https www ccdhb org nzworkingwithusnursingandmidwiferyworkforcedevelopmentclinicallearningenvironmentisbar 2014 pdf ISBAR


https: //www. ccdhb. org. nz/working-with-us/nursing-and-midwifery-workforce-development/clinical-learning-environment/isbar 2014. pdf

ISBAR I S B A Introduction Situation Background Assessmen/ Awareness R Recommendation Identify -I am What’s going on Brief, relevant history What I think is happening Request/Recommend -What you are asking them to do

ISBAR format ใชไดใน ทก รปแบบ : Clinical Handover communication Referrals Protocols, memos and emails Reports (Ward etc) Personal interactions


Surveillance

Early Warning System




Detection


Early Treatment


PPH • Trigger points แบงเปน 4 grade q first trigger point at 500 m. L, followed by 1000 m. L, 1500 m. L and over 2000 m. L • Response algorithms ทสำคญของแตละขนตอน คอ “effective communication and collaboration”

Trigger - Vital Signs Clinical triggers : HR, BP, oxygen saturation, etc.


Scores • The National Health System of the United Kingdom ทำ “Obstetric Early Warning Chart” ทำ checklist ทเปนส ของ vital status (ใชทงตวเลขและรองรอยทเหน ) และ guide เรอง intervention • บนทก “triggers” ณเวลาใดเวลาหนง ลงใหตรงแถบส “in one red or two yellow scores ”(See Best Practice article “Blood Loss: Clinical Techniques for Ongoing Quantitative Measurement”)

complete, clear, brief และทนเวลา ) อาจใชเทคนก ISBAR")
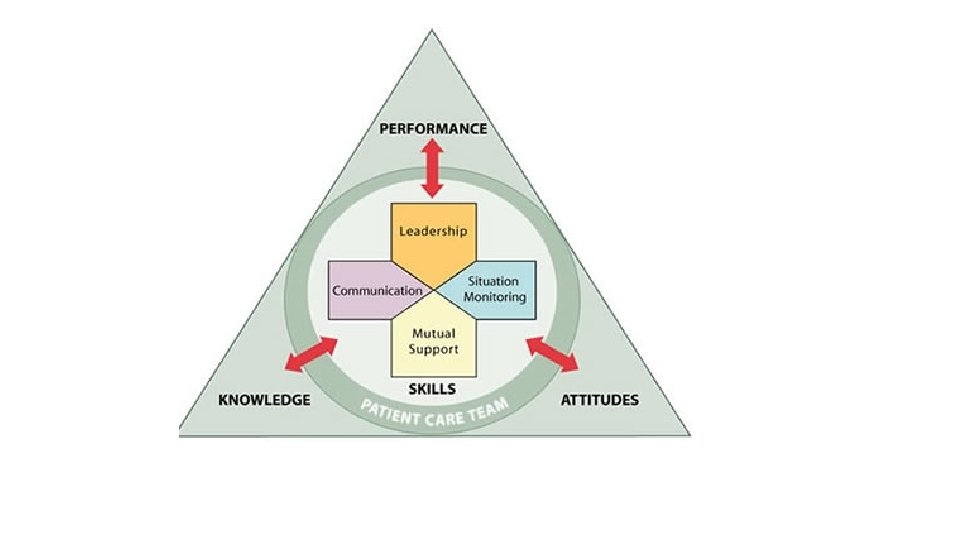
• Team. STEPPS โดยนยามตองม effective communication )complete, clear, brief และทนเวลา ) อาจใชเทคนก ISBAR เพอใชสอสารขอมลวกฤตเกยวกบ condition คนไข จำเปนตองใหความสนใจและลงมอทำทนท : Introduction, Identify: I am …………. Situation: What’s going on with the patient? Background: What is the clinical background or context? Assessment: What do you think the problem is? • Recommendation and Request: What would you do to correct the problem?
")
Maternal Early Obstetrics Warning Signs • MEOWS /MEWS • maternal early warning criteria (MERC)
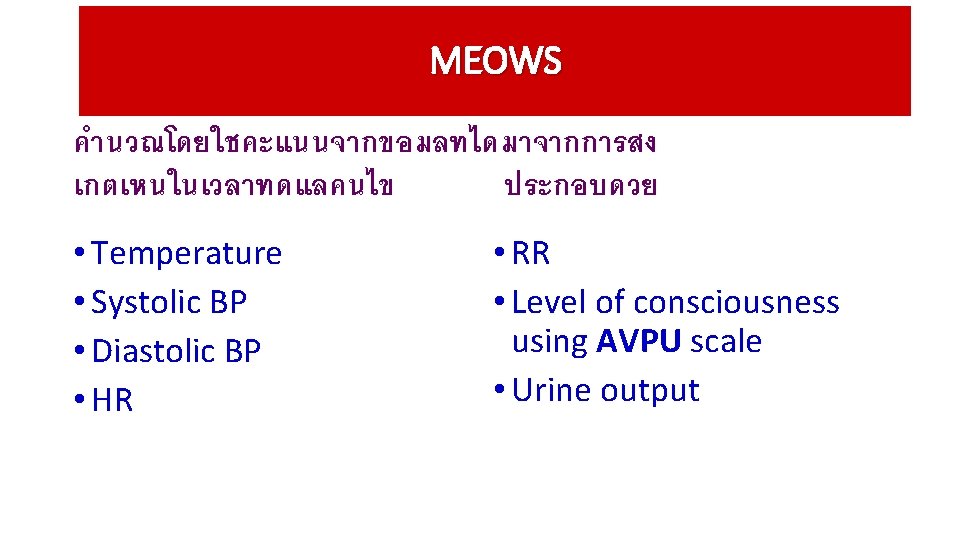

