Hormonal Agents Estrogen Androgen Inhibitors GonadotropinReleasing Hormone Agonists

Hormonal Agents Estrogen & Androgen Inhibitors Gonadotropin-Releasing Hormone Agonists Aromatase Inhibitors Tamoxifen Leuprolide Aminogluthethimide

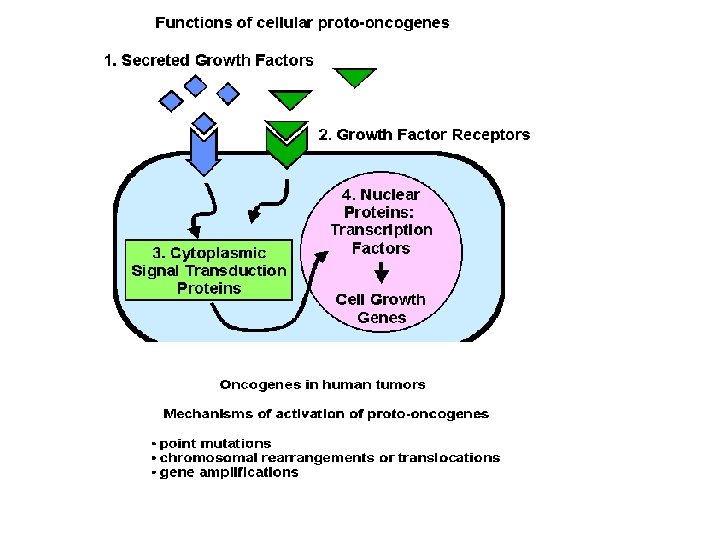
HORMONE ANTAGONISTS • Tumours derived from hormone-sensitive tissues may be hormone-dependent. • Their growth can be inhibited by (1) hormones with opposing actions, (2) hormone antagonists (3) inhibit hormone synthesis. • Hormones, or hormone analogues which themselves have inhibitory actions on particular tissues can be used in the treatment of tumours of those tissues.
, have both estrogenic and antiestrogenic effects on")
Tamoxifen • Selective estrogen receptor modulator (SERM), have both estrogenic and antiestrogenic effects on various tissues • Tamoxifen competitively binds to estrogen receptors on tumors and other tissue targets, producing a nuclear complex that decreases DNA synthesis and inhibits estrogen effects. • Patients with estrogen-receptor (ER) positive tumors are more likely to respond to tamoxifen therapy, while the use of tamoxifen in women with ER negative tumors is still investigational.

Tamoxifen • When used prophylatically, tamoxifen has been shown to decrease the incidence of breast cancer in women who are at high risk for developing the disease • It is active orally and is therefore particularly useful in maintenance therapy. • Hot flashes, Fluid retention, nausea are the main side effect. • Tamoxifen acts as partial agonist on the endometrium and has been linked to endometrial cancer in some women.

ANTIANDROGENS • such as Flutamide bind to androgen receptors and are effective in the treatment of prostate cancer. • It competes with testosterone and its powerful metabolite, dihydrotestosterone (DHT) for binding to androgen receptors in the prostate gland. • By doing so, it prevents them from stimulating the prostate cancer cells to grow. • Flutamide has been largely replaced by a newer member of this class, bicalutamide, due to a better side-effect profile.

Aromatase inhibitors • Aminoglutethimide is an example • It blocks the production of steroids derived from cholesterol and is clinically used in the treatment of Cushing's syndrome and metastatic breast cancer It blocks aromatase in the generation of estrogens from androstenedione and testosterone. It is a 2 nd line choice for the treatment of hormone sensitive metastatic breast cancer. Aminoglutethimide main side effects are : Dizziness, Lethargy, Visual blurring, Rash.

Aromatase inhibitors • Anastrozole is the newer agent that have less problem • Treats advanced estrogen and progesterone receptor positive breast cancer that is no longer responsive to tamoxifen. • Bone weakness is the main side effect.

Gonadotropoin-Releasing Hormone Agonist • Agents act as Gn. RH agonist, with paradoxic effects on the pituitary • Initially stimulating the release of FSH and LH, followed by inhibition of the release of these hormones • Resulting in reduced testicular androgen synthesis

Gonadotropoin-Releasing Hormone Agonist • Clinical uses includes a. Metastatic carcinoma of the prostate b. Hormone receptor-positive breast cancer • Given as depot preparations (monthly or yearly) • Side effects of the Gn. RH agonists are signs and symptoms of hypoestrogenism, including hot flushes, headaches, and osteoporosis.

