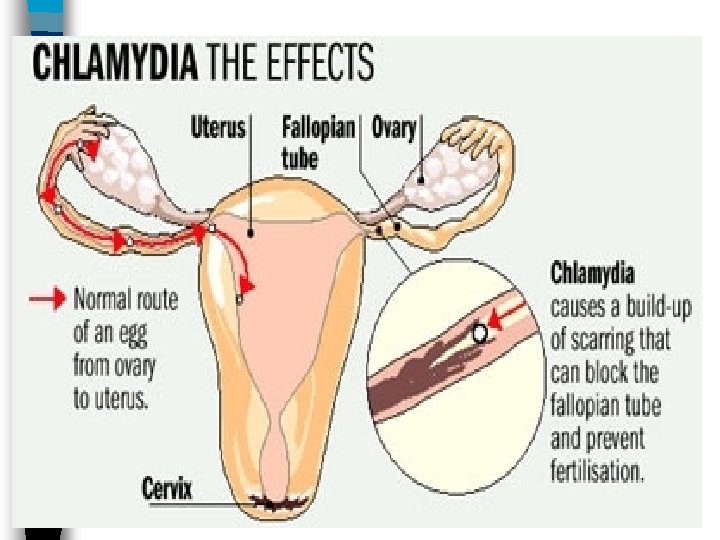
Chlamydial Infections n n n Most common bacterial STI Caused by Chlamydia trachomatis (gram -) transmitted during vaginal, anal, oral sex Underreported most people asymptomatic Incubation period 1 -3 weeks High incidence reoccurrence due to lack of treating sexual partners infected

Chlamydia

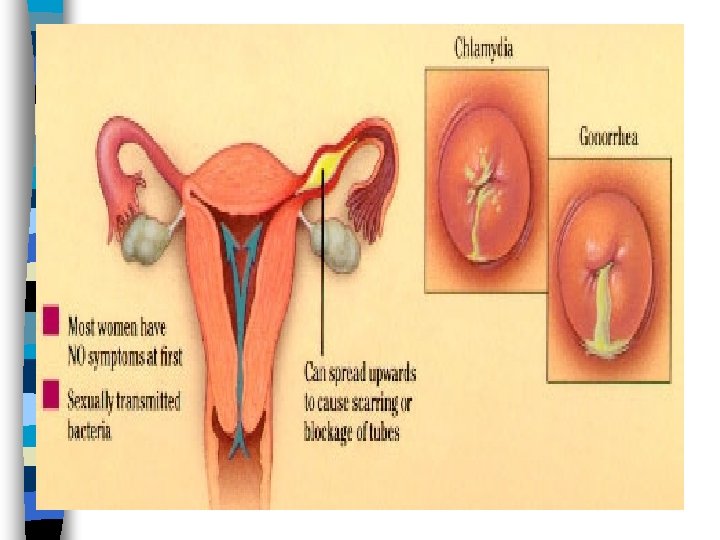
Manifestations n n n n n Females Most often asymptomatic Vaginal discharge Dysuria Lower abdominal pain Abnormal vaginal bleeding Dyspareunia Conjunctivitis Proctitis (commonly asymptomatic) n n n n n Males Often asymptomatic Urethral discharge Urethral itch Dysuria Testicular pain Conjunctivitis Proctitis (commonly asymptomatic) Neonates and infants n Conjunctivitis in neonates n Pneumonia in infants n <6 months of age n

Chlamydia

Complications Chlamydial Infections Men: n Epididymo-orchitis n Reiter syndrome Women: n Pelvic inflammatory disease n Ectopic pregnancy n Infertility n Chronic pelvic pain n Reiter syndrome

Epididymo-Orchitis

Reiter’s Syndrome Reactive Arthritis

Diagnosis of Chlamydial Infections n n n Presentation No definitive test for fast accurate dx Tissue culture of cellular material from urethral, endocervix or rectum Rapid non culture test- urogenital secretions to detect C. trachomatis EIA test ( enzyme immunoassay specimen) 10 -20 mls urine
 100 mg bid X 7 days n Zithromax 1")
Treatment Chlamydial Infections Doxycycline (Vibramycin) 100 mg bid X 7 days n Zithromax 1 g in a single dose (if ability to comply an issue) n Alternative regimes: n Erythromycin, Floxin, Levaquin Follow-up care: n Return if symptoms persist or recur n Treatment all sex partners n Use of condoms during all sexual contacts n

