HIV A Causative Agent of AIDS Dr Shubhada

HIV: A Causative Agent of AIDS Dr Shubhada Rahalkar Professor of Zoology Govt. Bilasa Girls P. G. College Bilaspur C. G.

WHAT IS HIV? ? p “Human Immunodeficiency Virus” p. A unique type of virus (a retrovirus) p Invades the helper T cells (CD 4 cells) in the body of the host (defense mechanism of a person) p Threatening a global epidemic. p Preventable, manageable but not curable.

History 40‘s - origin of HIV - genetically derived from simian retroviruses in Equatorial Africa p late 50‘s - first evidence of HIV infection in human p 1981: - first reports on AIDS p

History p First indication in 1981 n p Sudden unexplained outbreak of two very rare diseases from New York & Los Angeles p Koposi Sarcoma p Pneumocystis carinii Pneumonia 1983: - identification of causative agent HIV-1

OTHER NAMES FOR HIV p Former names of the virus include: n Human T cell lymphotrophic virus (HTLV-III) n Human T cell Leukemia Virus HTLV I and HTLV II n Lymphadenopathy associated virus (LAV) n AIDS associated retrovirus (ARV)

WHAT IS AIDS ? ? ? p “Acquired Immunodeficiency Syndrome” p HIV is the virus that causes AIDS p Disease limits the body’s ability to fight infection due to markedly reduced helper T cells. p Patients have a very weak immune system (defense mechanism) p Patients predisposed to multiple opportunistic infections leading to death.
 p Opportunistic infections and malignancies that occur in the absence of severe")
AIDS (definition) p Opportunistic infections and malignancies that occur in the absence of severe immunodeficiency p Persons with positive HIV serology who have a CD 4 lymphocyte count below 200 cells/mc. L or a CD 4 lymphocyte percentage below 14% are considered to have AIDS.
, enveloped virus of the lentivirus subfamily of")
STRUCTURE OF HIV p Icosahedral (20 sided), enveloped virus of the lentivirus subfamily of retroviruses. p p p Two viral strands of RNA found in core surrounded by protein outer coat. Outer envelope contains a lipid matrix within which specific viral glycoproteins are imbedded. These knob-like structures responsible for binding to target cell.

HIV p Integrase p p Viral enevlope. Embedded in the viral envelope is a complex protein - env – glycoprotein, cap gp 120, and a stem gp 41. Shell - p 17 Core or Capsid, - protein p 24(core antigen).
")
Structural Genes p Three main structural genes: n n n Group Specific Antigen (Gag) Envelope (Env) Polymerase (Pol)
 The gag gene determines the core and shell of the")
Group Specific Antigen (Gag) The gag gene determines the core and shell of the virus. p Expressed as precursor protein, p 55 p This precursor is cleaved into p 24, p 17 and p 15 Located in nucelocapsid of virus. p p 17 lies between protein core and envelope. p Two additional p 55 products, p 7 and p 9, are nucleic acid binding proteins closely associated with the RNA. p
 p Envelope (Env) gene codes for envelope proteins gp 160, (gp 120")
Envelope (Env) p Envelope (Env) gene codes for envelope proteins gp 160, (gp 120 and gp 41). n n This polyproteins will eventually be cleaved by proteases to become HIV envelope glycoproteins gp 120 and gp 41. gp 120 forms the 72 knobs which protrude from outer envelope. gp 41 is a transmembrane glycoprotein antigen and attaches to gp 120 and gp 41 both involved with attachment and fusion of HIV to CD 4 antigen on host cells.
 p Polymerase (Pol) codes for p 66 and p 51 subunits of")
Polymerase (Pol) p Polymerase (Pol) codes for p 66 and p 51 subunits of reverse transcriptase and p 31 an endonuclease. n Responsible for conversion of viral RNA into DNA, integration of DNA into host cell DNA and cleavage of protein precursors.

