Holdorf ULTRASOUND OF THE ABDOMEN PART I LECTURE

Holdorf ULTRASOUND OF THE ABDOMEN PART I LECTURE 10 URINARY TRACT II

Outline Acquired cystic disease Medullary sponge kidney Von Hippel-Lindau Disease Angiomyolipoma Tuberous sclerosis Renal cell carcinoma Renal metastases Wilm’s Tumor Acute pyelonephritis Chronic Pyelonephritis Xanthogranuomatous Pyelonephritis Pyonephrosis Mycetoma Acute renal failure Renal artery thrombosis Renal vein thrombosis Acute tubular necrosis Acute glomerulonephritis Hydronephrosis Nephrocalcinosis Papillary necrosis Renal sinus lipomatosis Urinary bladder Ureters Ureteral anomalies Transitional cell carcinoma Renal vascular ultrasound Resistive index Renal artery stenosis Renal transplantation Laboratory values

Acquired cystic disease Development of multiple cysts in chronically failed kidneys during long-term hemodialysis. Hemorrhage often occurs into these acquired renal cysts, resulting in pain and hematuria. These cysts do not function. Associated with an increased incidence of renal cell carcinoma.

Acquired Cystic Disease

Medullary Sponge Kidney Congenital dysplastic cystic dilatation of the medullary pyramids due to tubular ectasia or dysplasia. Ectatic collecting tubules may be seen on excretory urography. Due to urinary stasis, calcium deposits form in these dilated tubles. Sonographically, these calcium deposits appear as hyperechoic medullary pyramids.

Medullary Sponge Kidney

Von Hippel-Lindau Disease Inherited disease which usually presents in the second to third decade of life with serious visual impairment. Although Von Hippel-Lindau syndrome is characterized by retinal and central nervous system hemangioblastomas, sonographers need to be aware of other related tumors that can be found while performing a complete abdominal evaluation such as: Renal cell carcinomas Pheochromocytomas Islet cell tumors Renal and pancreatic cysts

Von Hippel-Lindau Disease

Angiomyolipoma Hyperechoic benign renal tumor. Its echogenicity is greater than or equal to that of the renal sinus. A propagation speed artifact may result in the posterior displacement of structures due to slower acoustic velocity in this fatty mass. CT confirmation of fat in an echogenic renal mass is considered diagnostic of Angiomyolipoma. 80% involve the right kidney.

Angiomyolipoma

Tuberous Sclerosis A multi-system genic disease that causes benign tumors to grow on organs such as the brain, kidneys, heart, eyes, lungs and skin. It commonly affects the central nervous system. The kidneys are the main focus of an abdominal sonographic evaluation in a patient with tuberous sclerosis. Patients with tuberous sclerosis have an increased incidence of renal cysts and Angiomyolipomas are typically bilateral in patients with tuberous sclerosis.

Tuberous Sclerosis-MRI of patient with Angiomyolipoma

Renal Cell Carcinoma Most common solid renal mass in the adult. Typically, it appears as a unilateral encapsulated mass. Nephrectomy is commonly recommended. Sonographically, it is hypoechoic relative to the normal adjacent renal parenchyma. Common presenting symptoms include: Hematuria (most common) Flank pain Palpable mass

Tumor extension into the renal veins and inferior vena cava is common. The lungs are the most common site of distant metastases. Lymph nodes, liver, bone, adrenal glands, and the contralateral kidney are also metastatic sites. Increased incidence associated with: Acquired cystic disease (chronic Dialysis) Von Hippel-Lindau Syndrome Tuberous sclerosis APKD

Renal Cell Carcinoma

Renal Cell Carcinoma

Renal metastases To the kidney Renal parenchyma may be the site of secondary tumors that have metastasized from other primary organs (such as the lung, breast, colon, etc…) Malignant cells from leukemia and lymphoma can metastasize to the kidney. Sonographically presents as: Hypoechoic masses of Diffusely enlarged inhomogeneous kidney.