HORMONES AS DRUGS • GLUCOCORTICOIDS have inhibitory effects on lymphocyte proliferation and are used in treating lymphomas and leukaemias. • REDNISONE is an example; that used to induce remission in the treatment of lymphocytic leukaemia and in the treatment of Hodgkin and non Hodgkin lymphoma. • The mechanism is unclear, may related to decrease glucose transport and decrease the available energy, or may related to the inhibition of protein synthesis and retard mitotic division in the cells.

Targeted therapy • Medication which blocks the growth of cancer cells by interfering with specific targeted molecules needed for carcinogenesis & tumor growth. • rather than by simply interfering those rapidly dividing cells. • selectively disrupt critical cancer pathways that are deregulated in a given type of cancer. • Targeted therapy can be divided into: (1) Small molecules (2) Monoclonal antibodies

Imatinib • Philadelphia chromosome or Philadelphia translocation is a specific chromosomal abnormality that is associated with chronic myelogenous leukemia (CML). • This translocation results in the Bcr-Abl fusion protein, the causative agent in CML, and is present in up to 95% of patients with this disease. • Imatinib is an inhibitor of the tyrosine kinase domain of the Bcr-Abl oncoprotein and prevents the phosphorylation of the kinase substrate by ATP.

Gleevec is one of the most effective modern medications for cancer treatment, .
 tyrosine")
Gefitinib • is the first selective inhibitor of epidermal growth factor receptor's (EGFR) tyrosine kinase domain. • EGFR is overexpressed in the cells of certain types of human carcinomas - for example in lung and breast cancers. • This leads to inappropriate activation of the anti-apoptotic Ras signal transduction cascade, eventually leading to uncontrolled cell proliferation. • Gefitinib inhibits EGFR tyrosine kinase by binding to the (ATP)binding site of the enzyme. Thus the function of the EGFR tyrosine kinase in activating the Ras signal transduction cascade is inhibited, and malignant cells are inhibited.

Beyond Chemotherapy EGF Binds to Receptor Resulting in Dimerization and Autophosphorylation EGF TK TK EGF TK Increased cell proliferation, inhibition of apoptosis, neoplastic angiogenesis p. Y TK p. Y Activation of intracellular signaling molecules clinicaloptions. com/oncology

Beyond Chemotherapy EGFR Cell membrane Shc Grb 2 Sos-1 PI 3 -K AKT “Downstream” signaling proteins STAT 3 Raf Synergy STAT 3 MEK m. TOR ERK Cancerrelevant outputs Resistance to drugs Proliferation Blood vessel growth Metastasis clinicaloptions. com/oncology

Mab. Thera

Bevacizumab inhibits the action of VEGF, a blood vessel growth Factor When VEGF is bound to Bevacizumab, it cannot stimulate the formation and growth of new blood vessels • prevents VEGF from binding to its receptor • adds to the effects of chemotherapy in cancers like bowel and lung • FDA approved for: – First-or second-line Colorectal cancer treatment in combination with 5 -fluorouracil-based chemotherapy – Unresectable, locally advanced, recurrent or metastatic nonsquamous non-small-cell lung cancer in combination with carboplatin and paclitaxel

Bevacizumab Serious side effects include: • bowel perforation • impaired wound healing • bleeding • kidney damage More common side effects of Are: high blood pressure • tiredness/weakness • clots in veins • diarrhea
 is overexpressed in 25% to")
Trastuzumab • HER 2 (epidermal growth factor receptor family) is overexpressed in 25% to 30% of breast cancers • Trastuzumab is an anti-HER 2 monoclonal antibody for HER 2 positive metastatic breast cancer treatment • Approved for adjuvant treatment of HER 2 -positive breast cancer (in combination with doxorubicin, cyclophosphamide, and paclitaxel) in 2006

Breast cancer and Childhood ALL
 • cyclophosphamide/MTX/5 FU (CMFx 6) • studies have demonstrated")
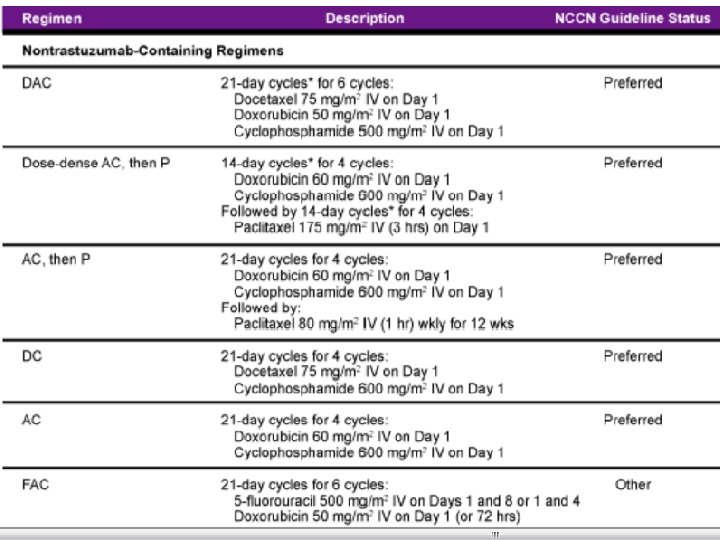
Anthracyclines • doxorubicin/cyclophosphamide (ACx 4) • cyclophosphamide/MTX/5 FU (CMFx 6) • studies have demonstrated an incremental benefit to anthracycline-containing regimens, particularly with Her-2/neu positive breast cancers
 HER 2 (+)")
Stage II Trial Paclitaxel Cyclophosphamide 600 mg/m 2 Tamoxifen if HR(+) HER 2 (+) Doxorubicin 60 mg/m 2 Etc. Herceptin
 Paclitaxel 90 mg/m 2 Surgery & RT Doxorubicin 60")
Stage IIIB Trial (HER 2+) Paclitaxel 90 mg/m 2 Surgery & RT Doxorubicin 60 mg/m 2 Dexrazoxane or Not Herceptin or Not Tamoxifen if HR(+) Cyclophosphamide 600 mg/m 2 Herceptin for a Year or Not

