How to Perform a Successful Transseptal Puncture Zoltan




































- Slides: 41
How to Perform a Successful Transseptal Puncture Zoltan G Turi MD, MSCAI, FACC Seton Hall University School of Medicine Hackensack University Medical Center
Disclosure Zoltan Turi MD, MSCAI Clinical Events Committee - Mitralign Research Support - Abbott Vascular Training Grant Support - Abbott Vascular, Medtronic
Alkhouli JACC CI 2016 De. Ponti JACC 2006
1958 - 1979
B A A B
Puncture? No
G. Joseph CCVD 42: 138, 1997
G. Joseph CCVD 42: 138, 1997
AP
2 cm 20 degree RAO
Puncture? No
90 o lateral
90 degree lateral
Cheng J Cardiovasc Electrophys 6 2007
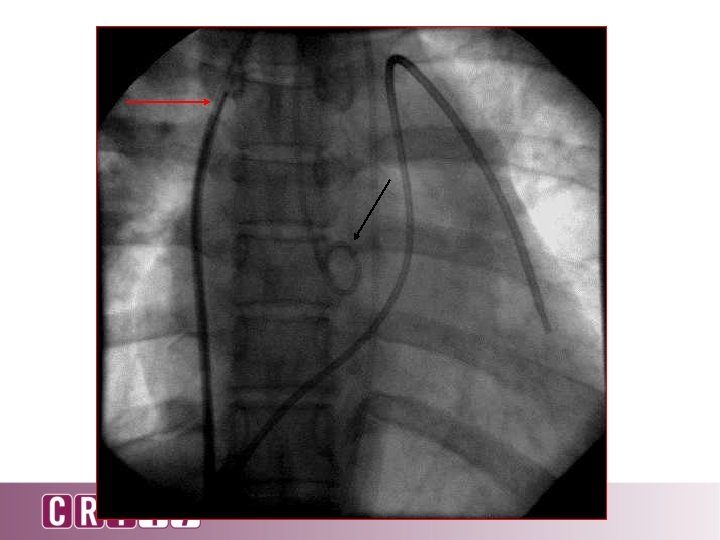
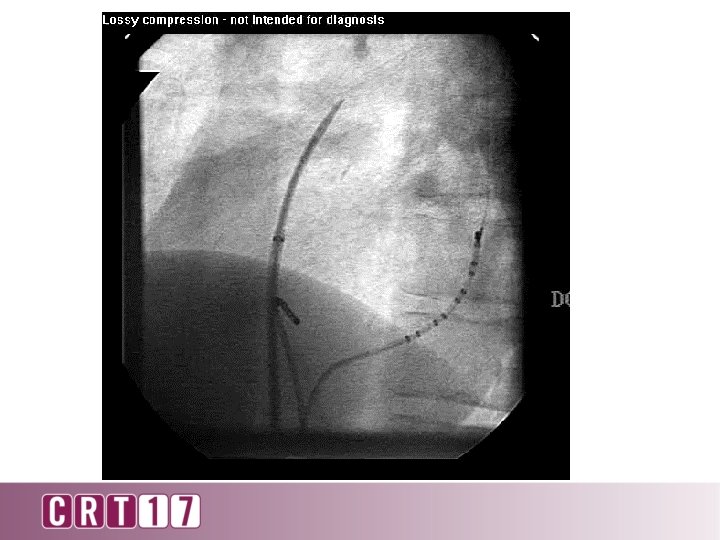
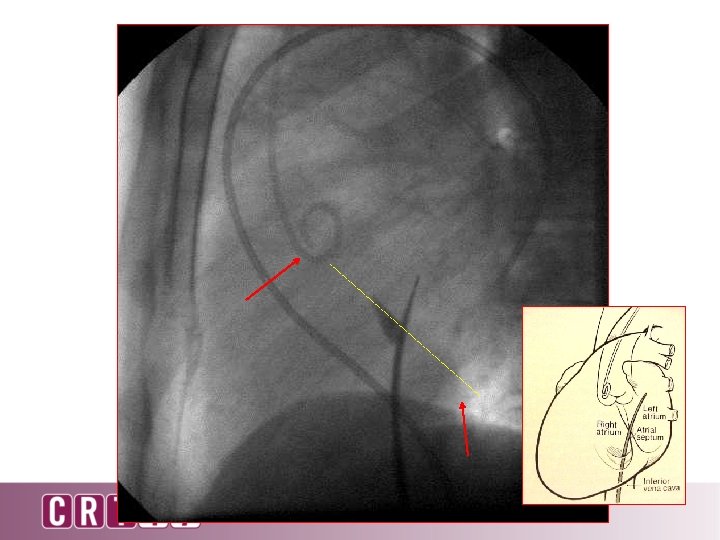
STOP – Check needle pressure – Check oxygen saturation – Inject dye
LA RA
Alternate Methods • Right atrial angiogram • Levophase LA gram • Aortic root angiography Superior atrial boundary Gauri Indian Pacing Electrophysiology J 2003 Aortic root Posterior atrial boundary Left ventricle 1 -3 cm x Inferior atrial boundary Plane of mitral valve Inoue technique (40° right anterior oblique projection) Faletra JASE 2011
Atlas of Percutaneous Mitral Valve Repair
Puncture high and posterior Puncture low and posterior
Singh GD, Intervent Cardiol Clin 2016 Alkhouli JACC CI 2016
Other Approaches to the Left Atrium • • Transhepatic Transjugular Subclavian Retrograde Singh SM Circ Arrhythmia Electrophys 2011
Complications • Tamponade 0. 5 -4 % • Embolic events: air/clot • • – Ischemia, MI, TIA/stroke ~ 1% Mortality 0. 1 – 1. 4 % Arrhythmias Vagal stimulation Transient ST elevation
