History 1905 Hook ended stripper Keller 1907 Ball

 1907: Ball ended stripper (Babcock)")
History • • • 1905: Hook ended stripper (Keller) 1907: Ball ended stripper (Babcock) 1916: Removal of SFJ collaterals (Homans) 1953: X-ray guided catheterization (Seldinger) 1956: Long stripping (Dodd, Cockett) 1963: Invagination stripping (Van der Stricht) 1998: EVLA, RFA 1999: Fluoroscopic UGS (EVLA + sclerotherapy) 2010: Steam vein sclerosis 2011: Mechano-chemical ablation / Cyanocrylate ablation 2013: Laser assisted foam sclerotherapy

Endovenous Τhermal Αblation Endovenous thermal ablation is an image-guided procedure that uses heat generated by radiofrequency or laser energy to seal of truncal superficial veins, diverting the blood flow to nearby deep veins

Mechanism of Action Thermal energy is transferred from the heating element to vein wall through conduction This results in: • Endothelial destruction • Collagen contraction • Vein lumen diameter shrinkage • Inflammatory response • Fibrotic sealing of the vessel

Histology
 The old system VNUS Inc, California, USA– Covidien, USA")
RF Closure Systems (originally VNUS) The old system VNUS Inc, California, USA– Covidien, USA (not currently trading) – Medtronic, USA
 characteristics • Long (7 cm) conductive heating coil • No energy")
RFA (Closure. FAST) characteristics • Long (7 cm) conductive heating coil • No energy delivery during repositioning • Energy delivery invariable by pullback speed • Fast: 2 -5 minutes (for a 45 cm GSV segment) • No maintenance / adjustments on the generator (intelligent software achieves desired temperature level by increasing automatically the RF power supply)

Laser characteristics � Wavelengths: 810, 940, 980, 1064, 1320, 1470 nm � Type: Diode or Nd: Yag � Continuous or staged drawback � Energy (Joules) � Power (Watts = Joules per second) � Linear Energy Density (J/cm) Linear Lasers Radial Laser Elves Biolitec

Laser Devices
 = power (W) x pull- back velocity of")
Laser characteristics � Total energy (J/cm) = power (W) x pull- back velocity of the catheter (cm/s) � Example : 13 W x 1 cm/5 sec=60 J/cm � A range of 60 to 80 J/cm is safe and produces a successful ablation Johnson C, Mc. Lafferty RB: Endovenous laser ablation of varicose veins: Review of current technologies and clinical outcome. Vascular 15: 250 -254, 2007

Supplies needed for EVLS � � � � Laser energy source Kit containing a laser fiberoptic, marked introducer sheath, and guide wire Percutaneous access set (often contained within the laser kit) Skin marker Sterile drapes Skin cleaner Duplex ultrasound Sterile ultrasound probe cover and gel Tumescent anesthesia 20 -m. L syringe 25 -guage needle Tumescent delivery system Dressing supplies

Set up Procedure room

Procedure � Outpatient � Arrive 1 hr before procedure � 10 mg diazepam � Preoperative DUS – marking the GSV � The leg is then prepped and draped
 �")
Procedure � Access to the GSV without lidocaine percutaneously (in rare cases cutdown) � The microsheath is then advanced into the GSV followed by a 0. 035 -inch guide wire to the level of the SFJ

Procedure � A 0. 035 -inch guide wire is advanced to the level of the SFJ

Procedure � The sheath and the laser fiber are advanced to the SFJ under ultrasound guidance
 440 cc 0. 9% Na. Cl 60 cc 1% Xylocaine")
Procedure � Tumescent (cold) 440 cc 0. 9% Na. Cl 60 cc 1% Xylocaine w/Epinephrine 1: 100, 000 16 cc Na. HCO 3 � Pressure bag (300 mm Hg)

Procedure � Tumescent anesthesia is then administered around the GSV

Procedure � Activation of the laser and withdrawn of the catheter

Procedure � Mini phlebectomies � Elastic bandages

Post-Procedure Instructions � First 48 hours relax, keep leg elevated � Get up every hour and walk around the house � Keep dressings/compression bandages on for 48 hours � Wear compression hose for next 2 weeks � Motrin, 600 mg, t. i. d. , for one week � Zantac, 150 mg, b. i. d. , for one week � Avoid strenuous exercise for two weeks � Return to work in 3 days

Relative Contraindications • Pregnancy / nursing • Liver dysfunction or Lidocain allergy • Severe hypercoagulopathy or hypercoagulation • Obstructed deep venous system • Aneurysmal dilatation of the proximal GSV or SSV • Extreme tortuosity of truncal veins

