Human Fascioliasis By Prof Dr Ayman El Shayeb

Human Fascioliasis By: Prof. Dr. Ayman El Shayeb Professor of Tropical medicine Alexandria Faculty of Medicine

Introduction For years, fascioliasis was considered as an uncommon zoonotic disease distributed worldwide, caused by the liver flukes Fasciola Hepatica and Giganticawhere several geographical areas have been described as endemic for the disease, which is now recognized as an emerging zoonosis by the WHO, and an important human parasitic disease. l In recent years, the epidemiological picture of human fascioliasis has changed In Egypt, human fascioliasis is increasingly recognized as an important public health problem. During the last few years, many Egyptians, especially children, where diagnosed as having fascioliasis.

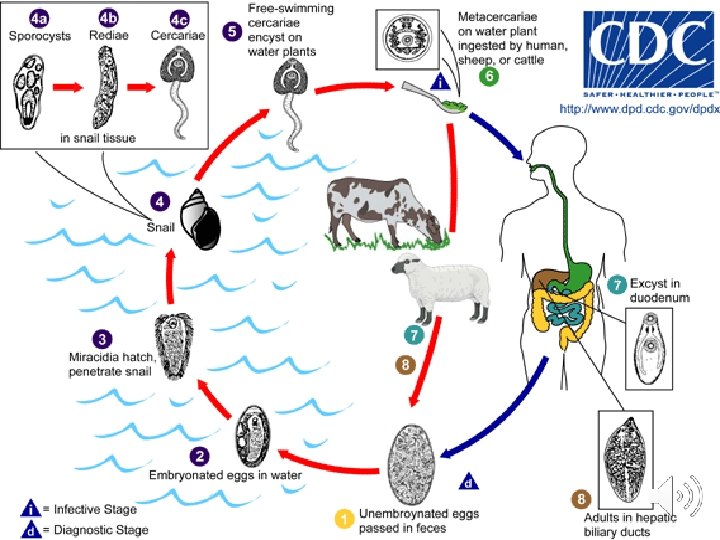

Mode of infection and life cycle Man gets infection by ingestion of raw aquatic plants or water contaminated with metacercariae. Infection might also be acquired from contaminated cooking utensils. l The metacercariae excyst in the duodenum, penetrate the intestinal walls into the body cavity, then penetrate the liver tissue where they maturate and become adult hermaphrodite flukes which live in the bile ducts and start to lay eggs 3 -4 months after ingestion of metacercariae. l

Clinical Presentations: • Acute stage: the migration of the F. hepatica larvae throughout the liver parenchyma. The larvae penetrate the liver capsule and begin to produce the symptoms 4 -7 days after ingestion. Migration and thus the acute phase continues for 6 -8 weeks until the larvae mature and settle in the bile ducts. • tender hepatomegaly, fever, upper right abdominal pain • ± splenomegaly, urticaria, cough, dyspepsia, anorexia, vomiting, diarrhoea, weight loss, jaundice, headache, hemobilia This stage is characterized by high eosinophilia up to 80%.

Chronic stage: These symptoms reflect the biliary obstruction and inflammation caused by the presence of the large adult worms and their metabolic waste in the bile ducts. . This stage presents by: cholangitis, cholestatic jaundice, nausea, vomiting, fatty food intolerance l upper right abdominal pain with hepatomegaly, pruritis, anemia and fever. l

Abnormal presentations: The patients may present with uncommon forms such as multi-organ infections, PUO, splenomegaly, upper GIT hemorrhage, hemorrhagic ascites, and even severe life threatening form of recurrent subcapsular hepatic hematomas. Ectopic fascioliasis: including eosinophilic panniculitis, pulmonary infiltrates, pleuropericarditis, meningitis & lymphadenopathy.

Halzoun: Is a type of Fasciola hepatica infection in which the worm settles in the pharynx. This occurs when an individual consumes infected raw liver. The young adult worms then attach themselves to the laryngeal-pharyngeal mucosa which causes considerable pain, edema, and bleeding that can interfere with respiration.

Diagnosis of fascioliasis: For diagnosing fascioliasis, you should focus on the following points: 1. History: e. g. from endemic areas, risky occupation and eating fresh vegetables. 2. Clinical presentation. 3. D. D. (Schistosomiasis, other liver flukes, VLM, viral hepatitis and other causes of cholangitis and gall stones). 4. Spurious infection: this false fascioliasis refers to the presence of eggs in the stool resulting not from actual infection but from ingestion of infected liver containing eggs. This situation can be avoided by having the patients follow a liver-free diet several days before the stool examination. 5. Eggs can be found in stool, duodenal content and bile as well as histological sections (useful in the chronic stage). 6. Eosinophilia: it is the most important laboratory abnormality in fascioliasis (40 -80% in acute stage and continues into the chronic stage). 7. Leucocytosis and anemia.

8. 9. Liver function tests: denoting cholestasis. Immunodiagnosis: the flukes do not begin to produce eggs until roughly 4 months after infection. Until this time and in the case of ectopic infections where eggs are not present in the stool, serological tests can be used, . A variety of available techniques include: skin test, IHAT, ELISA, IF, CIE, gel electrophoresis and metacercariae precipitin test. 10. Radiological imaging: US, CT, MRI, ERCP, percutaneous cholangiography and even laparotomy and liver biopsy may also be useful. These allow visualization of the lesion of acute and especially chronic fascioliasis and sometimes eggs or worms in the hepatobiliary system as well as histopathological lesions.

Treatment of fascioliasis 1. Medical therapy: l. Triclabendazole the drug of choice in treating fascioliasis. It is often effective at an oral dose of 10 mg/kg/day taken with or after meals, as single or better double doses on 2 consecutive days, or even for multiple doses in persistent infection. No serious side effects were noted. l. Praziquantel l. Bithionol Recently, preliminary results on a new drug, Myrrh were proved to be encouraging especially because of its double efficacy on both fascioliasis and schistosomiasis with no obvious side effects. l

2. ERCP: cases with obstructive jaundice can be treated by ERCP and sphincterotomy with worm extraction followed by fasciolicidal drugs. 3. Surgical therapy: Some cases with obstructive jaundice need surgical therapy where cholecystectomy is performed.

Prevention and control of fascioliasis Strategic control of fascioliasis must focus on: 1. Treatment and, if available, vaccination of animals which maintain the life cycle (sheep and cattle). 2. Control of snail vectors using molluscicides. 3. Health education. 4. Increased clinicians’ awareness of the problem, it diagnostic, therapeutic and prevention difficulties. As regard health education, it is important to know that, to prevent human fascioliasis we should clean the leafy salads from metacercariae (infective stage of fasciola). This could be achieved by either: -Citric acid in a concentration of 10 ml/ L -Commercial vinegar (120 ml/ L) -Liquid soap (12 ml/ L) -Potassium permanganate (24 mg/ L) All the above detach all metacercariae after 10 minutes exposure.

- Slides: 15