Gonorrhea n n n n Second most common STI Highest among people under 24 yrs. Living in high-density urban areas , multiple partners & unprotected sex Caused by Neisseria Gonorrhoeae (gram – diplococcus) Direct physical contact with infected host Mucosa with columnar epithelium susceptible (urethra-males; cervix, rectum, oropharynx) Neonates can develop during delivery infected mother Incubation period 3 to 4 days

Gonorrhea

Manifestations Females n Cervicitis n PID n Urethritis n Perihepatitis n Bartholinitis Males n Urethritis n Epididymitis Females & Males n Pharyngeal infection n Conjunctivitis n Proctitis n Disseminated gonococcal infection: – – arthritis, dermatitis, endocarditis, meningitis

Symptoms of Genital Tract Infection With N gonorrhoeae Females n Vaginal discharge n Dysuria n Abnormal vaginal bleeding n Lower abdominal pain n Rectal pain and discharge if proctitis n Deep dyspareunia Males n Urethral discharge n Dysuria n Urethral itch n Testicular pain, swelling or symptoms of epididymitis n Rectal pain and discharge if proctitis

Gonorrhea


Complications n n n n Females Pelvic inflammatory disease Infertility Ectopic pregnancy Chronic pelvic pain Reiter syndrome Disseminated gonococcal infection n n Males Epididymo-orchitis Reiter syndrome Infertility (rare) Disseminated gonococcal infection

Diagnosis Gonorrhea n History n Physical exam n Identification of gonococcus on smear & culture exudate from infected areas n Cornerstone diagnosis: culture with selective culture media

Treatment Gonorrhea n n n cefixime 400 mg PO in a single dose, OR ciprofloxacin 500 mg PO in a single dose (unless not recommended due to quinolone resistance) OR ofloxacin 400 mg PO in a single dose (unless not recommended due to quinolone resistance) OR ceftriaxone 125 mg IM in a single dose Teach importance identifying & treating all sexual partners Warn pregnant clients of danger of infecting newborns during delivery Take all medications Should be followed by empiric treatment for chlamydial and non-gonococcal infections

Path of a Gonorrhea Infection

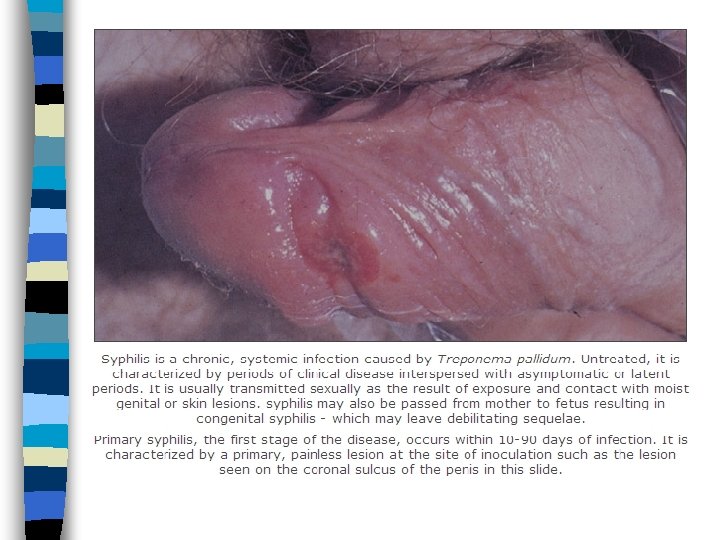
Syphilis Systemic highly infectious STI Caused by delicate motile treponema pallidum ( can’t survive outside body) n Transmitted by vaginal, anal & oral sexual contact n Organism multiplies locally & disseminates systemically thru blood stream & lymphatics n Rarely contracted from nonsexual personal contact, accidental inoculation or blood transfusion (syphilic donor) n n

