HIVAIDS An Update Allison M Liddell MD Infectious


 z 1981: AIDS recognized z Kaposi’s")


























 vl<105 vl>105 0 -49 16")










 + (zidovudine or")
 +")
 High rate of virologic failure z")
 High pill burden/ Dosing inconvenience Lack")























 z 1981: AIDS")























- Slides: 101
HIV/AIDS An Update Allison M. Liddell, MD Infectious. Care January 2 nd, 2006
HIV Curriculum z. Year 1: HIV Pathogenesis and Antiretroviral Therapy z. Year 2: Opportunistic Infections z. Year 3: HIV miscellaneous issues: Postexposure prophylaxis, pregnancy, neurologic disease, wasting syndrome, new drugs, HIV stigma, other special groups.
HIV Background z Late 1970’s Retroviruses described (HTLV) z 1981: AIDS recognized z Kaposi’s sarcoma, PCP appeared z risk groups identified z 1982: theory of HIV z 1983: HIV-1 identified z blood supply screening z 1983 AZT approved z 1994 PI’s approved z 1994 PACTG-076
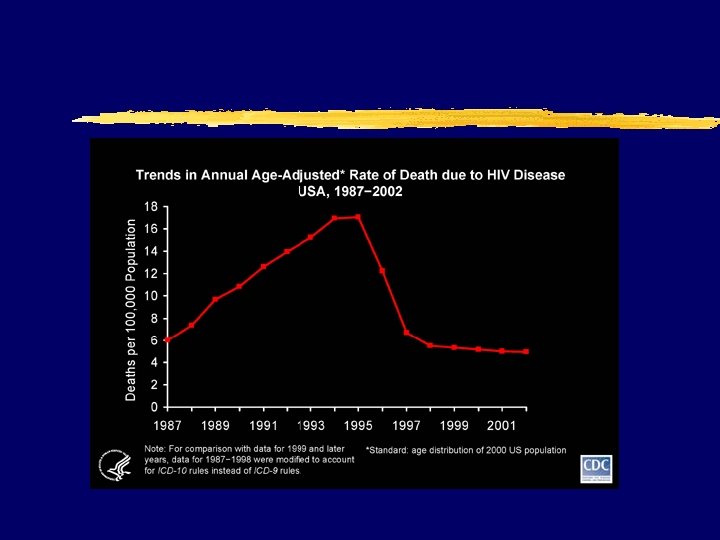
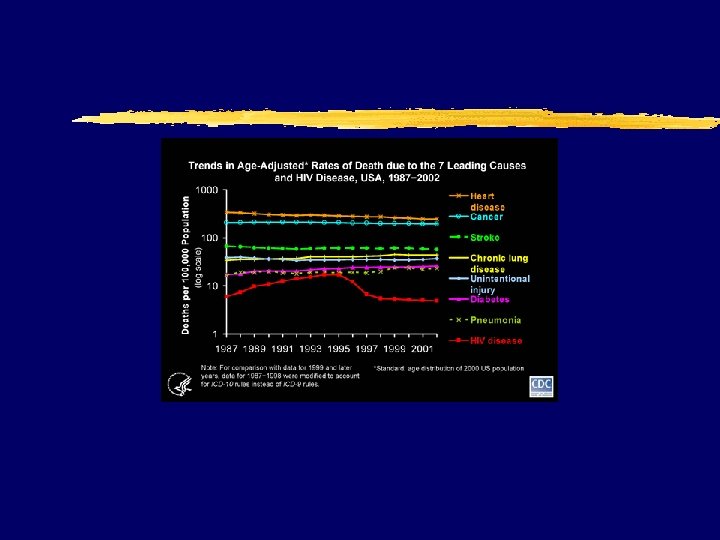
AIDS incidence
The HIV alphabet z HIV z AIDS z CD 4 z OI z HAART = Highly Active Antiretroviral Therapy z PI = Protease inhibitor (ritonavir) z NRTI = nucleoside reverse transcriptase inhibitor (zidovudine) z Nt. RTI= nucleotide… (tenofovir) z NNRTI = Nonnucleoside reverse transcriptase inhibitor (efavirenz)
AIDS case definition z CDC: 1993 Revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR 1992; 41(no. RR-17). z includes all HIV-infected persons who have less than 200 CD 4+ T-lymphocytes/u. L or a CD 4+ T-lymphocyte percent of total lymphocytes less than 14 z added pulmonary tuberculosis, invasive cervical cancer, or recurrent pneumonia to list of >20 AIDS defining illnesses
HIV virion
HIV pathophysiology z transmission via mucus membrane or iv exposure to infected body fluids z gp 120 binds CD 4 with CCR 5 z secondary role late of CXCR 4 for cell entry z Dramatic genetic and phenotypic variation yclades ydrug resistance z Nonprogressors z HIV-2 y. Rare in US -77 cases through 12/97 ycontributes on Africa
HIV pathogenesis
HIV pathophysiology z Progressive depletion of CD 4 cells z OI’s yfungal yviral ybacterial yprotozoal z malignancies y. Kaposi’s (HHV-8) ylymphoma ycervical cancer z 50% develop neurologic disease ydementia yvacuolar neuropathy yperipheral neuropathy
HIV natural history Sande: The Medical Management of AIDS, 6 th ed. , Copyright © 1999 W. B. Saunders Company
HIV infection diagnosis Sande: The Medical Management of AIDS, 6 th ed. , Copyright © 1999 W. B. Saunders Company
HIV diagnosis
Four FDA-approved Rapid HIV Tests Ora. Quick Advance - whole blood - oral fluid - plasma Uni-Gold Recombigen - whole blood - serum/plasma Reveal G 2 - serum - plasma Multispot - serum/plasma - HIV-2