Renal Metastases To the kidney
 is the most common CHILDHOOD renal tumor. Mean age at diagnosis")
Wilm’s tumor (nephroblastoma) is the most common CHILDHOOD renal tumor. Mean age at diagnosis is 3. 5 years. Patients typically present with a large asymptomatic flank mass. Other symptoms include: Hypertension Fever Hematuria

Metastasis can be seen to the lungs, bone, lymph nodes, and retroperitoneum. 90% survival rate with chemotherapy Tumor extension can be seen into the renal vein and IVC. Wilm’s tumors must be differentiated from adrenal neuroblastomas. Wilm’s tumors destroy the renal contour. If normal renal contour is maintained bilaterally, the abdominal mass is most likely an adrenal neuroblastoma.
 CNS tumors Lymphoma Neuroblastomas Soft tissue sarcomas Wilm’s")
Pediatric Cancer Incidence Leukemia (ALL) CNS tumors Lymphoma Neuroblastomas Soft tissue sarcomas Wilm’s tumors Bone Hepatic Tumors 35. 0% 16. 6% 15. 0% 7. 8% 7. 4% 6. 3% 6. 0% 1. 1%

Wilm’s Tumor

Acute Pyelonephritis Most renal infections occur via an ascending route from the bladder. They are usually caused by bacteria from the intestinal tract. Imaging studies are often unnecessary because the diagnosis of Pyelonephritis can be made clinically. Ultrasound findings include: Renal enlargement Hypoechoic parenchyma Absence of sinus echoes

When acute Pyelonephritis is focal, it is called acute focal bacterial nephritis or lobar nephronia. Sonographically, this appears as a focal wedgeshaped area or a hypoechoic renal lobe. A similar appearance can be seen in focal ischemia and renal infarction. Emphysematous Pyelonephritis is a bacterial infection associated with renal ischemia. More commonly occurring in diabetics. Immunosuppressed patients and patients with urinary tract obstructions. Bacteria produce inrarenal gas causing reverberation or comet-tail artifacts. Nephrectomy is usually required to treat infection.

Acute Pyelonephritis

Acute focal bacterial nephritis

Chronic Pyelonephritis Renal injury induced by recurrent renal infection due to: Anatomic anomalies Obstructive lesions Ureteral reflux Sonographically, chronic Pyelonephritis leading to end-stage renal disease appears as a small hyperechoic kidney with cortical thinning.

Chronic Pyelonephritis

Chronic Pyelonephritis
 Type of chronic phelonephritis resulting from chronic infections due to a")
Xanthogranulomatous Pyelonephritis (XGPN) Type of chronic phelonephritis resulting from chronic infections due to a long term obstruction. Associated findings include: Renal enlargement Parenchymal abscesses Staghorn calculus Papillary necrosis Hydronephrosis Pyonephrosis Loss of cortical-medullary boundary Cortical thinning

Failure to depict a normal kidney associated with a staghorn calculus suggest the diagnosis of XGPH

Staghorn Calculus cartoon

Staghorn calculus

Pyonephrosis Purulent material in the collection system of the kidney associated with an infection secondary to renal obstruction. Percutaneous or surgical drainage is required for adequate treatment. Ultrasound findings include hyperechoic debris in a dilated renal collecting system.

Pyonephrosis
 Candidiasis is the most common renal fungal disease. Fungal infections result")
Mycetoma (Fungal Ball) Candidiasis is the most common renal fungal disease. Fungal infections result from hematogenous seeding or ascending from the bladder. Fungus balls appear as hyperechoic, nonshadowing masses. Hematogenous =
")
Mycetoma (Fungal Ball)

Hyperechoic Renal Masses Mycetoma Angiomylipomas Blood clots Pyogenic debris Renal stones
 Reduction in glomerular filtration rate (GFR) resulting in an increase")
Acute renal failure (ARF) Reduction in glomerular filtration rate (GFR) resulting in an increase in blood nitrogen waste. Three main mechanisms of ARF: Prerenal failure (decreased perfusion) Hypotension Hypovolemia = Decreased blood volume Cardiac failure Renal artery stenosis (bilateral)