Viral Replication p First step, HIV attaches to susceptible host cell. n Site of attachment is the CD 4 antigen found on a variety of cells p Helper T cells p Macrophages p Monocytes p B cells p Microglial brain cells p Intestinal cells

Early Phase HIV Infection p In early phase HIV infection, initial viruses are M-tropic. Their envelope glycoprotein gp 120 is able to bind to CD 4 molecules and chemokine receptors called CCR 5 found on macrophages

Late phase HIV infection p In late phase HIV infection, most of the viruses are T-tropic, having gp 120 capable of binding to CD 4 and CXCR 4 found on T 4 lymphocytes.

Binding of Virus to CD 4 Receptor
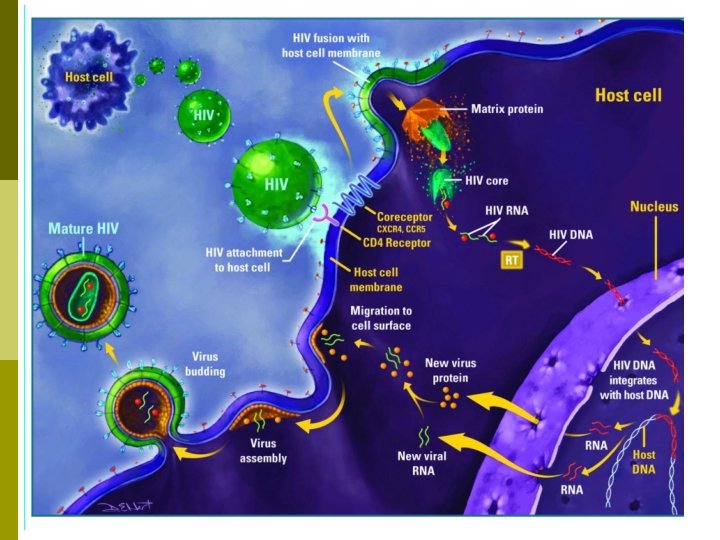

Viral Replication p p p After a period of latency lasting up to 10 years viral replication is triggered and occurs at high rate. CD 4 cell may be destroyed in the process, body attempts to replace lost CD 4 cells, but over the course of many years body is unable to keep the count at a safe level. Destruction of large numbers of CD 4 cause symptoms of HIV to appear with increased susceptibility to opportunistic infections, disease and malignancy.
 Infecting a Tlymphocyte")
HIV (arrows) Infecting a Tlymphocyte

Mode of transmission: p p p Sexual transmission, presence of STD increases likelihood of transmission. Exposure to infected blood or blood products. Use of contaminated clotting factors by hemophiliacs. Sharing contaminated needles (drug users). Transplantation of infected tissues or organs. Mother to fetus, prenatal transmission variable, dependent on viral load and mother’s CD 4 count.

Transmission

Clinical Features of HIV infection p AIDS is the last stage in the wide spectrum of clinical features in HIV infections

Stage 1 - Primary HIV Syndrome Mononucleosis-like, cold or flu-like symptoms may occur 3 to 6 weeks after infection. Lymphadenopathy Rash Fatigue Sore throat Fever Headache Diarrhea Neurologic manifestations. No symptoms may be present

Primary HIV Syndrome Acute HIV Infection - Symptoms are relatively nonspecific. p HIV antibody test often negative but becomes positive within 3 to 6 months, this process is known as seroconversion. p Large amount of HIV in the peripheral blood. p Primary HIV can be diagnosed using viral load titer assay or other tests. p Primary HIV syndrome resolves itself and HIV infected person remains asymptomatic for a prolonged period of p

Stage 2 - Asymptomatic p Lasts for an average of ten years p This stage is free from symptoms p There may be swollen glands p The level of HIV in the blood drops to low levels p HIV antibodies are detectable in the blood

Stage 2 – Asymptomatic: Clinical Latency Period p HIV continues to reproduce, CD 4 count gradually declines from its normal value of 500 -1200 mm 3. p Once CD 4 count drops below 500, HIV infected person at risk for opportunistic infections.