Ora. Quick Advance HIV-1/2 z CLIA-waived for finger stick, whole blood, oral fluid; moderate complexity with plasma z Store at room temperature z Screens for HIV-1 and 2 z Results in 20 minutes
Collect oral fluid specimens by swabbing gums with test device. Gloves optional; waste not biohazardous
Positive Predictive Value of a Single Test Depends on Specificity & Varies with Prevalence Predictive Value, Positive Test HIV Prevalence 10% 5% 2% 1% 0. 5% 0. 3% 0. 1% Test Specificity Ora. Quick Reveal Uni-Gold Single EIA 99% 98% 95% 91% 83% 75% 50% 92% 85% 69% 53% 36% 25% 10% 97% 95% 87% 77% 63% 50% 25% 98% 96% 91% 83% 71% 60% 33% 99. 9% 99. 1% 99. 7% 99. 8%
Routine HIV Screening for Emergency Department Patients z Ora. Quick testing since October 2002 y 60% accept HIV testing y 98% receive test results y 2. 5% new HIV positive y 80% entered HIV care Cook County Hospital, Chicago z 4 new demonstration projects (Wisconsin, Massachusetts, Los Angeles, New York)
Characteristics Rapid Test Positive Patients
Advancing HIV Prevention: New Strategies for a Changing Epidemic z Four priorities: 1. Make voluntary HIV testing a routine part of medical care 2. Implement new models for diagnosing HIV infections outside medical settings 3. Prevent new infections by working with persons diagnosed with HIV and their partners 4. Further decrease perinatal HIV transmission MMWR April 18, 2003
HIV diagnosis z. Median time to development of detectable antibody is 2. 1 months; 95% develop antibody within 5. 8 months. z 40 -60% have symptoms of acute HIV infection zhigh levels of plasma HIV RNA, infectious free virus in plasma, and plasma p 24 antigen levels in acute infection
Acute HIV Infection: Treatment Possible benefits: Possible risks: z Decrease the severity of acute disease z Alter the viral “set point” z Reduce the rate of mutation z Preserve immune function z Reduce risk of viral transmission z Drug-related adverse effects on quality of life z Earlier emergence of drug resistance z Limitation of future treatment options z Potential need for indefinite treatment
HIV Chronic Infection z Establish relationship z Establish stage of disease z Counsel regarding prognosis and transmission (including vertical) z Screen for coexisting OI y RPR y toxo y hepatitis y tuberculosis y ROS y neurologic exam y skin exam y PAP smear, GC/chlaamydia z Lipids z Resistance testing
AIDS Drug therapy
Prognosis per CD 4 3 year probability AIDS/death (%) vl<105 vl>105 0 -49 16 20 5 -99 12 16 100 -199 9. 3 12 200 -349 4. 7 6. 1 >350 3. 4 5. 4
Mellors JW, Munoz A, Giorgi JV, et al. Plasma viral load and CD 4+ lymphocytes as prognostic markers of HIV-1 infection. Ann Intern Med, 1997. 126(12): p. 946 -954.