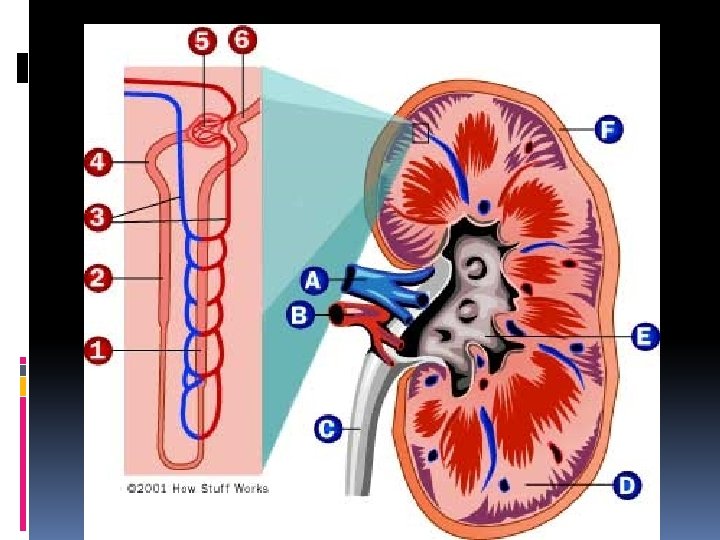
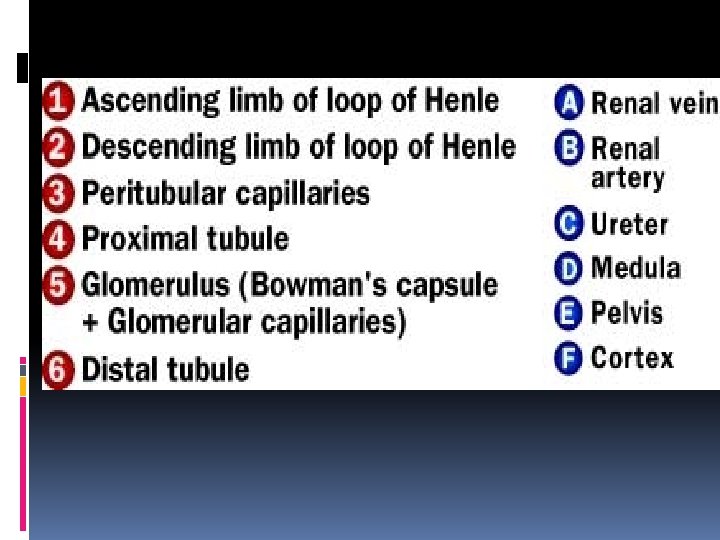
The glomerulus and its function
 renal failure acute tubular necrosis (most common) glomerular diseases (Nephritic syndrome) Interstial")
Intrinsic (intrarenal) renal failure acute tubular necrosis (most common) glomerular diseases (Nephritic syndrome) Interstial nephritis (Drugs or Contrast agents) Autoimmune disease

Ultrasound’s role in diagnosing the cause of acute renal failure is to determine: Hydronephrosis (indicates post-renal failure) Abnormal resistive index (<0. 7) Distinguishing the cause is important in relieving obstruction and in facilitating appropriate treatment of other renal medical disease. Prompt intervention prevents loss of renal parenchyma. Laboratory studies used to evaluate ARF: Urine output Urinalysis Blood urea nitrogen (BUN) Serum creatinine Changes in serum creatinine reflects changes in glomerular filtration rate, and is the most accurate method of determining ARF.

