How to establish diagnosis 692 421 Diagnosis and

How to establish diagnosis 692 -421 Diagnosis and treatment plan for comprehensive clinic Lecture room no. 4 Dr. Kanokporn Pangsomboon 15/10/2557

Past & Current Systemic Medical Conditions : ���������������� Family history : No Psychosocial history & Environmental factor : ����������������

Oral and maxillofacial history Head/Face/Jaw/Teeth Trauma : No Orofacial Pain : No Recurrent oral ulceration : No Discomfort in the mouth : No Head/Face/Neck Radiotherapy : No

• Previous dental check up/treatment : When have a problem • Previous treatment : Operative Tx. , Periodontal Tx. , Endodontic Tx. , Prosthodontic Tx. , Oral and /maxillofacial Surg. U/- TP with wrought wire 24 (short extend)

Behavioral history Personal history Smoking : No Smokeless tobacco : No Betel quid : No Drinking : No

Dietary behaviour ������� 3 ������ Favourite taste: ������ Favourite food consistency: normal ������� 1 �������������� 1

Plaque control and oral hygiene care • • • Tooth brush type: Medium Dentrifice: Salt-F® Brushing technique: up&down twice a day , duration: 2 mins Mouthrinse: Appliance: Abnormal oral habit: -

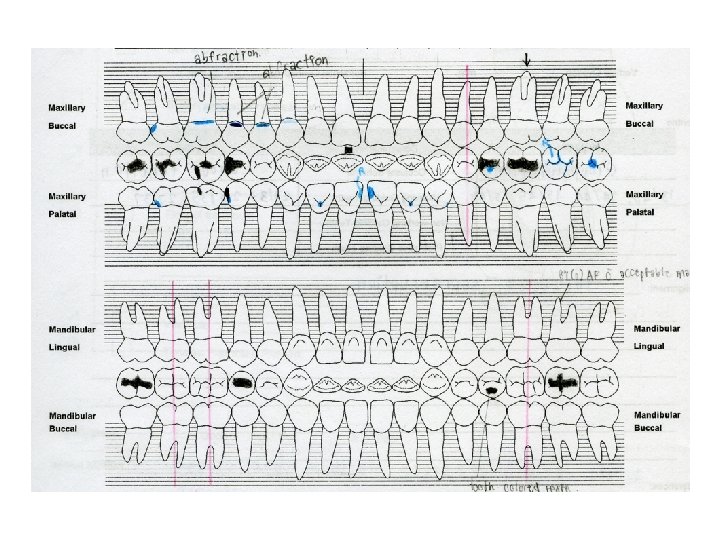
Area of chief complaint 15 OD amalgam filling under margin, hypersensitive to cold test 17 D large dental caries exposed pulp, sensitive to exploration, not sensitive to air blow, exploration and tenderness on percussion 13 B , 14 B , 15 B, 16 B abfraction, 14 O , 15 O erosion, not sensitive to exploration and air blow

Clinical examination 38 General appearance: WNL BP 178/111 mm. Hg, PR 89/min Extraoral examination : WNL Intra oral examination normal oral soft tissue except abrasive lesion sized 1 x 2 mm on alveolar ridge Bluish red in color at U/L anterior gingiva, round margin, bleeding on probing , gingival recession, pocket depth at posterior teeth, fistula opening leveling 2 mm from gingival margin of 37

Occlusion Centric unclassified Rt and Lt molar Rt and Lt canine Cl. I Eccentric 26/37 , 17/48 protrusive interference

Comprehensive evaluation • base line of information • analyzing, correlating, and synthesizing the information the diagnosis sequence has already begun

PQ 1

UA 11 tooth discoloration, EPT not response at 80 with control 21 response at 23 x-ray: radiolucency findings at apex 12 Pa , 21 M , 22 Pa , 28 O dental caries, not sensitive to exploration and air blow, patient has no any symptoms. 13 O, 23 O erosion, not sensitive to exploration and air blow, patient has no any symptoms.

