Hospice in HospitalGIP and Beyond Process and Experience

Hospice in Hospital—GIP and Beyond Process and Experience: 1 st Year Providence St Joseph Health, Sonoma County u. Gary A. Johanson, MD Palliative Care Services Medical Director Memorial Hospice and Home Health u. Advances in Palliative Care Conference u. Napa, CA u. November 2, 2017 11/5/2020 1

Objectives u u u Name 5 benefits of Hospice in Hospital HIH Describe the process of delivering Hospice care to patient in acute care hospital Understand challenges of starting up an HIH program 11/5/2020 this 2

Hospice-Hospital Partnerships 11/5/2020 this 3

Resources u NHPCO Compliance Tip Sheets u u 11/5/2020 this Regulatory Committee Acevedo Consulting Inc. Medicare Claims Processing Manual Medicare Benefit Policy Manual 4
 For patient and family u - 11/5/2020 this")
Benefits of Hospice in Hospital (HIH) For patient and family u - 11/5/2020 this Maximize concordance of care with goals Enhance Communication Optimize symptom management Grief support 5
 For Hospital: u Mission: Improve quality of end")
Benefits of Hospice in Hospital (HIH) For Hospital: u Mission: Improve quality of end of life experience in its many dimensions Improve patient satisfaction & community image Improve identification of expected death u u 11/5/2020 this Mortality metrics more accurately reflective of hospital performance Premier vs CMS criteria for exclusion Cost off-sets 6
 For Hospice: u - 11/5/2020 this Extend influence")
Benefits of Hospice in Hospital (HIH) For Hospice: u - 11/5/2020 this Extend influence of Hospice philosophy into hospital setting Enhance referral timeliness Integrate hospice services within the broader continuum of palliative services 7

Level of Care and Location LEVELS OF HOSPICE CARE HOME OPTIMAL FACILITY RESIDENTIAL HOSPICE GIP (General In-patient) NO Acute is most practical; SNF ok, but compromised YES ROUTINE YES Home, B&C, SNF Acute ok, but not ideal. YES RESPITE NO SNF when at all possible; must meet certain criteria YES CONTINUOUS CARE YES Home and B&C [In lieu of continuous care] 11/5/2020 this 9

Initial Steps Multi-stakeholder meetings u CEO: Hospital, Post-acute, Hospice CMO, CNO, COO Palliative, hospice, and hospitalist clinical leaders Quality, Registration, UR, C/M, Population Health - Many meetings/phone conferences since u - 11/5/2020 this Local team as well as representatives of So. Cal region Operations: Registration, quality, IT, compliance Clinical: Palliative, hospice, intensivists, hospitalists, nursing, social work, spiritual, pharmacy 10

Issues addressed u u u u u OSHPD requirements Premier mortality metrics Registration and transfers Physician staffing and roles Hospice staffing and education Hospital RN and staff education EMR documentation (Meditech) Medical Orders and Pharmacy transitions Policies and Procedures 11/5/2020 this 11

OSHPD: Office of Statewide Planning and Development Medical Information Reporting: 10/1/15 Discharge to Hospice does not qualify as a D/C Patient must either u u u Be formally released AND leave facility Transfer to ARU, psych, drug rehab, or skilled Leave AMA Die - u Otherwise one continuous stay even if leased space to a hospice 11/5/2020 this 12

Mortality Composite and Overall Scores u u Reduction in admissions for advanced illness difficult or undesirable to prevent death Reduction in preventable deaths through care bundles, order sets, teams, best practices Documentation of severity of illness Role of Hospice and Palliative Care and postacute world 11/5/2020 this 13

Mortality Composite and Overall Scores Premier u - If on Hospice by time of discharge, reported as expected death and excluded from mortality CMS u - Hospice within last year or started on Hospice by 1 st midnight 11/5/2020 this 14

Registration and Transfers Most sites do discharge and readmit u - 11/5/2020 this Does not meet OSPHD requirements in California Inefficient with much paperwork and extra coordination Creation of “Ghost Bed” Variable period of time shut off from pharmacy 15