Renal function and Blood Pressure: What’s the connection? How does high blood pressure hurt the kidneys? High blood pressure makes the heart work harder and, over time, can damage blood vessels throughout the body. If the blood vessels in the kidneys are damaged, they may stop removing wastes and extra fluid from the body. The extra fluid in the blood vessels may then raise blood pressure even more. It's a dangerous cycle. High blood pressure is one of the leading causes of kidney failure, also called end-stage renal disease (ESRD). People with kidney failure must either receive a kidney transplant or have regular blood-cleansing treatments called dialysis. Every year, high blood pressure causes more than 25, 000 new cases of kidney failure in the United States.
 is a sudden cause of prerenal failure")
Renal Artery Thrombosis Renal artery thrombosis (occlusion) is a sudden cause of prerenal failure that presents as: Acute flank pain Hematuria Sudden rise in blood pressure

Renal Artery Thrombosis/stenosis

Renal Vein thrombosis Associated with Extrinsic compression Nephrotic syndrome Renal tumors Renal transplants Trauma Sonographic findings include: Dilated thrombosed renal vein Absent intrarenal venous flow Enlarged hypoechoic kidney High-resistance renal artery waveform (reversal of diastolic component)

High-resistance renal artery waveform

Low resistance RA Waveform

Acute Tubular Necrosis ATN is the most common cause of medical renal disease or intrinsic (intrarenal) acute renal failure. ATN results from prolonged ischemia or the exposure of nephrotoxins (drugs or contrast agents) causing damage to the tubular epithelium of the nephron leading to acute renal failure.

Acute Tubular necrosis can be reversible. Sonographic findings include: Renal enlargement Increased resistive index (RI) (>0. 7)

Acute Glomerulo-nephritis Acute glomerulo-nephritis is an inflammatory response resulting to glomerular damage caused by an autoimmune reaction, infection or exposure to toxins. Presenting symptoms include: Sudden onset of hematuria Proteinuria Azotemia: High concentrations of urea and creatinine (among other nitrogen containing compounds) in the blood. RBC casts in urine. Sonographic findings �Renal enlargement �Increased resistive index (RI)

Hydronephrosis Dilatation of the renal pelvis and calyces. The normal renal sinus is a central echogenic area composed of peripelvic fat, renal vessels, lymph nodes and collecting structures. Hydronephrosis produces a separation of the normal sinus echogenicity by an anechoic urine collection.

Hydronephrosis

Hydronephrosis: Severe

Hydronephrosis: Moderate

Hydronephrosis: mild

If untreated, hydronephrosis secondary to obstruction can lead to Hypertension Loss of renal function Sepsis Common causes include Calculi Benign prostatic hypertrophy (BPH) Prostate cancer Pelvic malignancies Pregnancy Uretero-pelvic junction obstruction
 Ureteropelvic")
Three common areas of obstruction by a stone: Uretero-vesical junction (Most common) Ureteropelvic junction Pelvic brim

Common sites of kidney stones

Blockage in the UPJ

Uretero-vesical junction

Obstructive nephropathy is also diagnosed by evaluating the intrarenal vascularity. A threshold resistive index (RI) of greater than 0. 7 is suggestive of obstructive hydronephrosis.
 that result in the formation of")
Nephro-calcinosis Disorders of calcium metabolism (hypercalcemia and hypercalciuria) that result in the formation of calcium renal stones and deposition of calcium salts in the renal parenchyma. Nephrolithiasis (renal stones) arise in the collecting system. The main symptom of renal stones is acute back or flank pain often radiating down to the ipsilateral groin. When severe, this can be accompanied by fever, chills, dysuria, cloudy urine and hematuria.
 Malignancies")
Causes of Nephrocalcinosis Hyperparathyrodism Vitamin D intoxication (too much) Malignancies

Nephrolithiasis-Renal Stones

Nephrolithiasis-renal stones 20 month neonate

Papillary Necrosis Ischemia of the medullary pyramids. Clinical diagnosis can be made by identifying sloughed papilla in the urine. Passage of sloughed papillae can cause pain and urine obstruction. Papillary necrosis is associated with the following conditions: Analgesic (painkiller) abuse – most common Diabetes mellitus Urinary tract obstruction and infections Renal vein thrombosis Sickle cell disease Chronic heart failure Cirrhosis
 Necrosis")
Medullary (renal Pyramid) Necrosis

Medullary Necrosis

Sonographic findings include: 1. echogenic material within the collecting system representing sloughed papillae 2. triangular cystic collections are seen represent the absence of medullary pyramids 3. Bright echoes produced by the arcuate arteries can be visualized at the periphery of the cystic space.