Stages of Syphilis Primary Secondary Latent Tertiary

Primary Stage n Appearance of genital chancre n Chancre develops at site inoculation (anus, mouth, genital) 4 weeks after initial infection

Syphilis

Secondary Stage Develops 6 -8 weeks if primary not treated n Rash (palms of hands & soles feet) n Generalized non-tender lymphadenopathy n Mucous patches mouth n Flat papules labia, anus, corners mouth n General flu-like symptoms n Alopecia (eyebrows & scalp)

Secondary Syphilis

Latent Stage No manifestations produced n Client has positive blood test but shows no other evidence of Dx n Occurs 1 -2 yrs after primary lesion n

Tertiary Stage: Untreated syphilis can produce irreversible complications: n Chronic bone & joint inflammation, cardiovascular problems (aneurysm), lesions on body, visual, auditory & CNS problems. n Not infectious at this stage but terminal if not treated. n
 by scraping 1")
Syphilis Diagnosis: Health Assessment n Direct lab studies (identifies causal organism) by scraping 1 or 2 lesions dark field microscopy n Indirect labs (identify antibodies) in serum 4 wks after chancre appearance VDRL- most common (false neg. early stages) RPR-antigen to detect antibody for T. pallidum FTA-ABS n

Syphilis Treatment: n n n Parenteral Penicillin all stages Primary & secondary- Penicillin G IM one dose Latent stage-Penicillin G IM 3 X weekly Neurosyphilis-Pen G IV Allergic Pen G use doxycycline or tetracycline po X 2 weeks Clients primary or secondary must abstain from sexual contact for at least 1 month after Rx

Genital Herpes n n n A recurrent , systemic viral infection Most frequent cause genital ulceration Caused HSV (herpes Simplex) type 2 virus Herpes is transmitted while lesion present & 10 days after lesion healed Direct contact with exudate during sex or fomites (towels) Newborns can be infected during vag delivery

Manifestations Genital Herpes n n n Mild or unrecognized dx Genital herpes manifests 3 -7 days post contact Burning sensation (paresthesia) noted at site of inoculation Then, numerous small vesicles with erythematous border, form painful, shallow ulcers that crust & heal with scar in 2 -4 wks Reoccurrence major problem

Genital Herpes

Complications : Genital Herpes n Disseminated infections n Meningitis n Myelitis n Spontaneous n Ca abortion cervix n Lower motor neuron damage- atonic bladder, impotence, constipation

Treatment Genital Herpes: n n n n Zovirax, Valtrex or Famvir Not a cure Good genital hygiene Wear loose fitting cotton undergarments Sitz baths Complete drying genital area- hair dryer set on cool Aveeno & Burrows solution relieves burning & itching Pain- codeine & aspirin or local xylocaine

Genital Warts
: One of the most common STI n Caused by HPV (Human")
Genital HPV (Warts): One of the most common STI n Caused by HPV (Human papillomavirus) n Smoking, HIV, drug or alcohol abuse, poor nutrition & fatigue favor development n Discrete single or multiple papillary growths that are white to gray & pink-flesh coloured n Grow to form cauliflower like masses n Men-occur penis or scrotum, around anus or in urethra n Women-vulva, vagina, cervix & perineal area

Genital Warts: n Link ca cervix & vulvar ca Diagnosis: n Appearance of genital warts n Serology & cytologic testing to rule out secondary syphilis, ca or benign neoplasms n Dysplasia PAP smear do colposcopic exam & biopsy

Colposcopy

Genital HPV
 applied directly")
Treatment Genital HPV: n HPV vaccine n 80% TCA (trichloroacetic acid ) applied directly to wart or BCA (bichloroacetic acid) via cotton swab n Podophyllin resin (cytotoxic agent) small external warts (each wart) causes sloughing of skin containing viral particles • Local symptoms (pain, burning) & systemic (dizziness, leukopenia, resp. distress)