Stage 3 - Symptomatic p Persistent Generalised lymphadinopathy-PLG And p AIDS Related Complex-ARC p The immune system deteriorates p Opportunistic infections and cancers start to appear. n Constitutional symptoms n Common Opportunistic infections

Stage 4 - HIV AIDS p The immune system weakens too much as CD 4 cells decrease below 200.
 p")
Opportunistic Infections associated with AIDS CD 4<500 p Bacterial infections p Tuberculosis (TB) p Herpes Simplex p Herpes Zoster p Hairy leukoplakia p Kaposi’s sarcoma p Candidiasis

Opportunistic Infections associated with AIDS CD 4<200 p Pneumocystis jiroveci p Cryptococcosis p Coccidiodomycosis p Cryptosporidiosis p Toxoplasmosis p Non hodgkin’s lymphoma
")
Opportunistic Infections associated with AIDS CD 4 <50 p Disseminated Mycobacterium avium complex (MAC) infection p Histoplasmosis p Cytomegalovirus (CMV) retinitis p CNS lymphoma p Progressive multifocal leukoencephalopathy p HIV dementia

TB & HIV CO-INFECTION TB is the most common opportunistic infection in HIV and the first cause of mortality in HIV infected patients (1030%) p 10 million patients co-infected in the world. p Immunosuppression induced by HIV modifies the clinical presentation of TB p

Oral Hairy Leukoplakia p Being that HIV reduces immunologic activity, the intra -oral environment is a prime target for chronic secondary infections and inflammatory processes, including OHL, which is due to the Epstein-Barr virus under immunosuppressed conditions
")
Oral Candidiasis (thrush)

Infants with HIV Failure to thrive p Persistent oral candidiasis p Hepatosplenomegaly p Lymphadenopathy p Recurrent diarrhea p Recurrent bacterial infections p Abnormal neurologic findings. p

CD 4 and HIV progression in Patient

CD 4 and HIV progression in Patient

Immunologic Manifestations Early stage slight depression of CD 4 count, few symptoms, temporary. p Window of up to 6 weeks before antibody is detected, by 6 months 95% positive. p During window p 24 antigen present, acute viremia and antigenemia. p

Immunologic Manifestations p Antibodies produced to all major antigens. n n n First antibodies detected produced against gag proteins p 24 and p 55. Followed by antibody to p 51, gp 120 and gp 41 As disease progresses antibody levels decrease.

Immunologic Manifestations p Immune abnormalities associated with increased viral replication. n Decrease in CD 4 cells due to virus budding from cells, fusion of uninfected cells with virally infected cells and apoptosis. n B cells have decreased response to antigens possibly due to blockage of T cell/B cell interaction by binding of viral proteins to CD 4 site. n CD 8 cells initially increase and may remain elevated. n As HIV infection progresses, CD 4 T cells drop resulting in immunosuppression and susceptibility of patient to opportunistic infections. n Death comes due to immuno-incompetence.

Myths about transmission

Testing Options for HIV

Anonymous Testing p p p No name is used Unique identifying number Results issued only to test recipient 23659874515 Anonymous

Laboratory Diagnosis Immunological Tests p Specific tests for HIV infections p

Immunological Tests p Total leucocyte and lymphocyte count- leucopenia & lymphocyte count below 2000/mm 3 p T sub set assays- CD 4+ T cell count less than 200/mm 3, T 4/T 8 ratio is reversed p Platelet count- thrombocytopenia p Raised Ig. G & Ig. A levels p Lymph Node biopsy showing profound abnormalities
 Screening test for HIV Sensitivity >")
Blood Detection Tests HIV enzyme-linked immunosorbent assay (ELISA) Screening test for HIV Sensitivity > 99. 9% Western blot Confirmatory test Speicificity > 99. 9% (when combined with ELIZA) HIV rapid antibody test Screening test for HIV Simple to perform Absolute CD 4 lymphocyte count Predictor of HIV progression Risk of opportunistic infections and AIDS when <200 HIV viral load tests Best test for diagnosis of acute HIV infection Correlates with disease progression and response to HAART