Renal sinus lipomatosis Increased renal sinus fat that replaces normal renal parenchyma. Ultrasound shows an increase in the central sinus echo complex with cortical thinning. Intravenous urography demonstrates compression of he calyces and renal pelvis by renal sinus fat.

Renal Sinus Lipomatosis

Urinary Bladder The urinary bladder is located behind the pubic bone. The apex points anteriorly and is connected to the umbilicus by the median umbilical ligament (urachus). The ureters enter the bladder at the superolateral angle of the trigone and exit the bladder via the urethra. Normal bladder wall thickness is typically < 5 mm in a non-distended bladder < 3 mm in a distended bladder

urinary bladder wall thickening

Bladder Anomalies Bladder diverticula are herniations of the bladder mucosa through the bladder wall musculature. They may be congenital or acquired.

Bladder diverticula

Urachal Cyst A urachal cyst is a cystic dilatation of the fetal urachus, which is the medial umbilical ligament connecting the bladder to the umbilicus. This is seen sonographically as a cystic structure superior and anterior to the bladder

Urachal Cyst

Ureters The ureters exit the kidney posterior to the renal artery and vein. At the hilum of the kidney Vein exits anteriorly Artery enters between the vein and ureter Ureter exits posteriorly Descending inferiorly, the ureters lie on the anterior surface of the psoas muscles. In the pelvis, the ureters cross anterior to the common iliac vessels to insert upon the trigone of the bladder.

Vein, artery, ureter

ureters

Cartoon of the ureters/trigone

Ureteral anomalies Ureteroceles Appear as a cyst-like enlargement of the lower end of the ureter which projects into the ladder lumen at the uretero-vesical junction. Ectopic ureteroceles Are usually associated with a duplex kidney and complete ureteral duplication. The distal ectopic ureterocele results in obstruction of the upper pole collecting system.

Ureterocele


Ectopic ureterocele
 is the most common bladder neoplasm. The")
Transitional Cell Carcinoma Transitional cell carcinoma (TCC) is the most common bladder neoplasm. The urinary tract is lined with transitional cells. Although transitional cell carcinoma may occur in the bladder, ureters or renal pelvis, it commonly occurs in the urinary bladder. A mass or focal thickening of the bladder wall should raise the suspicion of a TCC.

Hydronephrosis may be caused by TCC originating in the ureter. Hematuria is the most common clinical presentation. Other bladder masses include: Cystitis Prostate cancer Squamous cell cancer Blood clots Pyogenic debris

Transitional cell carcinoma of the bladder

Renal Vascular Ultrasound The normal renal artery demonstrates continuous forward flow during diastole, typical of low resistance blood perfusion.
 Resistive index is commonly used to Evaluate renal transplant rejection Access")
Resistive Index (RI) Resistive index is commonly used to Evaluate renal transplant rejection Access suspected hydronephrosis Evaluate medical renal disease Renal dysfunction, caused by a variety of reasons, results in a loss of diastolic flow, thus increased renal arterial resistance.
 – end diastolic frequency (velocity) Peak systolic frequency (velocity)")
RI=Peak systolic frequency (velocity) – end diastolic frequency (velocity) Peak systolic frequency (velocity) Normal resistive index is typically <0. 7 (in real world more like <. 08) Resistive index is a value comparing the amount of diastole to that of systole. It is a relative value (no units) that can be measured in frequency or velocity. If the RI = 0. 5 (diastole is 50% of systole) If the RI =. 07 (diastole is 30% of systole) If the RI = 1. 0 (diastole is absent)

Normal RI. 67

Abnormal RI

End stage renal failure/snowball kidney

Renal Artery Stenosis Symptoms of renal artery stenosis Sudden onset of hypertension Uncontrollable hypertension A hemodynamically significant renal artery stenosis may produce decreased renal size (< 9 cm in length) Renal artery evaluation methods: Direct evaluation – Renal artery velocities Renal artery / Aortic ratio (RAR) > 3. 5
 Absent early systolic peak Parvus Tardus")
Indirect evaluation Parvus Tardus (slow and late) Absent early systolic peak Parvus Tardus is defined as a small slow pulse.