Indications for Initiation of Therapy: Chronic Infection z. Defer therapy for patients with viral load <100, 000 and CD 4 >350 (2005 recs)
HIV treatment considerations z Goals y Maximal and durable viral suppression (by 16 -24 wks) y Restoration and/or preservation of immunologic function x. CD 4 rise 100 -150/year y Improved quality of life y Reduction of HIV-related morbidity and mortality z Toxicity z drug interactions z disease interactions z pharmacokinetics z Adherence z HIV expertise y>20 pts asso w/improved outcomes y>50 even better
HIV treatment considerations Tools to Achieve Goals of Therapy · Maximize adherence to the antiretroviral regimen · Address substance abuse, depression, lack of social support · Rational sequencing of drugs · Preservation of future treatment options · Reserve 2 classes · Use of resistance testing in selected clinical settings
Antiretroviral agents z. NRTIs y. Always use at least 2 z. NNRTIs z. Protease inhibitors z. Fusion inhibitors
HIV Drug therapy
Inhibition of Fusion HIV-1 gp 41 CCR-5 gp 120 CD 4 gp 41 ENF
Current Antiretroviral Medications NRTI z z z z Abacavir Didanosine Emtricitabine Lamivudine Stavudine Zidovudine Zalcitabine Tenofovir NNRTI z Delavirdine z Efavirenz z Nevirapine PI ABC DDI FTC 3 TC D 4 T ZDV DDC TDF DLV EFV NVP Amprenavir Atazanavir Fosamprenavir Indinavir Lopinavir Nelfinavir Ritonavir Saquinavir y soft gel y hard gel y tablet z Tipranavir z z z z Fusion Inhibitor z Enfuvirtide APV ATV FPV IDV LPV NFV RTV SQV SGC HGC INV TPV T-20
Initial Treatment: Preferred Regimens NNRTI-Based z. Efavirenz* + (lamivudine or emtricitabine) + (zidovudine or tenofovir) pills/day 2 -5 PI-Based z. Lopinavir/ritonavir (Kaletra) + (lamivudine or emtricitabine) + zidovudine 8 -10 *Avoid in pregnant women and women with high pregnancy potential.
Selection of 2 NRTIs as Part of Combination Therapy Preferred: (zidovudine or tenofovir) + (lamivudine or emtricitabine) Alternative: (stavudine or didanosine or abacavir) + (lamivudine or emtricitabine)
Antiretroviral Medications: Not Recommended in Initial Treatment (1) High rate of virologic failure z Didanosine + tenofovir + NNRTI Inferior antiviral activity z Delavirdine High incidence of toxicities z z Zidovudine + zalcitabine Saquinavir (unboosted) Stavudine + didanosine Ritonavir used as sole PI
Antiretroviral Medications: Not Recommended in Initial Treatment (2) High pill burden/ Dosing inconvenience Lack of data in initial treatment z z z z Amprenavir/ritonavir Indinavir (unboosted) Saquinavir (unboosted) Nelfinavir + saquinavir Tipranavir Enfuvirtide
Antiretroviral Medications: Should not be offered at any time z. Regimens not recommended: y. Monotherapy (except possibly in prevention of perinatal HIV transmission) y. Dual NRTI therapy y. Didanosine + tenofovir + NNRTI y 3 -NRTI regimen of abacavir + tenofovir + lamivudine y 3 -NRTI regimen of didanosine + tenofovir + lamivudine
Antiretroviral Medications: Should not be offered at any time z. Antiretroviral components not recommended: y. Efavirenz in pregnancy and in women with high potential for pregnancy* y. Nevirapine initiation in women with CD 4 >250 cells/mm 3 or men with CD 4 >400 cells/mm 3 * Women with high pregnancy potential are those who are trying to conceive or who are not using effective and consistent contraception.