PQ 2 25 OM amalgam filling present secondary caries, without symptom 25 O erosion 24, 36 missing teeth from tooth extraction 24: TP with ww, risky swallowing 26: supraeruption tooth 28 supraeruption induce abrasive tissue at gingival of 38
 37 tooth mobility,")
PQ 3 35 old tooth color filling (probably from erosion problem) 37 tooth mobility, pocket formation with pus exudate, protrusive interference, fistula tract opening near gingival margin

PQ 4 46, 47 missing teeth from tooth extraction 43 O , 45 O erosion, not sensitive to exploration and air blow, patient has no any symptoms.

Problem lists

Construct for Diagnosis

Diagnosis summary

Problem lists • 37: tooth mobility, pocket formation, protrusive interference, fistula tract opening • Bluish u/l anterior gingiva, round margin, bleeding on probing , pocket depth, fistula opening, bone loss, gingival recession, • Dental check when having a problem? • Concern in oral health care (? ? ) • Physiological attrition and pathological erosion associated with sour food (? ? ), loss of posterior teeth
cond’t) 4. 5. 6. 7. 7. 8. 9. 12 Pa , 21")
Diagnosis summary )cond’t) 4. 5. 6. 7. 7. 8. 9. 12 Pa , 21 M , 22 Pa , 28 O cavitated caries. 25 OM secondary caries. 13 B , 14 B, 15 B, 16 B abfraction; R/O parafunctional habit. TP with wrought wire 24, short extending 36 , 47 edentulous area; 28 supraeruption 28 unoccluded tooth erosion, premolar and canine, secondary to early loss of molar 10. Psychological disorder, by history

Problem lists • Dental check when having a problem? • Concern in oral health care (? ? ) • Physiological attrition and pathological erosion associated with sour food (? ? ), loss of posterior teeth Risk analysis: • High caries risk? • Risk of Non carious lesion? ? • Periodontitis risk? ?


Treatment plan 1. 2. 3. 4. 15 OD , 25 OM refilling. 12 Pa , 21 M , 22 Pa , 28 O , 13 B , 14 B , 16 B filling. 28 extraction 11 RCT ������� 17 ����������� 5. SC&RP 6. 17, 26 , 37, 48 Selective grinding

Treatment plan 7. Prosthodontic construction �� options ������ A. U/L removable partial denture D. 16 , 26 : Orthodontic intrusion 24 , 36 , 47: Fixed / removable partial denture B. 24 Fixed partial denture -/L removable partial denture E. Intentional endo+crown 16 , 26 24 , 36 , 47 Fixed / removable C. 24 implant partial denture -/L removable partial denture
 for medical information ( ), effect on dental")
Holistic plan 1. Physician consultation (psychiatrist) for medical information ( ), effect on dental management, relationship between stress and attrition 2. 15 refilling, pulp capping 3. Caries control define etiology for erosion and attrition 4. 37 drainage 5. 17, 11 endodontic treatment 6. Operative treatment 7. Occlusal adjustment 8. Crown construction, RPD design and crown ������� 9. OHI and evaluation 10. Observed for erosin and abfraction 11. Recheck and recall

• U/ TP, -/L RPD 1. 28 extraction 2. Crown construction for occlusal equilibration (cantilever bridge) 3. -/L RPD

Prosthodontic plan • Option 1 U/- RPD, -/L RPD • Option 2 Cantilever bridge, -/L RPD • Option 3 U/-TP, -/L RPD • Option 4 implant (alignment teeth by orthodontic treatment)

Solutions/Treatment for Chief complaints For the chief complaint such as pain, acute infection, bleeding, and traumatic injury require immediate attention • Palliative Treatment • Curative Treatment

Holistic plan 1. 15 OD : urgency treatment: Refilling 2. 17: restorable or extraction? : RCT, Crown lengthening, P&C, other options 3. Patient’s –Doctor’s concerns about main problems (spaces, occlusion, interference? ? ): Prosthodontic & Orthodontic considerations, selective grinding? ?