Renal arteries

Renal stent

Parvus Tardus waveform
.")
Renal Transplantation Renal transplantation is the treatment of choice for end-stage renal disease (ESRD). Diabetes is the most common cause of renal disease leading to kidney transplantation. Pre-transplant evaluation of the living donor is important for screening and surgical planning. Harvesting the left kidney is favored due to its longer renal vein. Multiple renal arteries need to be identified (if present) as this will require additional surgical time.

The transplanted kidney can be placed on either side of the pelvis. The ureter is attached to the urinary bladder. The arterial anastomosis may be with the external or internal iliac artery. Poor function of the renal transplant may be the result of acute tubular necrosis (ATN) in the immediate post-transplantation period. Ultrasound is the most common imaging procedure of the renal transplant. It is utilized in accessing: Immediate surgical complications Location for renal biopsy Vascular status in acute rejection.
 �Urinomas (24 hours")
Post-transplant complications include: Fluid collections: �Hematomas (24 hours post op) �Urinomas (24 hours post op) �Abscesses Renal artery kinking or thrombus Renal vein thrombosis

Renal Transplant
 Loss of")
Sonographic findings of acute renal rejection include: Renal enlargement (increased length) Loss of cortical medullary boundary The resistive index (RI) is used to evaluate arterial flow resistance of eth renal vascular bed. <0. 7 = normal resistive index 0. 7 -0. 8 = questionable transplant dysfunction >0. 8 = transplant dysfunction

Laboratory values Urinalysis: includes the microscopic examination of sediment and qualitative evaluation of protein, glucose, blood, nitrites and white blood cells. Serum creatinine: serum concentration of creatinine is reversely related to glomerular filtration rate (GFR). Blood Urea Nitrogen (Bun): is unsuitable as a single measure of renal function because it varies with urine flow rates and production of ureas.

1. What is medullary sponge kidney? 2. Describe the sonographic appearance of medullary sponge kidney. 3. What is the most common cause of an abdominal mass in the newborn? 4. List four sonographic features of multiple dysplastic kidney disease. 5. What contra-lateral renal abnormalities are found when Multicystic dysplastic kidney disease is unilateral?

6. What are four sonographic criteria for a simple cyst? 7. What three criteria suggest that a cyst is atypical and possibly malignant? 8. Bilateral enlargement of the adult kidney caused by numerous cysts of varying sizes is seen with which disease? 9. Describe the sonographic appearance of infantile polycystic kidney disease. 10. Infantile polycystic kidney disease results in renal dysfunction. What other anomalies are associated with infantile polycystic kidney disease?

11. Name three anatomic anomalies that appear as pseudo tumors of the kidney. 12. What is the term which refers to patients on chronic hemodialysis that develop bilateral renal cysts? 13. What would a Sonographer look for in a patient with a history of tuberous sclerosis? 14 What are other names for a renal cell carcinoma? 15. Renal cell carcinoma is associated with what four disease?

16. Renal cell carcinoma Sonographically appears as an encapsulated, solid mass that is hypoechoic relative to normal, adjacent renal parenchyma. What additional areas should be evaluated whenever a solid renal mass is detected? 17. What common sonographic artifact is demonstrated with renal Angiomyolipoma, and adrenal myelolipoma? 18. What mass should be suspected when a filling defect is noted in the bladder? 19. What is the most common solid tumor in children diagnosed by ultrasound? 20. What are the ultrasound findings associated with significant acute pyelonephritis?
- Slides: 112