HIV dementia and HIVrelated brain impairment HRBI Jeanette
 Jeanette Meadway FRCP Consultant Physician Mildmay Hospital")
HIV dementia and HIV-related brain impairment (HRBI) Jeanette Meadway FRCP Consultant Physician Mildmay Hospital UK Hackney Road, London E 2 7 NA
 u")
What is HIV dementia? u An AIDS-defining illness with WHO definition (ICD 10) u Objectively defined decline in recent memory u Evidence of HIV infection u Exclusion of opportunistic infections, tumours or other brain disorders u Absence of acute brain syndrome (delirium)

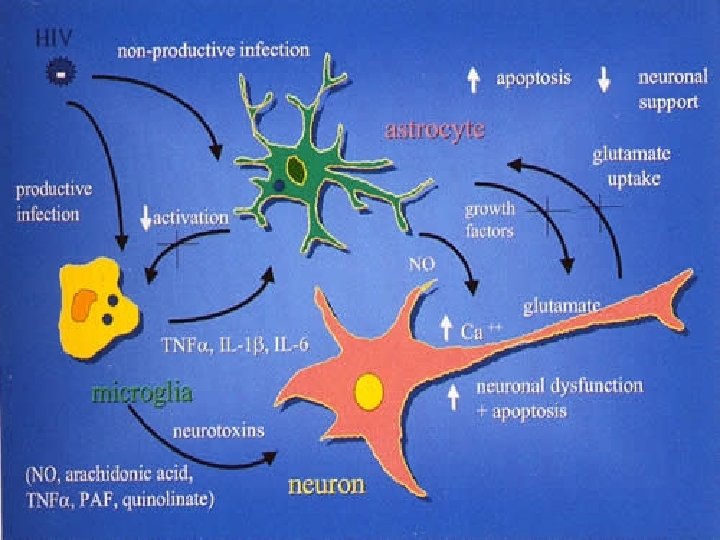
HIV dementia - cause u HIV affecting the brain u No HIV in nerve cells (neurons) u HIV in macrophages and glial cells u Damage due to increased cytokines? u Damage due to toxic effects of HIV envelope protein gp 120? u Damage leads to cell apoptosis (cell death) and structural changes

Diagnosis of HIV dementia u Function: cognitive impairment, motor dysfunction, behavioural changes u HIV disease: usually advanced with low CD 4 (<200), high viral load, no ARV treatment or inadequate ARVs despite deterioration u CT and MRI scans show brain shrinkage and white matter changes

MRI changes Brain shrinkage – rim of CSF inside skull, flattened gyri u White matter changes, most likely to affect frontal lobes as in this scan u (contrast medium in ventricles) u

What is HIV-related brain impairment? Not a diagnosis, an assessment of function which is useful for rehabilitation u Cognitive dysfunction (+- behaviour change and motor dysfunction) due to HIV -related pathology u Includes HIV-related illnesses causing cognitive impairment u Does not include unrelated brain impairment in an HIV+ve person eg due to alcohol u The same diagnoses are not included in HRBI if there is no cognitive dysfunction u

Why this definition of HRBI? u The conditions which lead to behavioural problems, cognitive impairment and motor problems in the context of advanced HIV offer the same challenge for rehabilitation u All are likely to benefit from supervised adherence to ARVs, multidisciplinary approach to social skills and other rehabilitation
 due to JC virus")
HRBI diagnoses u HIV dementia u PML (progressive multifocal leukoencephalopathy) due to JC virus u Cerebral toxoplasmosis u Herpes simplex virus encephalopathy u Cryptococcal meningitis u Cerebral lymphoma u other infections eg TB meningitis

Cerebral toxoplasmosis u u u When CD 4 low toxoplasma causes a cerebral abscess When contrast is injected, there is high uptake around the abscess – a ringenhancing lesion Toxoplasma may cause cognitive impairment

Cryptococcal Meningitis Cryptococcal meningitis is more insidious than bacterial meningitis u Varied neurological changes occur eg cognitive impairment u

PML Progressive – without treatment deteriorating neurology and death u Multifocal – affects separate parts of the brain, as seen with 3 in this scan u Leuko – affects white matter u

HRBI rehab at Mildmay Patients accidentally rehabbed at first u Those improving had full effective ARVs and full multidisciplinary team involvement u Emphasis on self-medication programme, relearning social skills and skills to allow independent activity u Some patients return to live independently u Behavioural improvements allow more appropriate placements for most patients u

A new type of dementia u. A patient restarted on ARVs later deteriorated and died despite fully controlled viral load and good CD 4 u PM showed no HIV in brain, no other infections or tumours, and vacuolated cells u This may be immune reconstitution syndrome u Occurs only in a minority of patients

Summary - HRBI u Cognitive +- behavioural and motor impairment due to HIV disease u Occurs only in advanced HIV u Most improve with full regular ARVs u Improvement with rehab team input u Rehab allows easier placement and improved quality of life u Deterioration on ARVs is uncommon

- Slides: 16