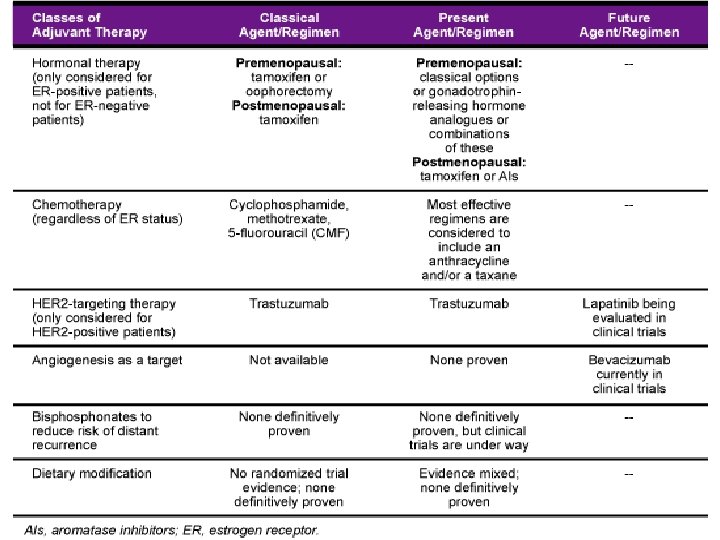
Drugs approved in Metastatic Breast Cancer Preferred first-line chemotherapy • Anthracycline-based. • Taxanes. • Cyclophosphamide, methotrexate and 5 -fluorouracil (CMF). Preferred second-line chemotherapy • If first-line was anthracycline-based or CMF, then a taxane. • If first-line was a taxane, then anthracycline-based or CMF.
 – Leukemia-free survival (LFS)")
Treatment results in ALL • Adults – Complete remission (CR) – Leukemia-free survival (LFS) 80 -85% 30 -40% • Children – Complete remission (CR) – Leukemia-free survival (LFS) 95 -99% 70 -80%

Chemotherapy for acute leukemias • Phases of ALL treatment – induction – intensification – CNS prophylaxis – maintenance post-remission therapy
 •")
Induction four to six weeks: • Vincristine • Glucocorticoid (prednisone, prednisolone or dexamethasone) • L-asparaginase • Anthracycline? ? ? In children with standard-risk ALL, such intensive induction therapy may actually increase morbidity and mortality and they standardly receive triple therapy with either anthracycline or asparaginase.

Consolidation • Once normal haematopoiesis is achieved, patients undergo Consolidation therapy. • Common regimens in childhood ALL include: 1. Methotrexate with mercaptopurine 2. High-dose asparaginase over an extended period 3. Reinduction treatment (a repetition of the initial induction therapy in the first few months of remission).

Maintenance • Maintenance usually consists 1. weekly methotrexate and 2. daily mercaptopurine. • 2 -3 years

CNS prophylaxis • Patients with ALL frequently have meningeal leukaemia at the time of relapse (50 -75% at one year in the absence of CNS prophylaxis) and a few have meningeal disease at diagnosis (<10%). • Intrathecal (methotrexate, cytarabine, steroids) • and for adult high-dose systemic chemotherapy (methotrexate, cytarabine, Lasparaginase)

Bisphonates are a drug class that prevent, reduce, and delay skeletal complications in cancer patients. Several mechanisms of action have been attributed to bisphonates, but they are noted for their ability to inhibit osteoclast-mediated bone resportion, or bone turnover. [61] In addition to their impact on preserving and rebuilding the skeletal system, there is also increasing evidence of a direct antitumor effect attributed to bisphonates.
- Slides: 35