Human Immunodeficiency Virus HIV and the correctional system

 problem for the correctional services but also")

")





 Drug abuse - HIV - Crime - Imprisonment")

")



")





 CCR 5 -antagonist • Maraviroc Integrase inhibitors")


 PI 2 NRTI’s + NNRTI Backbone 3 rd agent HAART")
 PI Kaletra Reyataz 2 NRTI’s + NNRTI Truvada Kivexa (Combivir)")
 Selection of resistant")



 The")




- Slides: 40
Human Immunodeficiency Virus – HIV and the correctional system
Prison inmates with HIV Medical (and practical) problem for the correctional services but also An marvellous opportunity for the individual and for society!
Swedish Prison and Probation Authorities 1987 Fight HIV and AIDS by prevention • • Information and education Discussions about route of transmission Testing Contact tracing and drug rehabilitation (and since 1996 ART treatment run by the civil health care)
The over all goal (at least from the inf dis epidemiologist point of view) • …is to reduce the risk for further transmission from a HIV positive individual to another inside the prison and later, after release, in the society. • …is to educate the ones who are still healthy to live their life in such a way that their risk of contracting the infection themselves is reduced
Harm reduction programmes Harm reduction ”hot potatoes” in Sweden but must be considered • Needle and syringes exchange • Belach distribution • Substitution therapy (Methadone) – opioid IDA
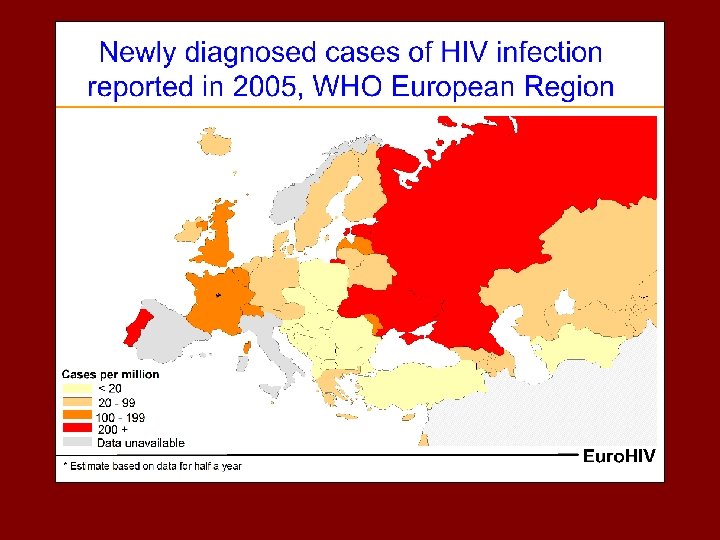
HIV epidemiology
HIV prevalens 2006
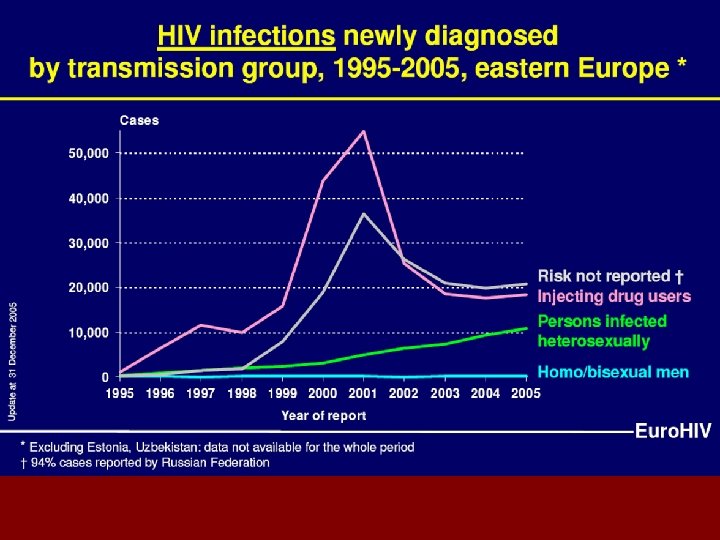
HIV in Europe • Slowly increasing prevalence in Western Europe • Quickly increasing prevalence in Eastern Europe
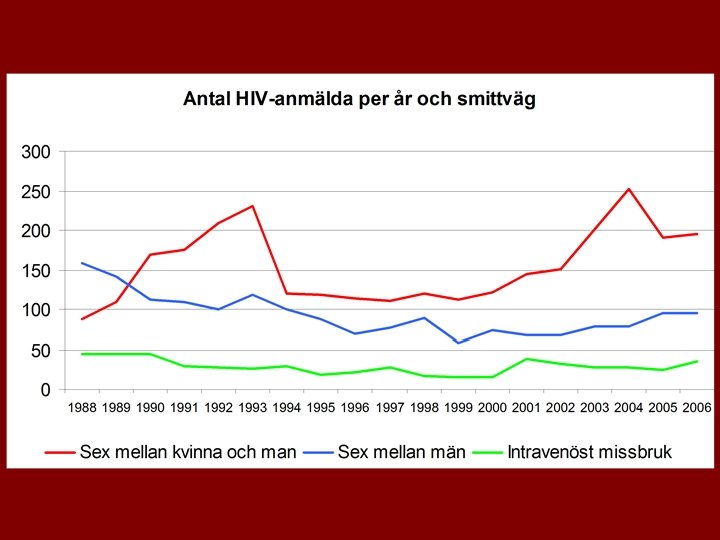
Why so few cases of HIV among iv drug abusers in Sweden? Of cause many reasons but…
(IV) Drug abuse - HIV - Crime - Imprisonment
Swedish Prison and Probation Authorities 1987 Fight HIV and AIDS by prevention • • Information and education Discussions about route of transmission Testing Contact tracing and drug rehabilitation (and since 1996 ART treatment)
The disease (Here symbolized by a dying T-helper cell)
HIV Lifecycle- why is HIV harmful? HIV Enemy CD 4+ cell 5000 new HIV General n HIV infects CD 4+ cells (T-helper cells) n HIV grows quickly inside CD 4+ cells – CD 4+ cells dies n Immunodeficiency developes due to lack of CD 4+ cells
HIV infection - natural history Prim HIV infection CD 4+ cells AIDS HIV nivå Death in AIDS
HIV treatment
Effect of antiviral treatment (ART)
Reported cases of AIDS and related death 1983 -2006 Aids Dead
HIV drugs- 4 different classes NRTI • RT= Reverse Transcriptase (the enzyme that rewrites the virus RNA to DNA form) • NRTI= Nucleoside RT Inhibitor • NRTI is nucleoside analogues (false DNA building blocks) that replases the real nucleosid in the new DNA chain and prevents it´s extension (chain terminator)
