HIV Update Dr Katharine Bond Dept of GU

HIV Update Dr Katharine Bond Dept of GU Medicine February 2016

HIV Update • HIV in Lincolnshire • HIV testing • HIV risk factors • HIV indicator illnesses • HIV prognosis • HIV treatment • HIV PEP (Relate update)

HIV in Lincolnshire • • ~ 230 registered patients Boston, Lincoln, Grantham, Skegness M>F Mostly UK (NB Boston) Many undisclosed MSM Women diagnosed late Most on antiretroviral therapy Most good adherence
 • Late diagnosis (≈ 55%")
Challenges • Undiagnosed (≈ 17% in UK - 2014) • Late diagnosis (≈ 55% among heterosexuals in UK – 2014) • Stepping up treatment – HIV care continuum target – ‘ 90 -90 -90’ in 2020 (UNAIDS) • HIV prevention • HIV stigma reduction

What is the single most important intervention to tackle the HIV epidemic? HIV TESTING
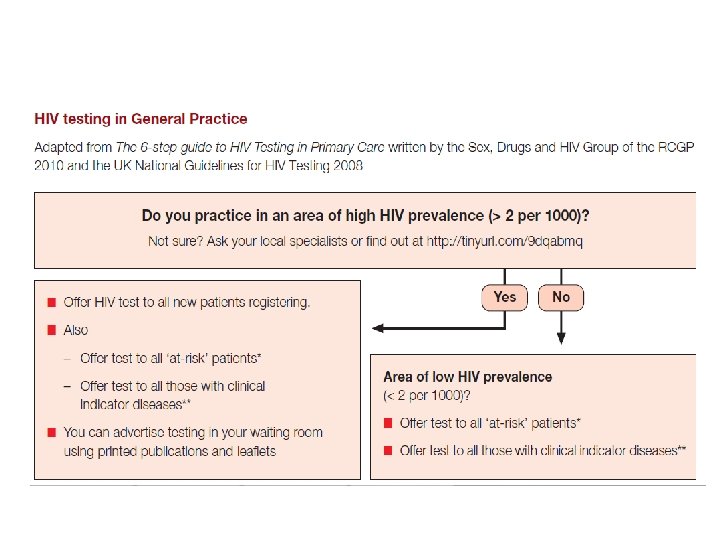

HIV Testing • Who can test? “It should be in the competence of any doctor, midwife, nurse or trained healthcare worker to obtain consent for and conduct an HIV test” • Pre-test counseling Benefits (prognosis, treatment) How will get test results • Disadvantages? • Test 10 ml clotted blood sent to virology marked ‘HIV test’ Point of care test Window period – 4 weeks

Positive test • Inform patient • Refer to GUM – 01522 308 800 • Positive health – 01522 513 999

HIV Prognosis • HIV not currently curable • HIV near to normal life expectancy – Cohort study in US showed life expectancy of a person diagnosed in their 20 s was an additional 51 years • Influencing factors – Stable on treatment – IDU – Late presentation

HIV Treatment • • One tablet vs two tablets OD vs BD Food restrictions Drug interactions Stribild Sleep/shift working Recreational drug use Long term side effects Eviplera Atripla Triumeq

HIV treatment • Recommend for starting combination therapy – 3 or more active drugs – 1 st line NNRTI or PI/r or Integrase inhibitor with 2 NRTIs – CD 4 350 (or universal start? ) – Start earlier with co-morbidities – Treatment as prevention – Aim to supress viral replication

Goal of HAART • The clinical goal – Extend life expectancy and QOL • The virological goal – Reduce HIV viral load to the lowest level possible for as long as possible to prevent disease progression, as well as limiting resistance to ARV drugs • The immunological goal – Restore and preserve immunological function, by maintaining CD 4 cell counts and resisting infection by opportunistic pathogens • The epidemiological goal – To reduce transmission of HIV to others

HIV Treatment • NNRTIs – Efavernz, Nevirapine, Rilpiverine, Etravirine – Atripla, Eviplera • NRTIs – Tenofovir, Abacavir, Lamivudine, Emtricitabine, Zidovudine – Truvada, Kivexa, Combivir • Protease Inhibitors – Darunavir/r, Atazanavir, Lopinavir/r, Tipranavir/r • Intergrase inhibitors – Raltegravir, Elvitegravir, Dolutegravir – Stribild, Triumeq • Fusion inhibitors – T-20 • CCR 5 Inhibitors – Maraviroc
 • Inhibits CYP")
Drug Interactions • Induction and Inhibition of Enzymes – Ritonavir/Cobicistat (Stribild) • Inhibits CYP 3 A and CYP 2 D 6 -mediated metabolism • Inducer of CYP 1 A 4, glucuronosyl transferase (GT), and possibly CYP 2 C 9 and CYP 2 C 19 – Efaverenz • Induces CYP 3 A 4 activity – Nevirapine • Induces CYP 3 A 4 and CYP 2 B 6
 – Beclomethasone – Budesonide")
Common Drug Interactions • Steroids with PI/r or Stribild (cobicistat) – Beclomethasone – Budesonide Fluticasone Dexamethosone Prednisolone • Statins with PI/r or Stribild (cobicistat) – Pravastatin – Simvastatin Lovastatin • Absorption – PPIs with Atazanavir and Rilpiverine (Eviplera) – H 2 antagonists with unboosted Atazanavir or ATZ/r with tenofovir/truvada – H 2 antagonists with Rilpiverine or Atz/r

Common Drug interactions ● ● Antidepressants – Citalopram, Fluoxetine levels increased with ritonavir – Quetiapine Olanzapine PI/r Contraception – ● Methadone – ● COCP POP Implant levels are decreased with HAART Methadone reduction in levels so dose increase Anticoagulation/blood thinning – Warfarin levels may be affected by HAART therefore monitor – Clopidogrel reduces effect with PI/r

• If in doubt – www. hiv-druginteractions. org – University of Liverpool – Or ring us….

HIV Prevention • Risk reduction measures – Condoms provision – Needle and syringe provision – Male circumcision • • STI diagnosis and treatment ART as prevention PEP (Post-exposure Prophylaxis) Pr. EP (Pre-exposure Prophylaxis) • PROUD (UK) and IPERGAY (France) – 86% reduction in HIV acquisition with Truvada

• Assess Risk – >1/1000 recommend – 1/1000 to 1/10, 000 consider • Give within 72 hours • A&E/GUM • 28 days of ARV therapy – Raltegravir/Truvada • Google “BHIVA guidelines PEPSE” – BHIVA 2011 PEPSE guidelines

Risk

Recommendations

Summary • Multidisciplinary approach to HIV testing and prevention – Primary care – Secondary care – Community/outreach • Stepping up HIV treatment – UNAIDS targets to end HIV epidemic • HIV stigma and discrimination – shared responsibility – Crucial intervention to achieve AIDS-free generation

Useful websites • www. bashh. org • www. bhiva. org • https: //www. gov. uk/government/organisations/pu blic-health-england • www. medfash. org. uk • www. clinicaloptions. com • www. aidsmap. com • www. hivinsite. com • www. stif. org. uk
- Slides: 27