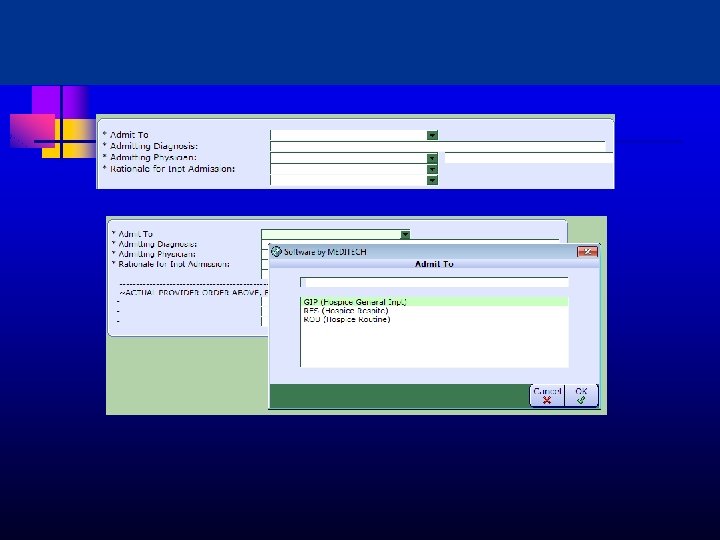
Registration and Transfers Split Billing u MD order triggers internal HIH Admission Notification in Registration Dept Current in-patient acct changed to hospice acct Series of steps u u u 11/5/2020 this Level of care Insurance payer change New reason for visit 16

Hospice in Hospital


Physician Staffing and Roles Primary MD u - u u u PCP; Hospitalist; PC; Hospice Daily rounds Transfer CTI Daily GIP determination; coordination with hospice IDT and hospital Call schedule 11/5/2020 this 23

Hospice Nursing Staffing and Training u u u Huge challenge Familiarization with Medicare documentation requirements Irregular patient flow GIP determinations Education of hospital staff 11/5/2020 this 24

Hospital Nursing Education u u u Familiarization with process Collaboration essentials Promote advocacy for patient Managing stress and grief Accessing Hospice team in a timely fashion 11/5/2020 this 25

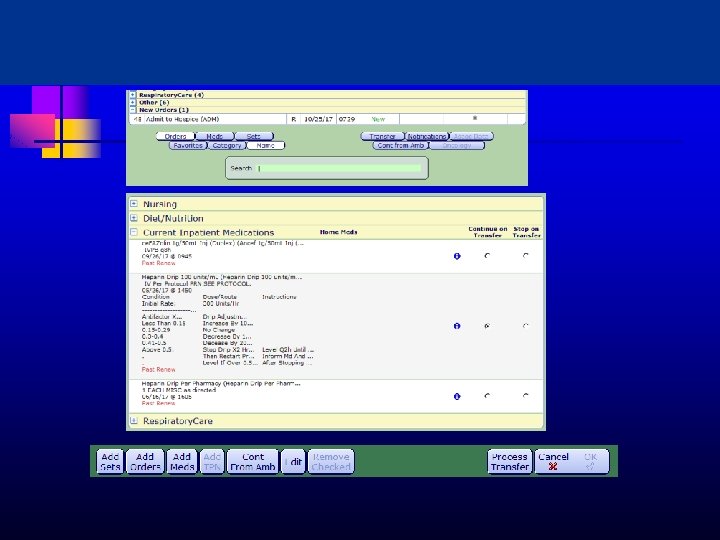
EMR Documentation u u Templates for palliative and hospice documentation Mapped to PCQN for automatic upload to a central shared database 11/5/2020 this 26

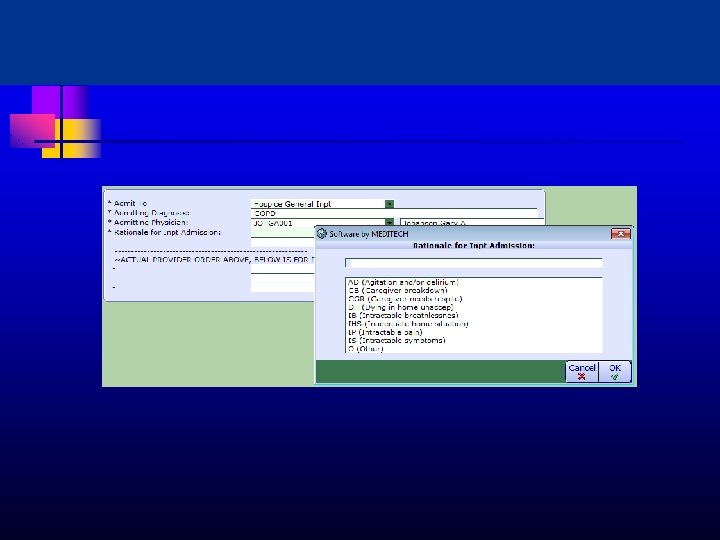
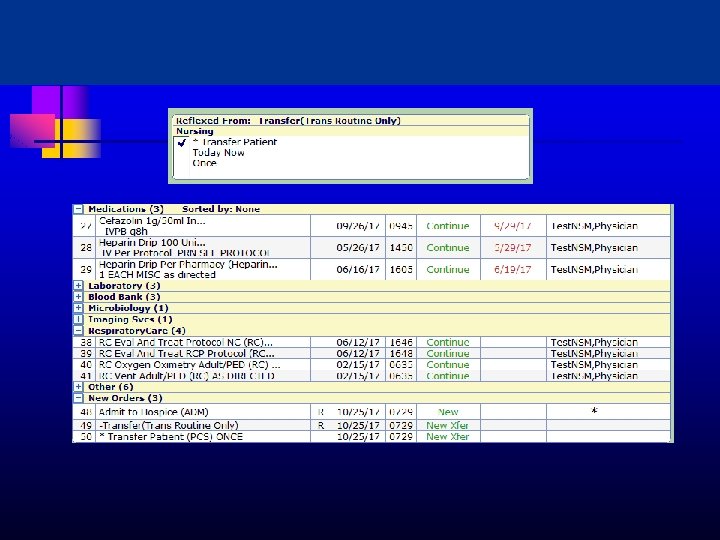
Order Sets Transfer order functionality End of Life order set Pharmacy coordination u u u - Rapid availability of agents for symptom crisis Subcut route Midazolam, IV haloperidol, fentanyl use on med surg RMAD—Rectal Medication Administration Device 11/5/2020 this 27