Specific tests for HIV infections p Demonstration of HIV byn Antigen and other component n Viral isolation n Polymerase chain Reaction n Antibody Detection

Antigen and other component p After Single Massive Infectionn n n p Virus antigen detectable after two weeks Antigen p 24 earliest viral marker in blood Ig. M- appears in about 4 -6 weeks, followed by Ig. G After small dose Infectionn n Process may be delayed May coincide with acute or seroconversion stage

Antigen and other component Afterwards free p 24 antigen disappears from circulation & remain absent in long asymptomatic phase p p 24 antigen capture assay ELISA – using anti p 24 antibody as solid phase p

Viral isolation Can be isolated from the peripheral lymphocytes p Co-cultivation of patient lymphocytes with uninfected lymphocytes in the presence of Interlukin-2 p Not suitable as routine diagnostic test p

Polymerase chain Reaction p Most sensitive and specific test p DNA PCR, RNA PCR p Complex and costly

Antibody Detection Simplest and most widely used techniques p Appearance of antibody in bloodp n n n Ig. M- Disappears in 8 -10 weeks Ig. G- remains through out Anti HIV antibody- disappear following clinical AIDS

Antibody Detection 2 -8 weeks to months to appear p Seronegetive infective stage “Window Period” p

Western Blotting p p p Confirmative test HIV proteins separated according to their electrophoretic mobility by Polyacrylamide gel electophoresis Blotted on Nitrocellulose paper Reacted with enzyme conjugated with antihumamglobulin Substrate is added to produce colour

Urine Testing p Urine Western Blot n n n As sensitive as testing blood Safe way to screen for HIV Can cause false positives in certain people at high risk for HIV

Oral Testing p Orasure n n The only FDA approved HIV antibody. As accurate as blood testing Draws blood-derived fluids from the gum tissue. NOT A SALIVA TEST!

Treatment Options

HAART = highly active antiretroviral treatment
 p Nucleoside Reverse Transcriptase inhibitors n p Non-Nucleoside Transcriptase inhibitors n")
Antiretroviral Drugs (HAART) p Nucleoside Reverse Transcriptase inhibitors n p Non-Nucleoside Transcriptase inhibitors n p AZT (Zidovudine) Viramune (Nevirapine) Protease inhibitors n Norvir (Ritonavir)

HEALTH CARE FOLLOW UP OF HIV INFECTED PATIENTS For all HIV-infected individuals: p p p CD 4 counts every 3– 6 months Viral load tests every 3– 6 months and 1 month following a change in therapy PPD (Purified protein derivative test for TB) INH (Isoniazid)for those with positive PPD and normal chest radiograph RPR or VDRL for syphilis Toxoplasma Ig. G serology CMV Ig. G serology Pneumococcal vaccine Influenza vaccine in season Hepatitis B vaccine for those who are HBs. Ab-negative Haemophilus influenzae type b vaccination Papanicolaou smears every 6 months for women

PRIMARY PREVENTION: Five ways to protect yourself? p p p Abstinence Monogamous Relationship Protected Sex Sterile needles New shaving/cutting blades

NON GOVERNMENTAL ORGANIZATIONS NGOs are involved in HIV/AIDS public awareness and in the care and support of persons living with HIV/AIDS. p Also working on education and prevention interventions targeting sex workers, truck drivers, and other high-risk groups. p But reaching less than 5 percent of the vulnerable population. p

WHAT WE CAN DO? ? nine priority areas p We can reduce sexual transmission of HIV. p We can prevent mothers from dying and babies from becoming infected with HIV. p We can ensure that people living with HIV receive treatment. p We can prevent people living with HIV from dying of tuberculosis. p We can protect drug users from becoming infected with HIV. p We can remove punitive laws, policies, practices, stigma and discrimination that p block effective responses to AIDS. p We can stop violence against women and girls. p We can empower young people to protect themselves from HIV. p We can enhance social protection for people affected by HIV.

LIVING WITH HIV/AIDS
- Slides: 67