Clot • Flush needle frequently • Be ready to proceed as soon as needle and sheath are introduced • Anticoagulate as soon as secure access to left atrium is obtained and patient is stable Kim JS Circ Arrhythmia Electrophys 2013 Alkhouli JACC CI 2016
Factors Influencing Complication Rates • Diagnostic versus interventional – Diagnostic – 1. 3% (Roelke CCD 1994) – Interventions - 3. 8% (Liu AHJ 2006) • • • Level of anticoagulation Sheath size Left atrial pressure Presence and compliance of pericardium Use of echo guidance Most important – Operator learning curve
Be on the Hemodynamic Alert • Bradycardia • Hypotension – But can have hypertension and tachycardia • Call for echo but don’t wait – Check fluoro for straightening and immobility of left heart border
Errant Punctures • Free wall – right and left atrium • Pulmonary vein hemothorax • Aorta – sometimes benign • Stitch perforation RA LA
Predisposing Factors to Bad Sticks • • Severe kyphoscoliosis Giant left atrium Prominent Eustachian Valve Anatomic variations Eustachian valve
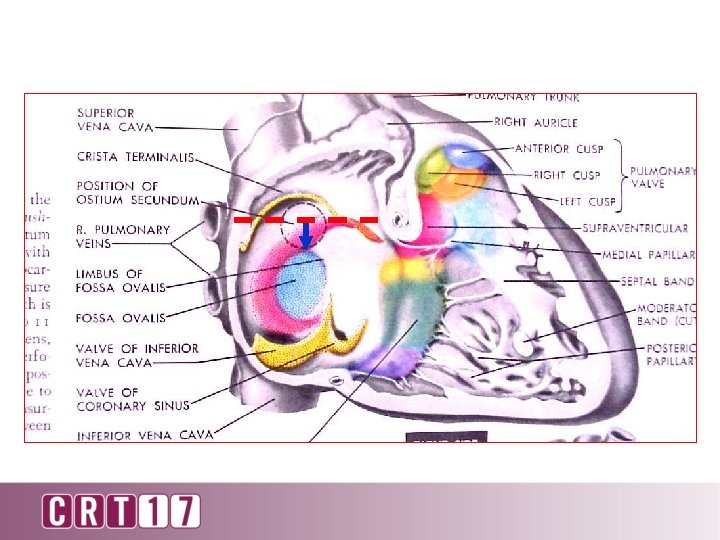
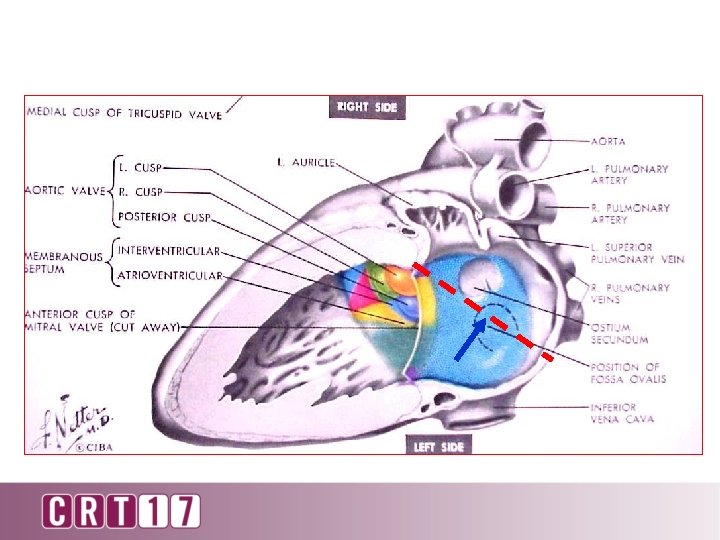
Not All Fossa Are The Same Bulging May not be where you expect it to be
“Controlled perforation”. 014 wire stylet Thick, fibrotic, aneurysmal septum Bidart Heart Rhythm 2008 Winkle Heart Rhythm 2011 RF vs Standard N 575 vs 975 Failure to cross 0. 17 vs 1. 23% Tamponade 0 vs 0. 92 %
Conclusions: Negative LA pressures in conjunction with air-leaking sheaths are identified as potentially important factors for air intrusion into the LA. Catheterization and Cardiovascular Interventions 71: 553– 558 (2008)
Complications of Transseptal Access: Air Embolism Courtesy Dr. Kalyanam Shivkumar
How Do You Become Competent De. Ponti JACC 2011
Go Where Diseases Requiring Transseptal are Prevalent
Stay Sharp