Holistic plan 1. 15 OD : emergency treatment: Refilling 2. 17: restorable or extraction? : RCT, Crown lengthening, P&C, other options 3. Patient’s –Doctor’s concerns about main problems (spaces, occlusion, interference? ? ): Prosthodontic & Orthodontic considerations, selective grinding? ? 4. What are the real causes, the relationship of problems? Why abfraction, caries, stress, no denture need? ?

Holistic plan Prosthodontic construction �� options ����� A. U/L removable partial denture D. 16 , 26 : Orthodontic intrusion 24 , 36 , 47: Fixed / removable partial denture B. 24 Fixed partial denture -/L removable partial denture E. Intentional endo+crown 16 , 26 24 , 36 , 47 Fixed / removable C. 24 implant partial denture -/L removable partial denture

Holistic plan May not be serious in sequence but should be combined with the long term treatments • 28 extraction • 11 RCT or observed? restoration? • Check for priority, relationship to other treatment: 25 OM refilling, 12 Pa , 21 M , 22 Pa , 13 B , 14 B , 16 B filling. • SC&RP: which areas first? Consider Prev. • Prevention in overall: caries, perio, abfraction, . . OHI, Fluoride, sugar consumption, listen to patients. . etc. .

PQ 3

Problem lists • Undiagnosed diseases that are suspected by the dentists • Hypersensitivity to medications or materials • Diagnosed medical conditions may increase the risk of serious complications during dental treatment • the patient’s dental problems other than the chief complaint

Listing possible solutions for patient problems to create diagnosis Problem lists • • Chief complaint General health problems Dental health problems Behavioral problems Potential solutions/ Treatment options Benefits: Organization Professional competency Patient education

A prioritised problem list • Include active and inactive problems • Prioritise from the most relevant to the patient’s • Define the problem using the most specific description supported by clinical data without over interpretation the findings

A prioritised problem list • A problem may be – Symptoms: patient description from history • Pain, fever, swelling – Signs: clinical exam findings • Fistular opening, blood-filled lesions on gingivae, tooth mobility – Radiograph data • Radiolucency at apex of tooth – Lab data • Increase neutrophil level, decrease platelet level – Known diagnosis • Medical diagnosis: congestive heart disease, gastritis • Dental diagnosis: fluorosis

Diagnosis approaches to pain • • • • Site or location Time and mode of onset Severity Nature Frequency Progression Duration Factors which relieve pain Factors which exacerbate pain Course of pain Radiation of pain to another site Cause of pain Associated findings How to take a history of pain?

Differential diagnosis for pain of dental origin • Pulpal pain – – – • Periodontal pain – – • burn Acute necrotizing ulcerative gingivitis Pericoronitis Desquamative gingivitis teething Tracking of pus from third molar Migratory abscess of the buccal sulcus Bone pain – – • Apical periodontitis Traumatic periodontitis Periodontal abscess Periodontal-endodontic lesions Gingival pain – – – – • Dentine hypersensitivity Cracked tooth involving the pule Pulpitis Aerodontalgia Alveolar ostetis Osteomyelitis infected dental cyst Trauma, fracture Pain associated with dental prostheses Usually • Unilateral • Never referred across to the other side of face • Periodontal pain is localized and the patient can point to the tooth invloved • Pulpal pain in poorly localized and may referred to another tooth on the same side of the arch, the opposite arch on the same side (usaually the same relative position, i. e. upper 5 to lower 5 region). Occasionally, pain may be referred to any tissues supplied by any branch of the trigeminal nerve on the same side. • The commonest source of pain in the region of the jaws is the dental pulp • Since common things occur commonly, eliminate them first! • A diagnosis local anesthetic injection may help to locate the arch and region from which pain is aring.