HIV drugs- 4 different. PIclasses protease inhibitor NRTI • The protease is the enzyme that splits the new established virus in smaller that can later be put together to a new functional contagious virus • PI bindes to the protease and obstructs it´s function
HIV drugs- 4 different. PIclasses protease inhibitor NRTI NNRTI • NNRTI= non-nucleoside RT inhibitors • Obstructs the same RT enzyme as NRTI but in a different way • NNRTI inhibits RT through binding to the enzyme
HIV drugs- 4 different. PIclasses protease inhibitor FI-Fusions inhibitor NRTI NNRTI • FI prevents HIV to enter the cell by preventing the virus to bind to the cell surface
New HIV drug classes (in the pipe-line) CCR 5 -antagonist • Maraviroc Integrase inhibitors • Raltegravir • Elvitegravir (Mk-0518) (GS 9137)
HIV treatment principles Start of treatment: Not too early - not too late Less long time side effects develope CD 4+ cell count 200 -300 Before symptoms
HIV treatment principles 2 • Only patients with undetectable viral load have a durable effect Undetectable is <40 copies/ml • If virus is not fully suppressed- resistance will always develop Only fully adherent patients reach undetectable viral load
Favored Initial Combinations (HAART) PI 2 NRTI’s + NNRTI Backbone 3 rd agent HAART = Highly Active Anti-Retroviral Treatment (a combination of 3 or more HIV drugs)
Favored Initial Combinations (HAART) PI Kaletra Reyataz 2 NRTI’s + NNRTI Truvada Kivexa (Combivir) Stocrin
Why resistance? Detectable viral levels during treatment (HIVRNA >50 kop/m. L) Selection of resistant virus Incomplete viral suppression always leads to development of resistance !!
What are the major causes of Treatment Failure ? – Suboptimal adherence – ARV toxicity and intolerance – Pharmacokinetic problems – Suboptimal drug potency / viral resistance
Resistance test: • NRTI- 8 mut • NNRTI-1 mut • PI- 13 mut
Conclusion! • Treatment and follow up of treatment of HIV is complex • Viral levels, CD 4 cells, combination possibilities, side effects, resistance…. • And if it isn´t conducted properly one might harm the patient – resistance. And remember. Treatment must be followed up carefully also after the patient leaves the prison! Can an active IVDA fix that? • Co-op with specialist in HIV treatment (that is now a ”specialty of it´s own”) and rehab drug abuse
Conclusion Co-operation between experts and authorities The hospital And the doctor (me? ) The HIV patient and the prison system Communicable Disease Control Other org and authorities
HIV – risk of transmission • Blood transfusion • Pregnancy mother/child ~100 % 15 -35 % • Iv drug abuse - sharing syringes 1 -10 % ? • Coitus (vaginal intercource) • Anal intercource <1% <3% Needle-stick incidents at hospitals Mucosal exposure at hospitals 0. 3 % 0. 09 %
HIV – risk of transmission
Conclusion • Complex situation! • Opportunity! • Only treat the treatable! • Combine with treatment of drug dependancy • Beware of the resistance!
Thank You!