HIV RTI’s
HIV NNRTI’s
Adverse Effects: PIs z All PIs: y. Hyperlipidemia y. Insulin resistance and diabetes y. Lipodystrophy y. Elevated liver function tests y. Possible increased bleeding risk in hemophiliacs y. Drug-drug interactions
Adverse Effects: PIs z Amprenavir and fosamprenavir - GI intolerance, rash z Atazanavir - hyperbilirubinemia, PR interval prolongation z Indinavir - nephrolithiasis, GI intolerance z Lopinavir/ritonavir - GI intolerance z Nelfinavir - diarrhea z Ritonavir - GI intolerance, hepatitis z Tipranavir – GI intolerance, rash, hyperlipidemia, liver toxicity
HIV Drug Interactions z. Most important with NNRTI’s and PI’s z. Always look up drug interactions every time you prescribe a drug to a patient on HAART Just do it!!!
Adverse reactions Fusion inhibitors z. Enfuvirtide y. Injection site reaction y. Hypersensitivity y. Eosinophilia y. Possible increased pneumonia
HAART failure z. Resistance testing z. Maintain even partial suppression complete cessation associated w/rapid progression to AIDS/death
HIV FOR THE PRIVILEGED Background z Late 1970’s Retroviruses described (HTLV) z 1981: AIDS recognized z Kaposi’s sarcoma, PCP appeared z risk groups identified z 1982: theory of HIV z 1983: HIV-1 identified z blood supply screening z 1983 AZT approved z 1994 PI’s approved z 1994 PACTG-076
HIV: The Reality z. In the US y. As of December 31, 2000: x 774, 467 persons were reported with AIDS x 448, 060 had died xnumber of persons living with AIDS (322, 865) was the highest ever reported x. Approximately 800, 000 --900, 000 persons in the United States are infected with HIV xapproximately 275, 000 of these persons might not know they are infected
HIV: The Reality Worldwide z In 2002, 14, 000 people/day became infected z At end of 2002 y 42 million people worldwide were living with HIV/AIDS. x 38. 6 million adults x 3. 2 million children younger than 15 years y. Approximately 70 % (29. 4 million) live in Sub-Saharan Africa x 9 % of adults between age 15 and 49 x. In 4 African countries, it’s 30%
Ask the Question Offer CTS-counseling, testing and referral to everyone
Perinatally Acquired AIDS Cases by Quarter-Year of Diagnosis* 1985 -1998, United States 200 100 Pediatric AIDS Cases 80 150 60 100 40 50 20 0 Maternal ZDV Use 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 Quarter-Year of Diagnosis 0 Percent Receiving Zidovudine Number of Cases 250
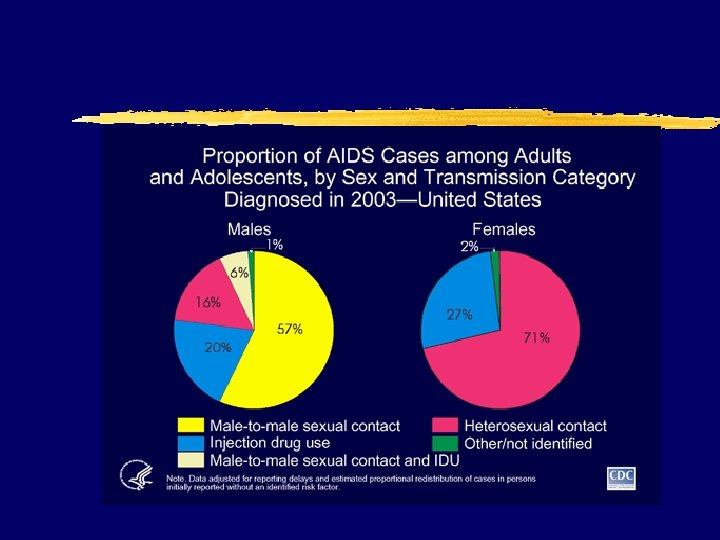
The Epidemiology of HIV/AIDS in Women • Women represent the fastest growing • • segment of the HIV epidemic (35% of all new infections in the United States) The CDC estimates that women will account for half of all infections in the United States by the end of 2002 85% of women with HIV are of childbearing age
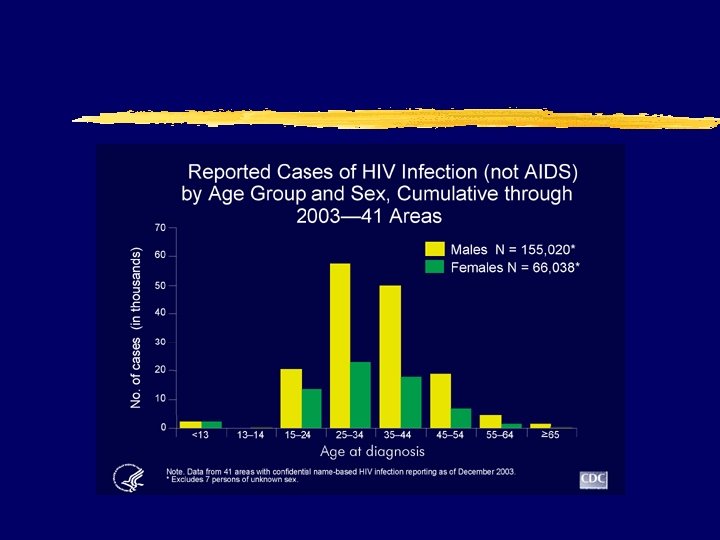
AIDS Cases in Women 13 Years of Age By Age at Diagnosis, Reported in 1998, United States