Diagnosis approaches to swellings When was the swelling first notice? What made the patient notice the swelling? Is the swelling painful? Is the swelling interfering with functions? Has the swelling changed since it was first noticed? Does the swelling ever disappeared or change its size during normal activity? • Has the patient ever had any other swellings? • Has the patient has any other associated symptoms? • What does the patient think caused the swelling? • • •

Diagnosis approaches to ulcers • Where was the ulcer first noticed • What drew the patient's attention to the ulcer • In what way does the ulcer trouble the patient? • Has the ulcer changed since it was first noticed? • Has the patient had a similar ulcer on the same site, or elsewhere? • Was the ulcer preceded or accompanied by any of the following features: blister? , peeling of the epithelium, a lump, colored or pigmented patches • Where there any accompanying general symptoms at the time of the ulcer formation? How to take a history of an ulcers?

Diagnosis approaches to ulcers Inspectation • Size and shape • Number • Position • Edge: undermined edge, punched out edge, sloping edge, raised edge, everted edge • Floor of ulcer • Discharge • Surrounding area • Depth • Bleeding • Relationship of ulcer with deeper structures • Surrounding skin/mucous membrane Palpation • Tenderness • Margin and edge of an ulcer on palpation • Association with regional lymph nodes How to examination of an ulcers?

Diagnosis approaches to swelling How to examination of a swelling?

Diagnosis approaches to ulcers How to examination of an ulcers?

Holistic plan 1. Based on a whole assessment 2. Based on a whole diagnosis; – Problems, needs and objectives of each patient: priorities…based on concerns. . • disease • illness: feelings, expectation, concerns – Individual tooth, all tooth, oral health, general health, oral health, behaviour, family, social, etc… – Relationship of causes/factors of patient’ s problems

Holistic plan. 4 Planned sequence of activities – From the ends through the starting point – Concern Chief Complaint (CC) first but may not be treated or completed (CC) first. . – Solve the real causes of the problems!! – Integration of Cure, Prevention, Promotion – Know the serious sequences, changeable ones (Consider time and management) – Consider emergency, urgency plan, referral care – Consider temporary/uncertain treatment – Consider holistic plan in terms of phases, visit plan? ? – Consider relationship of each plan with the context, concerns and overall plan of patients at present…