Treatment Genital Warts n Liquid nitrogen n Electrocautery n Laser therapy n Interlesional interferon n Surgical incision n Treatment only destroys infected tissue not the virus life long follow-up is required

Website for STI Information n http: //www. phac-aspc. gc. ca/STI- mts/sti_2006/sti_intro 2006_e. html

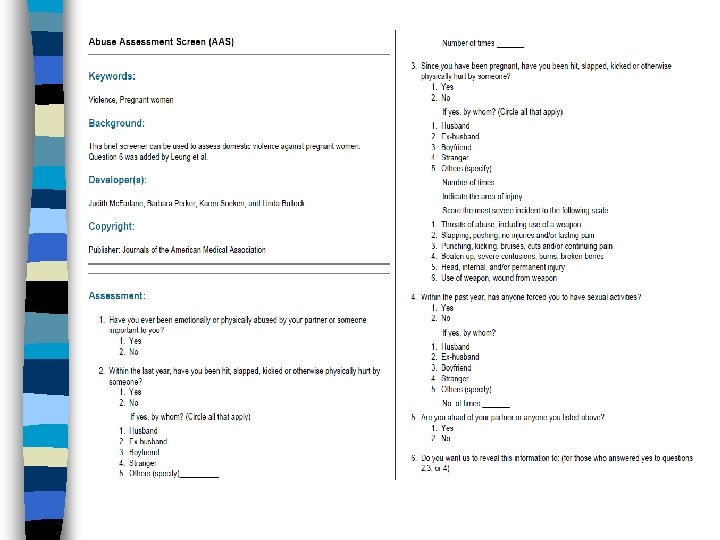
Sexual & Family Violence p. 2413 -16 Text

Family violence n Family violence statistics

The White Ribbon Campaign Men “Working to End Violence Against Women”

Manifestations n physical injuries or n health problems, such as anxiety, insomnia, or gastrointestinal symptoms, that are related to stress. n They usually do not identify their abuser

Indications: Abuse n multiple injuries that are in various stages of healing n injuries are unexplained n explanation does not fit the physical picture.

Indications: Neglect na dependent person with adequate resources and a designated care provider shows evidence of inattention to hygiene, to nutrition, or to known medical needs (eg, unfilled medication prescriptions, missed appointments with health care providers).

Assessment & Diagnosis n n n n Acute awareness of the signs of possible abuse, maltreatment, and neglect. Nurses must be skilled in interviewing techniques to elicit accurate information. A careful history is crucial in the screening process. Careful evaluation & documentation. Assessment of the client's general appearance and interactions with significant others, An examination of the entire surface area of the body, and a Mental status examination.

Management n Primary concern is the safety and welfare of the client n Treatment focuses on the consequences of the abuse, violence, or neglect and on prevention of further injury. n Protocols of most EDs require that a multidisciplinary approach be used. n Respite services n Support groups n NS Adult Protection Act

Sexual Violence n can include the following crimes: – – – – • rape sexual assault incest unwanted touching indecent exposure sexual harassment child molestation All forms are crimes under the Criminal Code

Sexual violence can happen to anyone…at any age…at any place…at any time.

Sexual assault n n n encompasses a wide range of criminal acts in the Criminal Code of Canada. ranges from unwanted sexual touching to sexual violence resulting in serious physical injury or disfigurement to the victim. It also includes special categories of offences designed to protect children from sexual abuse. Sexual assault level 1, (section 271). This involves minor physical injuries or no injuries to the victim. Sexual assault level 2, (section 272). This includes sexual assault with a weapon, threats or causing bodily harm. Aggravated sexual assault level 3, (section 273). This results in wounding, maiming, disfiguring or endangering the life of the victim.