AVPU scale A - Alert and conscious V-Voice P-Pain U-Unresponsive Response to voice Response to pain No response to voice or pain

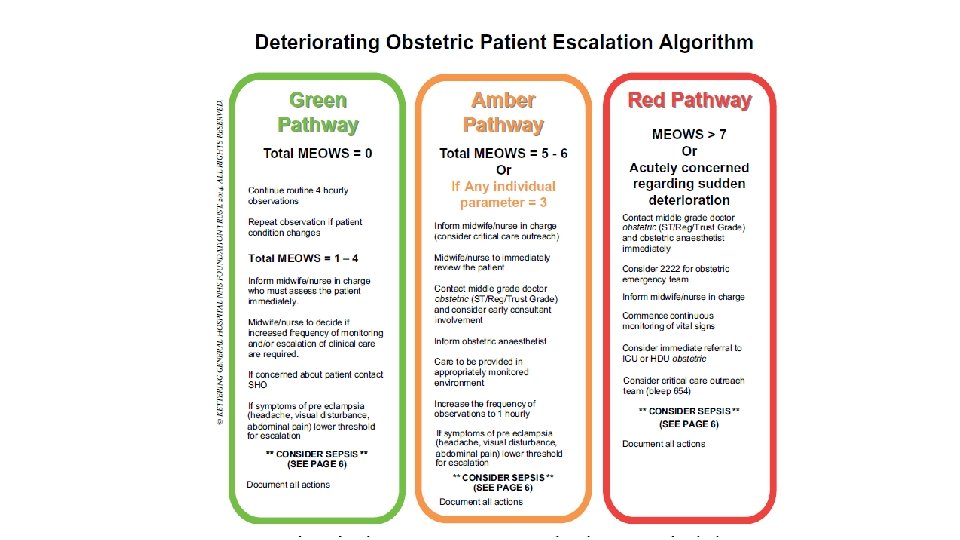
MEWS SCORES Physiological parameters Normal values Yellow alert RR 10 -20 21 -30 Oxygen sat. 96 -100 T 36. 0 -37. 4 C 35 -36 or 37. 5 -38 C SBP 100 -139 150 -180 or 90 -100 DBP 50 -89 90 -100 HR 50 -99 100 -120 or 40 -50 Neurological response Alert Voice Red Alert <10 or >30 <95 <35 or >38 C >180 or <90 >100 >120 or <40 Unresponsive pain

Score 3 T SBP < 69 3 3 0 1 2 3 < 35 C 35 -35. 9 C 36 -37. 4 C 37. 5 -37. 9 C 38. 0 -38. 9 >39 C 70 -79 80 -89 90 -139 140 -149 150 -159 >160 <49 50 -89 90 -99 100 -109 >110 40 -49 50 -99 100 -109 110 -129 >130 11 -19 20 -24 25 -29 >30 Alert Response to voice Response to pain Unconscious DBP <40 P R < 10 AVPU Urine output/hr <30 < 10 Not measure