RFA vs Laser RFA ₊ Avoids pullback variability ₊ Controlled heating at 120 o. C, during each 20 -seconds treatment cycle Laser ₊ Pullback variability, can result in variable and insufficient energy dosing ₊ Uncontrolled heating, occasionally resulting in carbonization vein perforations bruising / heat damage of perivenous tissues
 – 69 pts –")
RFA vs Laser • RCT multicenter (5 US, 1 European) – 69 pts – 87 limbs-GSV – RFA Closure. FASTTM vs. Laser 980 nm (Biolitec. TM), • RF produced significantly less pain, bruising, tenderness, adverse sequelae • RF significant improvements in VCSS and global Qo. L scores • At 1 -month, equalization in most recovery parameters was observed RECOVERY Study – Almeida JI et al, J Vasc Interv Radiol, 2009

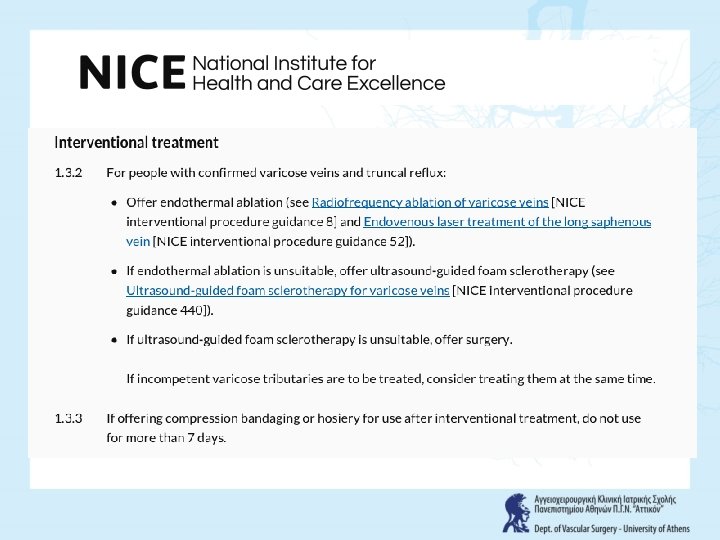
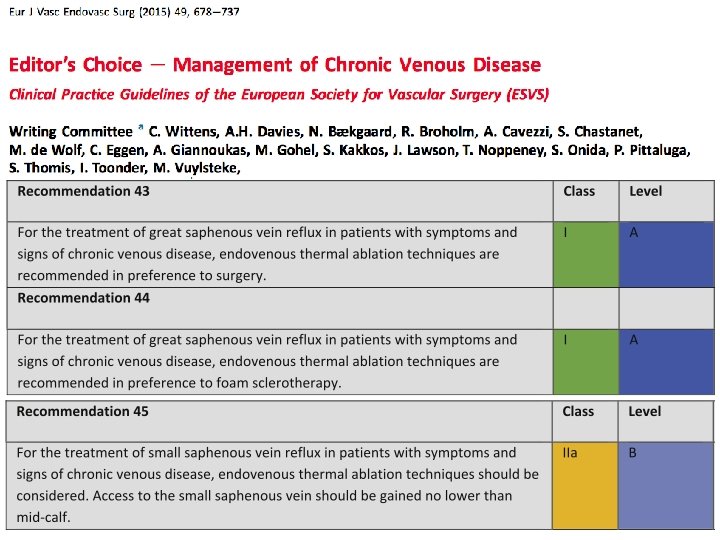
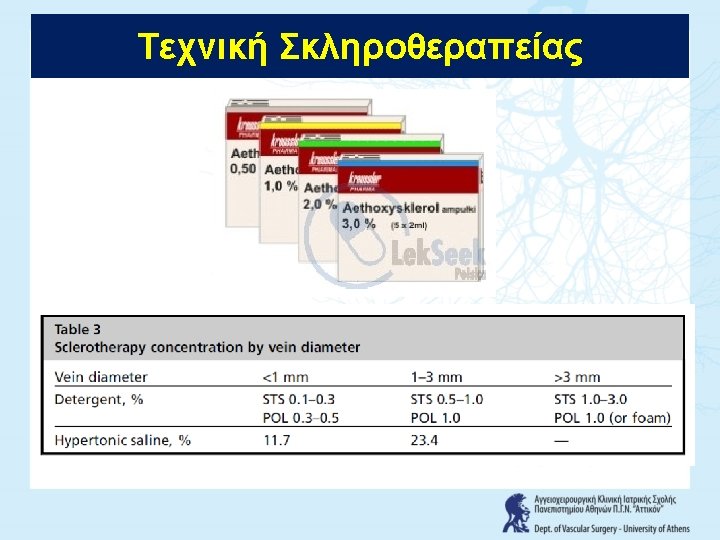
Κατευθυντήριες Οδηγίες European guidelines for sclerotherapy in chronic venous disorders. Rabe E, Breu FX, Cavezzi A, Coleridge Smith P, Frullini A, Gillet JL, Guex JJ, Hamel-Desnos C, Kern P, Partsch B, Ramelet AA, Tessari L, Pannier F; Guideline Group. Phlebology. 2014 Jul; 29(6): 338 -54





- Slides: 39