AIDS in Adolescents and Adults, by Sex and Age at Diagnosis, Reported in 2000, United States 13 -19 Years 20 -24 Years N=342 N=1, 346 Male Female >25 Years N=40, 271
Reported HIV* in Adolescents and Adults, By Sex and Age at Diagnosis, Reported in 2000, United States 13 -19 Years 20 -24 Years >25 Years *From the 34 areas with confidential HIV case surveillance Male Female
Public Health Rationale for Screening • 85% of women with HIV / AIDS are of child-bearing age • It causes significant morbidity and • mortality Tests are acceptable, reliable, and valid
Public Health Rationale for Screening • Interventions are acceptable and of • • proven benefit Benefits of intervention far exceed the cost of screening It upholds women’s right to make informed decisions about testing and to know their HIV status
Guidelines for Screening • Screening should be performed • annually, along with other family planning services Screening should also be performed in response to risk factors, with retesting as needed and agreed to by the patient
Health Care Providers Diagnosing HIV Infection
Who Initiates Testing? In one study …. In this study, 8 providers denied testing to women who specifically asked to be tested
Definition of “Missed Opportunity” Missed Opportunity = An encounter with a health care provider for any reproductive health issue—regardless of risk factors or any contact with any other HCP—by a patient engaging in high-risk behavior where testing was not performed. —Mac. Donald et al. , 1998
Clients should be counseled in Risk Reduction Methods Vaginal and anal sex: • • • Condom use Female condom use Abstinence Reduce # of partners Limit the use of substances prior to sexual activity • Monogamy Oral sex: • Condom use • Dental dam or plastic wrap use • No brushing or flossing prior to performing oral sex • Avoiding ejaculation inside the mouth
Clients should be counseled in Risk Reduction Methods Injection Drug Use • Needle exchange • Cleaning with bleach in absence of new needles • No sharing of works • Don’t inject (other, less risky routes available) Non-Injection Drugs • Reduce intake • Don’t combine drugs • Choose the least risky route • Avoid sexual activity when drunk or high
Contraception and Prevention of HIV 1 Infection z. The only methods which have strong evidence supporting their efficacy to protect against HIV infection are condoms and female condoms z. All clients need to be informed of this fact, and counseled in the consistent and correct usage of these methods
Youth Risk - Understand Youth Risk Behaviors Illinois Female YRBS 1999 38. 1% 26. 4% 16. 9% 42. 9% grades 9 -12 have had intercourse >4 partners sex in past 3 months used alcohol/drugs during most recent episode did not use a condom during the last episode
New drugs
New drugs
New drugs