Step-wise HIH Process Decision by primary care team that hospice is appropriate or at least should be considered---family is prepped u - Hospice RN/SW assessment & consultation with hospice MD Once all in agreement and patient/family have signed on u u - A “Transfer” order is completed Plan of Care re-focused and medication orders adjusted Care is a collaboration of hospice team and hospital unit u - u Referral to PC vs Hospice in Hospital nurse directly Followed by primary MD/NP and Hospice MD Discharge possible but usually death in hospital 11/5/2020 this 35

Document Development Palliative vs Hospice vs Comfort Care Summary Message; Benefits and Burdens Policy Procedure u u - Roles and Responsibilities Next steps Tip sheets u u - Admission Checklist PCA and infusions 11/5/2020 this 36

Roles and Responsibilities 11/5/2020 this 37
 CMS designated term for PCP")
Provider Billing u u - Attending of Record (AOR) CMS designated term for PCP “most significant role in the determination and delivery of medical care” Bills Part B—requires modifier ALL other physicians bill Hospice (Part A) Must have contracts w/ hospice already “in place” All visits by Hospice physicians bill Hospice u Cannot be duplicative 11/5/2020 this 38

Hospice Medicare Billing 11/5/2020 this 39

Patient Profile Year 1 DATE TOTAL PTS TOTAL DAYS GIP ROUTINE 5/30/16 --6/30/16 8 34 24 10 7/1/16 --6/30/17 135 426 161 265 7/1/17 --9/30/17 41 115 43 72 TOTAL 184 575 228 347 11/5/2020 this 40

Patient profile year u u LOS prior to hospice transition completed Average 8. 1; Range 0 -25; Mode 4 -8 LOS on Hospice in Hospital Average 3 days; Range 1 -14; Mode 2 -3 41

Case 1 u u u 68 yo woman retired RN newly dx stage IV lung CA and rapid progression SOB placed on Hi Flow 02 Hospice referral with attempted wean to discharge home GIP while weaning…balked Transfer to ROUTINE—explored dispo Back to GIP 8 days later 11/5/2020 this 42

Case 2 u u 77 yo man with progressive cancer pain Pain still problematic days after admission and clearly declining and unable to discharge Infusion begun and titrated to relief Daughter commented he had not been that comfortable for months 11/5/2020 this 43

Case 3 u u 64 yo homeless man with nil intake in context of metastatic lung CA Symptoms were controlled and fading sensorium Survival expectation 3 -6 days but no practical place to send him. Began Hospice ROUTINE and with continued hospice support, his last days and staff’s sense of well being were greatly enhanced 11/5/2020 this 44

Successes u u u u u Countless family and staff testimonials 184 patients and families Oncology floor welcome: clarity and support Positive involvement in ICU extubations Elevation of hospice and palliative in eyes of hospital community Added impetus to Hospice House Significantly measureable effect on mortality scores Initial skepticism faded to near nil at this time Plan to pilot at Petaluma Valley Hosp in January 11/5/2020 this 45

Successes u u u Plans to expand ED presence Palliative sedation and major pain issues Tracking mechanisms Weekly IDT meetings at the hospital Coordination with Palliative Care 11/5/2020 this 46

Ongoing Challenges Careful documentation of GIP Coordinating timely orders for symptom flares Managing Hospice capacity Emergency Department direct admission Upstream identification of patients u u u - Advance Care Planning Predictive modeling Expand post-acute care capacity Engage PCP’s and medical homes Navigators as oversight coordinators Disposition u 11/5/2020 this Residential Hospice 47
- Slides: 42