Sexual Assault: Contrary to popular belief, sexual violence is not motivated by sexual desire, it is an act of power, dominance & manipulation n Sexual violence is an attack, attempt to hurt, humiliate & control the victim n Sex is merely the weapon n

Rape Trauma Syndrome: n n n an acute stress reaction to a life-threatening situation acute disorganization phase, which may manifest as an expressed state in which shock, disbelief, fear, guilt, phase of denial and unwillingness to talk about the incident, followed by a phase of heightened anxiety, fear, flashbacks, sleep disturbances, hyperalertness, and psychosomatic reactions phase of reorganization, in which the incident is put into perspective. Some victims never fully recover and go on to develop chronic stress disorders and phobias. Suicidal ideations may occur

Reactions to Sexual Assault: – Fear – Irritability – Anger – Impatience – Humiliation – Insomnia – Depression – Guilt – Eating disorders – Shame – Flashbacks – Self-blame – Helplessness – Revenge
 n The manner in which the client is")
Management Sexual Assault Nurse Examiner (SANE) n The manner in which the client is received and treated in the ED is important to his or her future psychological well-being. n Crisis intervention should begin when the client enters the health care facility. The client should be seen immediately. n Most hospitals have a written protocol that reflects consideration for the victim's physical and emotional needs as well as forensic evidence collection that is required. n

Nursing Management of Sexual Assault Assess & provide care without destroying evidence, remain calm. Encourage discussion about the trauma to the extent that the survivor feels comfortable n Remind the survivor that they are not responsible for the assault –no matter what--and that no one asks or deserves to be raped n Be supportive. Validate the survivor’s reactions to the assault. Avoid saying you know how the survivor feels. No one can ever really know n Be a good listener and avoid judgment/blame n

Nursing Management n Encourage the survivor to seek counseling from specially trained mental health professionals. n Encourage a safety plan n Help them to regain control of their life & support safety n Respect the survivor’s need for privacy. n Get someone they choose to come with them to be assessed.

Medical/legal Issues Post Sexual Assault: The medical/legal attention received after an assault should focus on four areas of treatment and testing: n Treating Injuries (external and internal) ABC n Concerns about pregnancy n Sexually transmitted infections n Protecting evidence in case charges arise

Emergency Management: Sexual Assault Initial: n Treat shock & urgent medical problems (head injury, hemorrhage, wounds , fractures) n Assess emotional state n Contact support person (social worker, rape advocate) n Do not wash client until all evidence is collected n Place sheet on floor, have client stand on it to remove clothing. Place sheet with clothing in paper bag

Initial Emergency Treatment n n n Maintain evidence for all legal specimens. Clearly label evidence & keep in locked cabinet until given to law enforcement agency. Determine method of contraception, date of LMP & Tetanus status. Consider tetanus prophylaxis if lacerations contain soil or dirt Vaccinate with Hepatitis B (if not immunized). Offer Emergency Contraception
 Dried")
Physical examination n n External evidence of trauma (bruises, contusions, lacerations, stab wounds) Dried semen stains (appearing as crusted, flaking areas) on the patient's body or clothes Broken fingernails and body tissue and foreign materials under nails (if found, samples are taken) Oral examination, including a specimen of saliva and prescribed cultures of gum and tooth areas Pelvic and rectal examinations are also performed

Laboratory Evaluation Sexual Assault: n n n Vaginal smears-microscopic evaluation for semen & trichomonads Oral/rectal swabs & smears if indicated Blood samples: VDRL, pregnancy test, HIV & Hep B Cultures: cervix & other areas as indicated for gonorrhea & Chlamydia Fingernail scrapings Pubic hair & clippings of matted pubic hair.

Follow-up Treatment Sexual Assault: n Care of injuries & emotional trauma n Prophylaxis for STI’s , tetanus, Hep B n Pregnancy test 2 -3 weeks n HIV, Syphilis & Hep B 6 -8 weeks n Protection legal rights n Recommendation of continued follow-up & services of rape crisis center.
")
The Medical-legal Kit (also referred to as the rape kit or sexual assault kit) Is completed if a survivor is considering reporting the sexual assault to the police. If a survivor is undecided about reporting, the kit can be completed and the evidence stored, usually for five to twelve months. The kit must be completed within 24 to 72 hours after a sexual assault. • The examination is two to three hours in duration, and is conducted by a physician and/or a nurse.

