History of Invention Role of Muscle Stimulator in



: earliest report of a survivor")
 : performing an Inguinal Colostomy for imperforate")
 : Imaging to delineate the abnormality")







 and Galvanic ( Steady")

















- Slides: 34
History of Invention & Role of Muscle Stimulator in Pediatric Surgery M. J. Ansari General & Pediatric Surgeon May 2006
Introduction Electronic Muscle Stimulation is an advanced technique used world wide for Testing , Identification, Repair , Reconstruction, and other purposes on Skeletal Muscles.
Historical Background • The history of Muscle Stimulator is closely related to the history of Anorectoplasty for Imperforated Anus : – Throughout the centuries, doctors have seen and have tried to treat babies born with imperforate anus. Very few patients are described, so most patients are assumed to have died without treatment.
Historical Background – Paulus Aegineta (7 th century ): earliest report of a survivor of surgery. He suggested rupturing an obstructing membrane with the finger or point of a knife and then dilating the tract until healing was complete. This approach was used for many years. – Scultet (1660 ): anal stenosis with dilatation. – Cooke ( 1676 ) : incision and dilatation and advised care of the sphincter muscles – Bell ( 1787 ) : midline perineal incision to find the bowel.
Historical Background – Dubois ( 1783 ) : performing an Inguinal Colostomy for imperforate anus. Other surgeons followed suit, but almost all infants died, so colostomy remained unpopular and only a procedure of last resort. – Amussat ( 1835 ) : Formal Perineal Proctoplasty (ie, mobilization of the bowel through a perineal incision with suturing of it to the skin) this technique gained rapid acceptance – Dieffenbach (1826): described Anal Transposition – Chassaignac( 1856 ): used a probe through a stoma to guide the perineal dissection – Leisrink (1872), Mc. Leod (1880), and Hadra (1884): recommended opening the peritoneum if thebowel was not encountered from below.
Historical Background • Wangensteen and Rice (1930 ) : Imaging to delineate the abnormality • Rhoads, Pipes, Randall, Norris, Brophy, Brayton (1948 -1949) : Single-stage Abdominoperineal Procedures • Stephens (1953) described this procedure and emphasized preservation of the Puborectalis Muscle. This surgery and its modifications were the standard approach until 1980.
Historical Background • In 1980 , the surgical treatment of the anorectal malformations has changed drastically with the introduction of the Posterior Sagittal Anorectoplasty, an approach developed by Prof. Dr. Alberto Peña, also known as Peña's Surgery
Historical Background • This surgical procedure requires a series of technical details to be observed and, a very important one, is the precise location of the external sphincter striated muscle structure, where the rectum is repositioned.
Technique of PSARP / Pull-Through • It entails a midline posterior sagittal incision running from the middle portion of the sacrum to the anterior edge of the external sphincter. • The sphincter mechanism is divided in a midline incision, thereby preserving the nerve fibers and decreasing the amount of postoperative pain. The back of the child's buttocks is opened like a book, and all internal structures are exposed.
Technique of PSARP / Pull-Through • The rectum is then meticulously separated from the genitourinary tract, dissected, and freed enough to reach its normal site without tension. The fistula site is then closed.
Technique of PSARP / Pull-Through • With the use of an electrical muscle stimulator, the limits of the sphincter mechanism are determined and the rectum is placed in its optimal location to achieve the best functional results.
Historical Background • This is achieved with the striated muscles electrical stimulation. • This technique and muscle stimulator has been developed by Prof. Pena since 1980 , reported in 1982 , and has been accepted worldwhile.
Historical Background • At the same period, Iranian pediatric surgeons were doing different techniques, generally without muscle stimulator. • Cut back, Y-V plasty, Transposition , Sacral Approach( Scharlie ), Abdomino-perineal Pullthrough ( Stephens ) were common procedures. • Results were poor for high type malformations. • Mislocation and Incontinence were common.
PSARP with Faradic & Galvanic Current Faradic ( Interrupted ) and Galvanic ( Steady ) current was available on physical therapy devices
PSARP with Faradic & Galvanic Current Stimulation with this device was unsatisfactory and impractical.
Development of Device
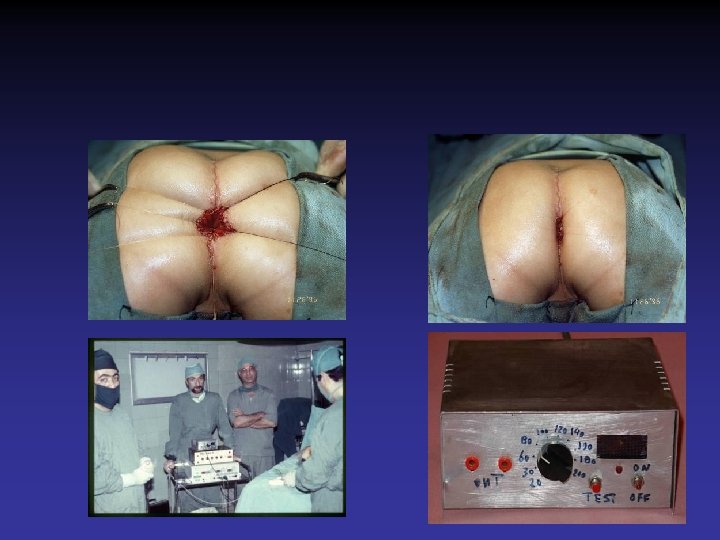
First Operation
First Operation with Muscle Stimulator , 26. 11. 1995 , Ali-Asghar Children Hospital
Post-OP Contraction
1 st Version 2 nd Version
Main Characteristics • The MJA-2 is a muscle stimulator specially developed for this surgical approach. It is a current pulse generator and the pulse amplitude values available cover all the needs, from the initial transcutaneous stimulation to the direct stimulation of the exposed muscles.
Main Characteristics • It is easily installed close to the surgical field as it is light, compact, is powered both by AC current and batteries. An acoustical and LCD indicator informs the electrical current flow through the muscle tissue.
Main Characteristics • • • Current pulse generator Pulse amplitude: selectable values are 1 -200 m. A. Pulse duration: 200 µs Pulse repetition frequency: 50 pps ( HZ ) Pulse shape: rectangular biphasic Maximum stimulation voltage: 300 V Batteries: two, 9 V alkaline. Dimensions: 190 x 150 x 60 mm Weight: 670 g (with batteries)
Applications • Diagnostic • Therapeutic • Follow-up
Applications in Anorectal Malformations • Diagnostic – Anatomy of Muscles – Quality and Force of Muscle Contraction – Anatomical Relation of Muscle to Adjacent Organs – Diagnosis of Mislocatiom
Applications in Anorectal Malformations • Therapeutic – General assessment of surgical anatomy – Identification of ant border of sphincter before incision – Identification of midline of muscles during deepening of incision – Recognition of ant and post border of muscle complex before reconstruction – Assessment after completion of operation
How to Use • Always start with low voltage – 40 -60 m. A over skin – 20 -40 m. A directly over muscle • Moisture skin with saline before contact • Clean blood , clot , and debrie before contact • Repeat test time by time bilateraly
Precautions Never use the device on conscious patient Stimulation with this device is very painful
Precautions Do not contact continuously Continuous contact may result in burn
Precautions Do not connect the probe to device by power on This may result to shortcut and electrical burn.
History of Invention & Role of Muscle Stimulator in Pediatric Surgery M. J. Ansari General & Pediatric Surgeon May 2006