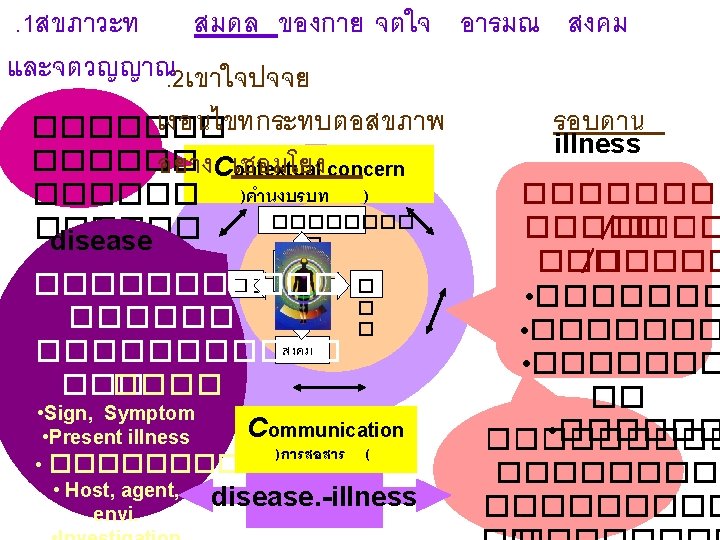
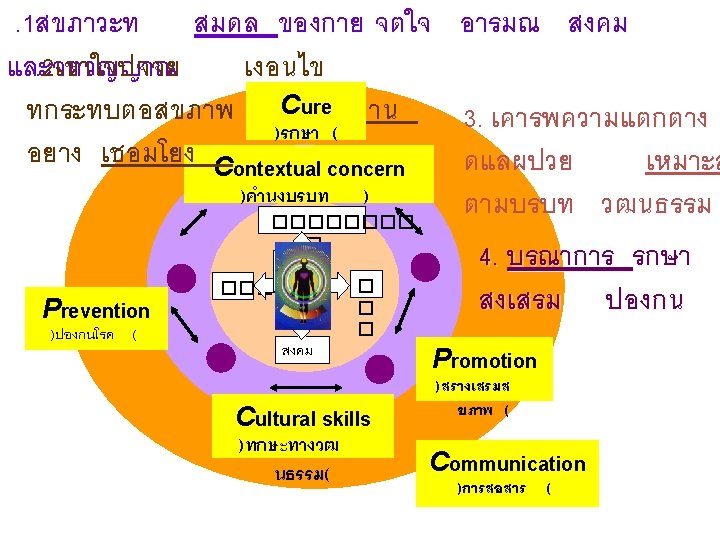
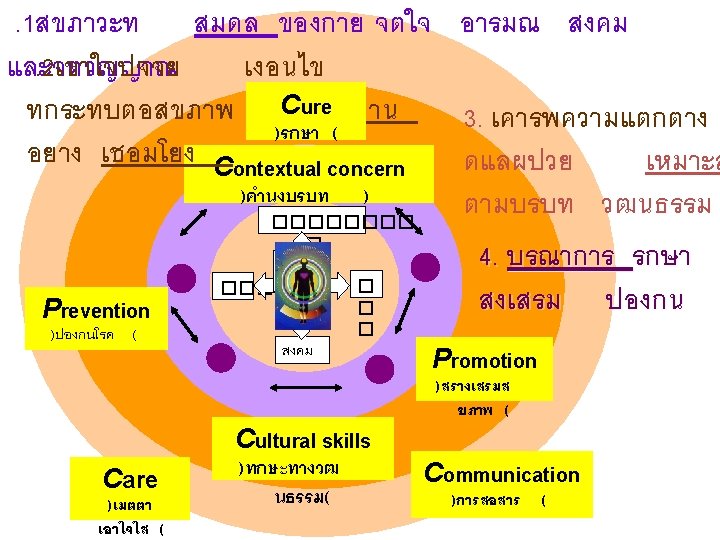
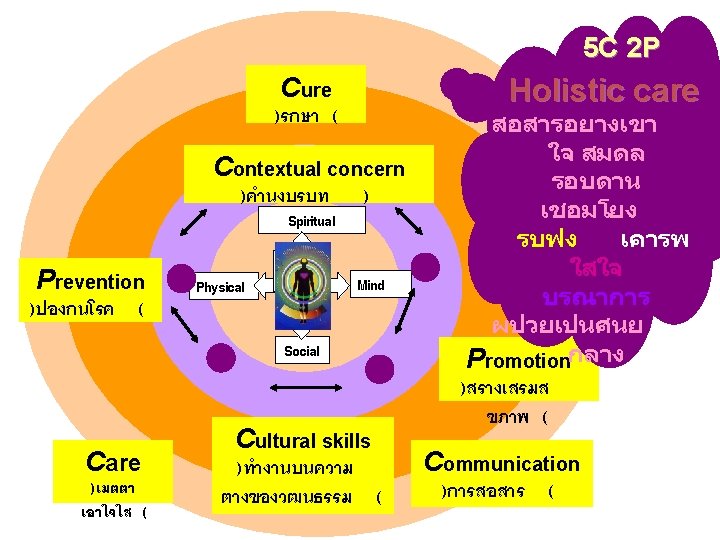
Holistic plan 4. Patient participation – Exchange doctor & patient’s perspective: • • • – Expectations/ goals Explain rationale, risks, benefits, anticipated outcomes, alternatives and prognosis of plan Share decisions…. Empowerment: self care. . …Health…Life… • • Positive approach Risk analysis and prevention and promotion 5. Patient-centred: based on patient’s situation, goals, context and perspectives (dynamic) 5 C 2 P : Cultural competency, Contextual concerns, Care, Cure, Prev, Prom, Communication


- Slides: 76