If Rohypnol use is suspected: • A urine sample should be taken as soon as possible from the victim. Urine collected after 72 hours from ingestion is unlikely to show presence of Rohypnol. • Make sure the urine sample is stored in a liquid-tight container. • The urine sample should be refrigerated or frozen as soon as possible.

Know the Following: 1. What are four reasons for nurses to increase their knowledge and understanding of the impact of sexual assault? 2. Identify and discuss two ways that victims of sexual assault express their emotions? 3. Discuss six common myths and associated facts related to sexual assault. 4. Discuss fears commonly experienced by sexual assault victims. 5. Discuss how nurses can help minimise victims emotional trauma, prevent further victimisation and promote recovery

6. How can nurses assist victims of sexual assault? 7. Discuss legal responsibilities associated with the care of sexual assault victims. 8. Discuss the physical examination and subsequent physical care of victims of sexual assault. 9. As part of nurses' total assessment, why & how should nurses directly question clients about suspicious indications of family related violence? 10. How can nurses support persons who are subjected to family violence?

Family violence: Clinical guidelines for nurses. Ottawa. www. phac-aspc. gc. ca/ncfvcnivf/familyviolence/initiative_e. html www. phac-aspc. gc. ca/ncfvcnivf/familyviolence/html/femexpose_e. html www. phac-aspc. gc. ca/ncfvcnivf/familyviolence/html/fvclinical_e. html www. phac-aspc. gc. ca/ncfvcnivf/familyviolence/famvio_e. html www. justicce. gc. ca/en/ps/fm/familyvfs. html

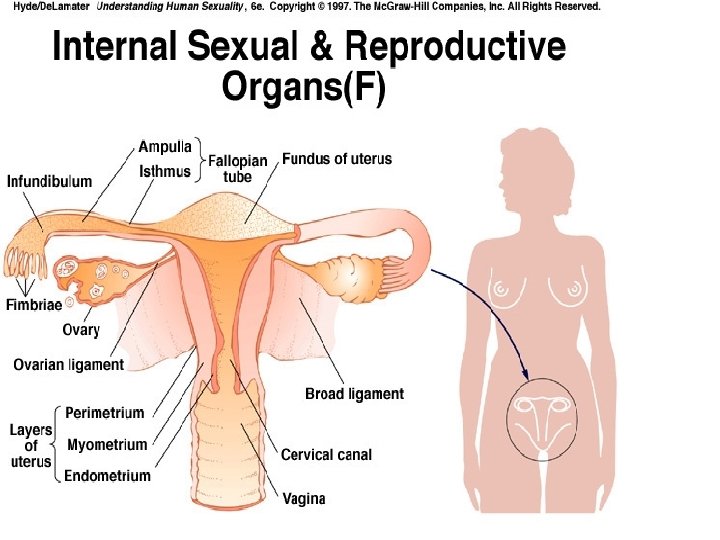
Female Reproductive

Role of Nurses in Women's Health n n n n Personal hygiene Strategies for detecting and preventing disease, especially sexually transmitted diseases (STIs), including human immunodeficiency virus (HIV) infection Issues related to sexuality and sexual function, such as contraception; preconceptional, prenatal, and postnatal care; sexual satisfaction; and menopause Diet, exercise, and other health-promoting practices that maintain and enhance health Avoidance of stressful and abusive situations that are detrimental to health and well-being Maintaining a normal weight for height and avoiding substance abuse and smoking Avoidance of unhealthy lifestyle and risk behaviours

Health History & Clinical Manifestations Menstrual History, Pregnancies, Menses n Sexual History n Female Genital Mutilation n Domestic Violence n Incest and Childhood Sexual Abuse n Rape and Sexual Assault n Health Issues of Women with Disabilities (chart 46 -4) n

Diagnostic Evaluation n Cytologic Test for Cancer- Pap Smear – Bethesda System (chart 46 -7) n Colposcopy and Cervical Biopsy n Cryotherapy and Laser Therapy n Cone Biopsy and LEEP n Endometrial (Aspiration) Biopsy n Dilatation and Curettage n Endoscopic Examinations n Other

Management of Normal and Altered Female Physiologic Processes n Menstruation n Perimenopause n Menopause n Premenstrual Syndrome n Dysmenorrhea n Abnormal Uterine Bleeding

Perimenopause Period extending from the first signs of menopause—usually hot flashes, vaginal dryness, and irregular menses—to beyond the complete cessation of menses

Health Promotion & Disease Prevention Consider the following: n Sexuality, fertility, contraception, STIs n Unintended pregnancy n Oral contraceptive use. n Breast health.

