History and Significance of Proper Blood Pressure Measurement

History and Significance of Proper Blood Pressure Measurement

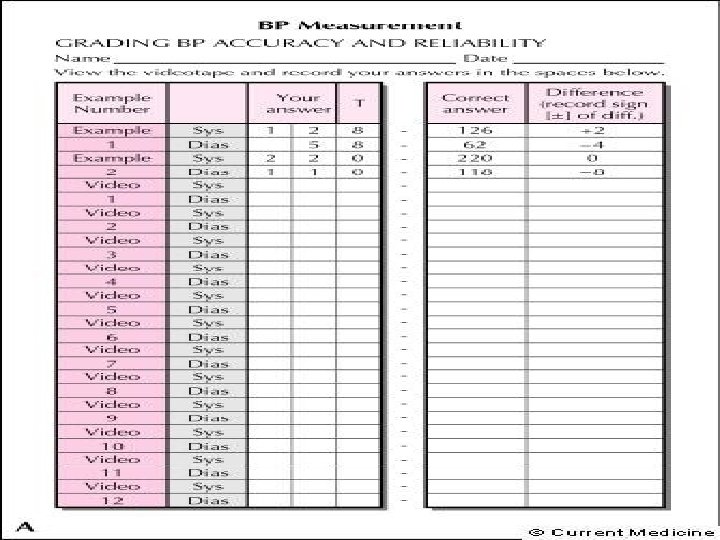
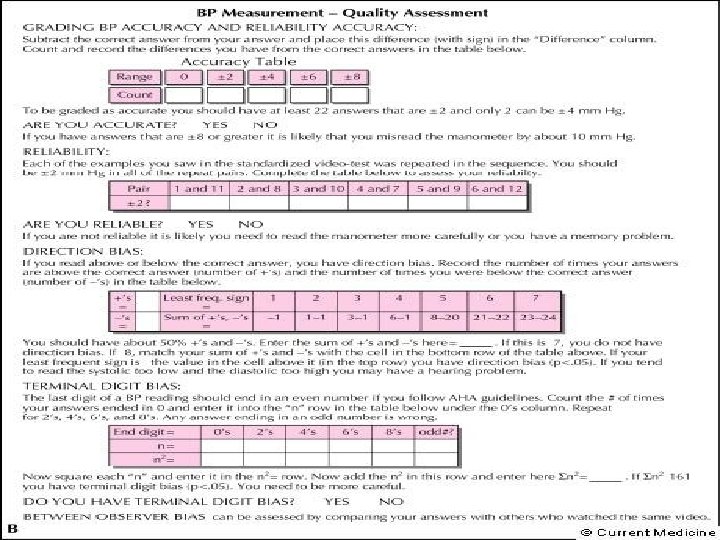
The effect of training on BP observer errors

History of indirect measurement of arterial blood pressure 1733: Stephen Hales first estimated arterial pressure in the horse. 1828: Nearly 100 years later, Poiseuille introduced the mercury manometer indirect method to reliably measure arterial pressure. 1847: Permanent blood pressure recordings, using a mercury manometer and a rotating smoked drum, were developed by Ludwig. 1876: von Basch developed a clinically useful way to measure the systolic pressure by recording the direct pressure necessary to occlude the pulse at the wrist. 1896: Riva-Rocci connected the manometer to an inflatable cuff that encircled the arm. Indeed, Riva-Rocci's report of the steps and pitfalls necessary for accurate and reliable blood pressures includes nearly all of the steps that we know and teach today. This article has recently been reprinted [4]. 1901: von Recklinghausen documented the importance of cuff width, and the standard 12 -cm-wide cuff was adopted for normal arms. 1905: Korotkoff described the sounds heard over a partially occluded artery that even today remain the simplest and most accurate way to measure blood pressure noninvasively in human and animals.

Technique and Equipment

The measurement of BP in the clinic

Skills a good blood pressure observer must have

The equipment

Calibrating the manometer READING YOUR READING ELECTRONIC DEVICE ERROR DIFFERENCE Systolic 1 122 127 +5 Diastolic 1 78 66 -12 Systolic 2 118 119 +1 Diastolic 2 70 64 -6 Systolic 3 116 110 -6 Diastolic 3 68 65 -3 Avg systolic error 5+1 -6/3 = 0 Avg diastolic error (-12 -6 -3)/3 = 7 Comment Device reads 7 mm Hg too low diastolic

Calibrating the manometer

Selecting the most accurate cuff

The cuff and arm circumference

Blood pressure cuff sizes, arm circumference ranges, and bladder widths and lengths CUFF SIZES ARM CIRCUMFERENCE RANGE AT MIDPOINT, cm BLADDER WIDTH, cm BLADDER LENGTH, cm Newborn 6 3 6 Infant 6 15 5 15 Child 16 21 8 21 Small adult 22 26 10 24 Adult

The stethoscope

Cuff Placement and Pulse Detection

Positioning the cuff and arm

Where to listen for the pressure

Steps to determining the maximum inflation level 1. Inflate the cuff to 60 mm Hg, then inflate by 10 - to 15 mm increments until the pulse can no longer be felt. Inflate another 10 to 15 mm Hg and then deflate at 2 mm/s. Note where the pulse reappears as you deflate the cuff. This is the palpated systolic pressure, which is very close to the true intra-arterial systolic pressure. 2. Release the pressure completely 3. Add 30 mm Hg to the pressure; this is the MIL 4. Place the bell of the stethoscope over the palpated brachial pulse in the antecubital fossa, inflate to at least the MIL, release the pressure at a steady 2 mm Hg/s, and record the readings

Where to listen for the blood pressure sounds

Recording the Pressure and the Auscultatory Gap

Recording the pressure and the auscultatory gap

Steps to record the blood pressure reading 1. Inflate the cuff quickly to the MIL 2. Immediately begin to deflate at 2 mm/s 3. Remember the systolic pressure at the point where you hear the first of at least two regular sounds 4. Repeat this number silently to yourself with each heart beat until you detect the diastolic pressure at the point where the last regular sound is heard 5. If K sounds are heard to 0, repeat the reading and note the K 4 or muffling and record all three sounds (eg, 142/66/0) 6. Record the arm, position, cuff used, and the systolic and diastolic pressure 7. Wait 1 min Repeat the reading two more times. Experts recommend discarding the first two readings and averaging the last two.

Which arm should be used?

Testing the mercury manometer • Check the 0. Top of meniscus should rest at the zero mark. Add/remove Hg. • Inflate to 200 mm Hg. Wait 1 minute. Record pressure. If lower than 170 there is a leak. Release pressure. • Note whether Hg rises and falls smoothly • Locate and correct any leaks by replacing appropriate part • Date device to indicate that it was inspected/repaired today

Testing the aneroid manometer • Does the needle rest at zero? (Discard devices with stop pins. ) • Inflate to 200 and check pressure release as for mercury above • Using a Y connector, connect to a mercury device and record the readings at the critical decision points If any reading is off by 4 mm Hg, remove it from service • Place a date on the device that indicates that it was inspected today

Checking the stethoscope • Check ear pieces for obstruction • Check/replace/shorten tubing as needed • Check for a low-frequency detector

References
- Slides: 29