Hulsi Behet 1889 1948 Main Distribution Silk Root
")
Hulûsi Behçet (1889 -1948)

Main Distribution: Silk Root Male/Female Ratio • Variable • Near the same in large series Mean Age: 25 - 30 Genetic Origin: Turkic Tribe

Silk Road

Prevalence/100, 0 00 Portugal 1. 5 Japan 13. 4 Turkey 80 -370 Spain 7. 5 Iran 16. 7 Egypt 7. 6 Saudi Arabia 20 Kuwait 1. 2 China 14

Pathogenesis · Unknown · Genetic predisposition · Infection / environmental pollution · Immunological reaction · Damage of vascular endothelium

HLA-B 51 -associated Relative Risk for the occurrence of Behçet’s disease 1 5 3 63 5 73 43 11 9 2 5 10129 4 20 9 9 1 4 8 9
 w Viruse (HSV) w Chemicals (heavy metals)")
Triggering Agents w Bacteria (Strep. oralis (sanguis) w Viruse (HSV) w Chemicals (heavy metals)

Genetic predisposition w HLA-B 51
 dominates the flora of the oral mucosa in")
Bacterial infection · Strep. oralis (sanguis) dominates the flora of the oral mucosa in patients with the disease. · A chronic infection with Ig. A proteaseproducing Strep. sanguis species is suggested.

Viral infection · Partial transcription of the HSV-I genome in patients´ peripheral blood mononuclear cells. · Identification of a 211 -bp HSV-I DNA fragment in patients´ peripheral blood cells. · HSV-I DNA was detected in 43% of 91 saliva patients´ samples compared to 14% of 87 samples from healthy controls (p<0. 01).

Immunological parameters · Strep. sanguis hsp-60 and -65 induce proliferation of gd+CD 8+ T-cells. · MICA protein is recognised by T-cells with a variable Vd 1 gd region in their Tcell receptor. · Antigens are presented to gd+CD 8+ Tcells assisted by the MICA molecule.

Behçet’s disease: a systemic disorder Skin involvement (Folliculitis/pustules, erythema nodosum, pyoderma, necrotising ulcers, superficial thrombophlebitis, pathergy reaction) Cerebral manifestations Uveitis (sterile meningoencephalitis, (Hypopyon-Iritis, Retinitis) vasa neurorum) Oral aphthous ulcers Cardiac involvement (Pericarditis, endocarditis) Lung involvement (Aneurysma, embolic lesions, haemorrhagy) Arterial aneurysma (Vasa vasorum) Kidney involvement Phlebothrombosis (Vasculitis) Gastrointestinal involvement Genital ulcers Prostatitis (Gastritis, ulcers, Pseudo-Crohn) Arthritis
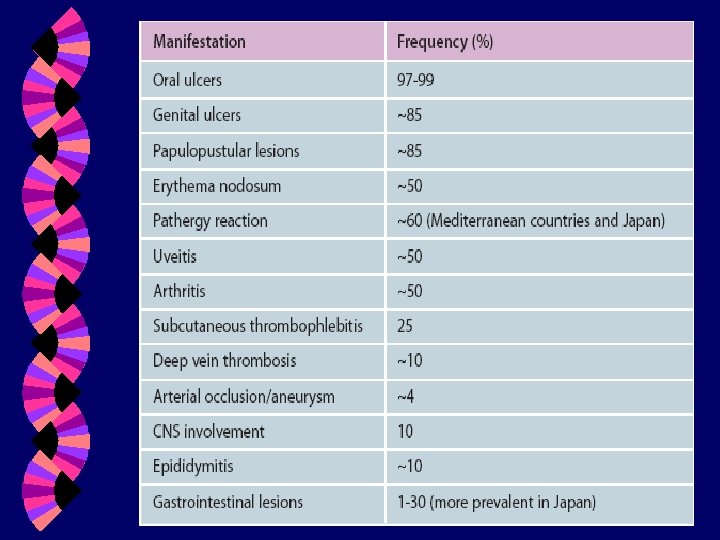

Clinical presentation A common clinical feature in patients is painful, recurrent muco-cutaneous ulcers. Oral ulcers: Size ranges from a few mm to 2 cm. Grossly and histologically similar to common oral ulcers. Multiple. Often heal spontaneously in 1 -3 weeks.

Genital ulcers w Occur in 75% of patients. w Appear similar to oral ulcers. w Most frequently scrotal in men, vulvular in women. w Epididymitis, salpingitis, urethritis