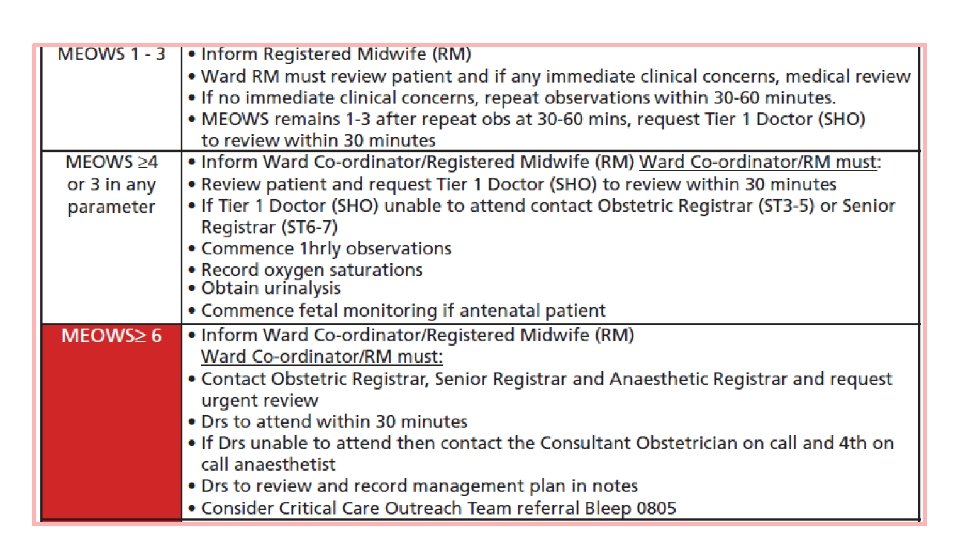
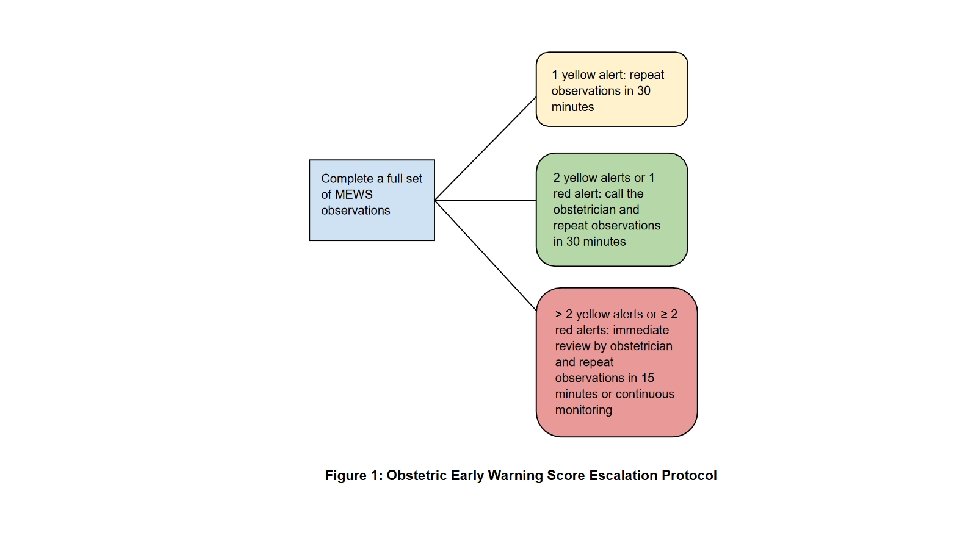
MEOWS SCORES Scores frequency of observations 1 1 -3 >4 or 3 in any parameter + ++/or a medical review Initiate call out cascade ผท triggers ดวยคะแนน ≥ 4, or 3 ใน parameter ใดๆ ควรให oxygen รวมกบทำ full set of observations