Menopause n Cessation of menstruation n Menopause is perceived as a normal part of the life cycle n Consider Surgical Menopause

Clinical Manifestations Irregular menses, breast tenderness, and mood changes – perimenopause n Hot or warm flashes and night sweats n – profuse sweating, causing discomfort, sleep disturbances and subsequent fatigue, and embarrassment Atrophic changes and osteoporosis Genitourinary system affected by estrogen Vulvovaginal area changes Fatigue, dizziness, forgetfulness, weight gain, irritability, trouble sleeping, feeling “blue, ” and feelings of panic n Psychological considerations n n

Clinical Manifestations Menopause

Menopause Medical management: n Hormone Replacement-estrogen plus progesterone – Advantages & Disadvantages of HRT- women must be informed to make a decision Advantages: decrease CVA, osteoporosis, Alzheimer’s Dx Disadvantages: research has demonstrated that HRT with pre-existing & unknown estrogensensitive breast tumors can accelerate growth & endometrial cancer – Methods of administration
 – Transdermal estrogen patch –")
HRT Types HRT: – Tablet (Estradiol, Estriol & Esterone) – Transdermal estrogen patch – Gel – Vaginal estrogen (for urogenital manifestation) – Vaginal cream-bedtime, several times/week

Menopause Natural Remedies: n Vit E n Calcium n Exercise n Diet n Relaxation n Guided Imagery n Annual screening

Menopause Education self-care : n n n Relief vaginal dryness- use water-soluble lubricants Sexual activity Prevent osteoporosis- wt bearing exercises, Ca, stop smoking, reduce alcohol & caffeine Prevent UTI’s- increase fluid intake, void 23 hours, good personal hygiene, cotton underwear Pelvic relaxation- Kegel excercises, lose weight & excercises to increase muscle tone.
 • • • A combination of emotional & physical manifestations that")
Premenstrual Syndrome (PMS) • • • A combination of emotional & physical manifestations that occur cyclically A somatic (physical syndrome) not psychic Involves endocrine & autonomic & CNS Manifestations peak women 30 -40 yrs. 2 -5% women experience PMS

PMS Etiology Unknown-serotonin regulation is currently the most plausible theory • May be related to hormonal changes combined with other factors n • Diet • Stress • Lack of exercise • A complex of symptoms that result in dysfunction

PMS: Clinical Manifestations Symptoms begin in 5 days preceding menses, relief within 4 days of onset of menses. (chart 46 -10) n n n n n Fluid retention (eg, bloating, breast tenderness) Headache Swelling Depression Anger Irritability Anxiety Confusion Withdrawal Dysfunction usually occurs in relationships, parenting, work, or school.

PMS Management n n n n Use of social support and family resources Nutritious diet - whole grains, fruits, vegetables; increased water intake may help. Serotonin reuptake inhibitors (fluoxetine) alprazolam (Xanax) has been effective but is addictive. spironolactone may be effective in treating fluid retention. Initiation/maintenance of exercise program. Stress reduction techniques.

PMS Nursing Management n n n n Acknowledge PMS Nursing assessment lifestyle, sleep, nutrition & health maintenance Provide education re: syndrome & reassure about physiologic basis for manifestations Encourage lifestyle modifications-reduce Na & refined CHO, small freq. meals (stabilize glucose to decrease fatigue, craving, irritability), Ca intake 1000 mg/day, reduce alcohol, caffeine, smoking cessation, weight reduction, exercise Improve coping: support groups, educational sessions Education re medications Psychosocial assessment
- Slides: 129