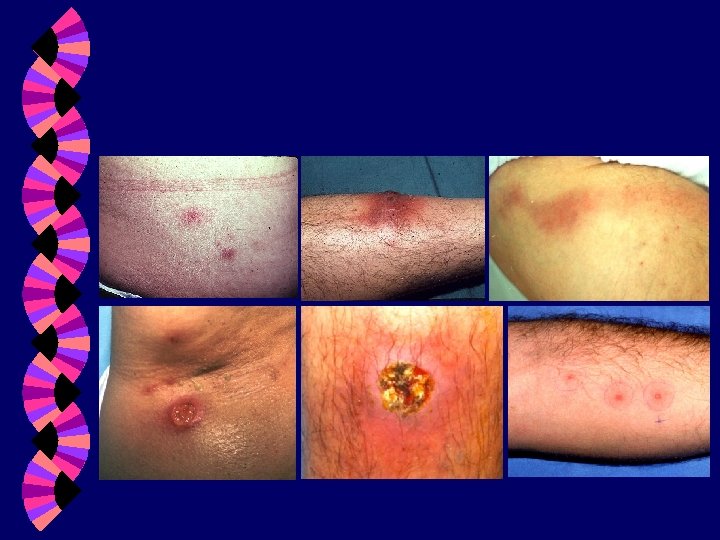
Cutaneous lesions Acneiform lesions, nodules, erythema nodosum, superficial thrombophlebitis, palpable purpura, pyoderma-gangrenosum.

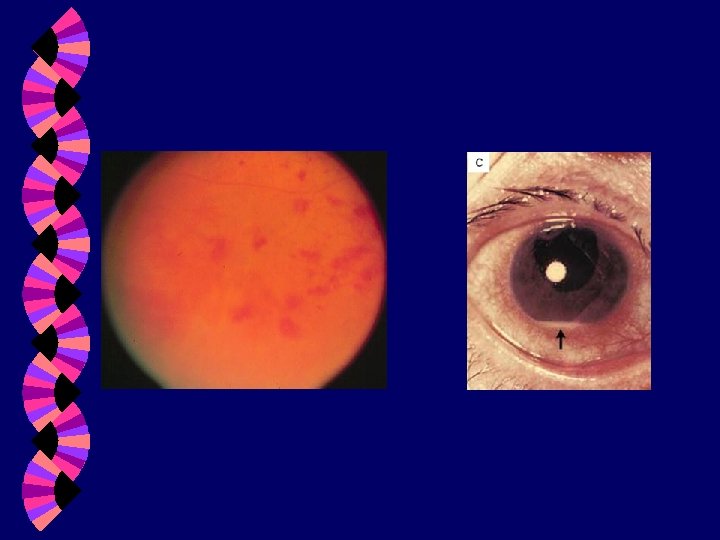
Ocular disease Ø Uveitis is bilateral or unilateral, episodic sometimes with no resolution between episodes. Ø Hypopyon: purulent material present in anterior chamber indicating severe anterior uveitis. Ø Posterior uveitis, retinal vasculitis, vascular occlusion, optic neuritis: may progress to blindness if untreated. May require immunosuppressive treatment. Ø Glaucoma, cataracts can occur.

Neurological disease More common in males w Occurs in less than 20% of patients w Commonest abnormalities are vascular thrombosis and focal parenchymal lesions. w Manifestations include: progressive personality change, psychiatric disorders, dementia, aseptic meningitis, encephalitis. Peripheral neuropathy is not common. w Arteritis can lead to dissection, aneurysmal dilatation and subarachnoid hemorrhage. w

Vascular disease w Venous involvement occurs more commonly than arterial. w Superficial and deep venous thrombosis is common. w Many patients have small vessel vasculitis. w 30% have large vessel involvement, including stenosis and aneurysms. w Pulmonary arterial involvement is characteristic.

Arthritis w w Arthritis is nonerosive, inflammatory oligoarthritis w Occurs in 50% of patients w Asymmetric and usually does not result in deformities. w Commonly affects medium/large joints. w Occurs particularly during exacerbations, lasts 1 -3 wks.

Diagnostic criteria Recurrent oral ulcers at least 3 times in a year w Recurrent genital ulcers w Eye inflammation w Skin inflammation w • Pseudo folliculitis • Acne-like lesions • Erythema nodosum-like w Positive Pathergy test

DIFFFERENTIAL • Reiter's syndrome and other forms of spondyloarthropathy • Inflammatory bowel disease (Crohn's disease and ulcerative colitis) • Syphilis • Erythema nodosum • Aphthous stomatitis

DIFFFERENTIAL • • • Herpes simplex Stevens-Johnson syndrome Vasculitis Multisystem disease Thrombophlebitis related to coagulation factor deficiency

Prognosis and clinical course w Variable with exacerbations and remissions. Typical presentation is initially with mucocutaneous lesions and subsequently ocular and neurological disease occurring years after diagnosis. w Mortality is low and is usually related to pulmonary or CNS hemorrhage or bowel perforation. w Most common cause of morbidity is ocular disease which can result in blindness if untreated.

Treatment w Is based on degree of involvement and individual presentation. w Studies of treatment protocols are small. Agents used- mucocutaneous disease w Topical steroids w Colchicine w Dapsone w

Severe mucocutaneous disease Methotrexate Prednisone Interferon Alpha Thalidomide Systemic disease Prednisone Azathrioprine Cyclophosphamide Anti-TNF drugs

Complications • • Death Blindness Paralysis Embolism/thrombosis - pulmonary, vena cava, peripheral • Aneurysms • Amyloidosis • Thrombotic events, especially when anticardiolipin antibodies present

• Normal life expectancy, except with neurologic involvement • Possible vision impairment • Avoid English Walnuts!!
- Slides: 30