Surveillance of PPH

PPH Prevention Causes Treatments Dx & Its Severity Integration

Risks • Before • During

Significant risk factors • Retained placenta (OR 3. 5, 95% CI 2. 1 -5. 8) • Failure to progress during the second stage of labor (OR 3. 4, 95% CI 2. 4 -4. 7) • Placenta accreta (OR 3. 3, 95% CI 1. 7 -6. 4) • Lacerations (OR 2. 4, 95% CI 2. 0 -2. 8) • Instrumental delivery (OR 2. 3, 95% CI 1. 6 -3. 4) • Large-for-gestational-age (LGA) newborn (OR 1. 9, 95% CI 1. 6 -2. 4) • Hypertensive disorders (OR 1. 7, 95%CI 1. 2 -2. 1) • Induction of labor (OR 1. 4, 95%CI 1. 1 -1. 7) • Augmentation of labor with oxytocin (OR 1. 4, 95% CI 1. 2 -1. 7)

BMI >40, the risk: • Normal delivery 5. 2% • Instrumental 3. 6%

ACOG




 Symptoms and Signs Degree")
Clinical Findings in Obstetric Hemorrhage Blood Volume Loss BP (systolic) Symptoms and Signs Degree of Shock 500 -1000 m. L (10 -15%) Normal Palpitations, tachycardia, dizziness Compensated 1000 -1500 m. L (15 -25%) Slight fall (80 -100 mm Hg) 1500 -2000 m. L (25 -35%) Moderate fali (70 -80 mm Hg) Restlessness, pallor, oliguria Moderate 2000 -3000 m. L (35 -50%) Marked fall 50 -70 mm Hg) Collapse, air hunger, anuria Severe Weakness, tachycardia, sweating Mild

Class-SHOCK 3 2 1 blood loss Pulse BP Conscious 750 -1, 500 m. L loss 15 -30% blood loss Pulse 100 -120/min BP ���� Orthostatic) 4 >2000 ml/>1 bl vol > 40% blood loss Pulse >140/min BP ������ Coagulopathy • ตนทนเดม • ปรมาณเลอดทเสยเพ ม



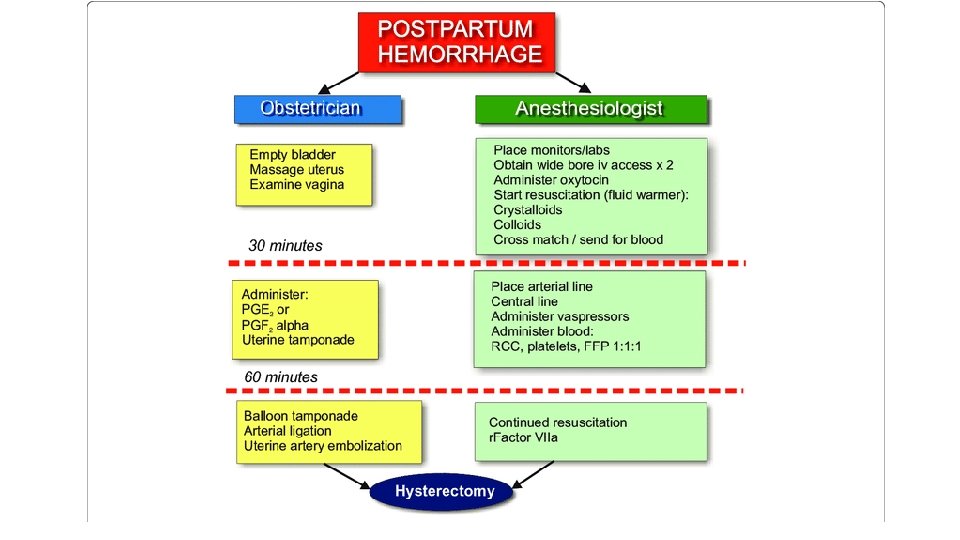
First Second Medication
 • ม")
Organization of care • ใช formal protocol สำหรบปองกน (Weak, minimal quality evidence) • ม formal protocol ในเรองการ (week, very low quality evidence) และรกษา refer จากชมชน • ทำ simulation ระดบชมชน (week, very low quality evidence) • Monitor การใช uterotonics เพอการปองกน process indicator evaluation (week, very low quality evidence) เปน

Hemodynamic คงท Try conservative ไมคงท Surgery

trigger responses

Criteria for near-miss study of hemorrhage
- Slides: 74