Historical Perspective on Quality and Registries BDMS Inaugural

Historical Perspective on Quality and Registries BDMS Inaugural ACS Symposium 2019 Joaquin E. Cigarroa, MD Chief of Cardiology, Clinical Chief of KCVI Professor of Medicine Knight Cardiovascular Institute

Disclosures • None

Overview • • • Historical Context Magnitude of Issues Existing Structures Need for Evolution Opportunities
 noted a substantial difference between")
Historical Context: Ignaz Semmelweis • Ignaz Semmelweis (1818 -1865) noted a substantial difference between mortality rates for two obstetric clinics operating within the same institution and introduced official mortality rates • He noted a mortality rate of 9. 09% for physicians and 3. 3% for midwifes and determined the difference was secondary to puerperal fever.

Clinic Mortality Rates

• Action based on observation: introduced policy of handwashing in chlorinated lime before delivering babies reduced the physician staffed delivery mortality rate to 2. 38% • Variation: as new medical students started, an increase in mortality rates was observed secondary to neglecting the standard • Introduced public display of students who failed to wash hands which changed behavior and reduced mortality rates • Skepticism by medical community led to a loss of his job.

Lessons Learned: Key Ingredients for Quality • Ability to quantify outcomes and analyze with formal statistical analysis • Identification of a problem or opportunity for improvement. • Identification of the cause of the difference and determining if the outcome could be improved. • Test hypothesis by knowledge of prior outcome, identification of potential causes, introducing remediation method and remeasuring outcome to assess impact.
 • Born into upper-class English family and struggled against societal")
Florence Nightingale (1820 -1910) • Born into upper-class English family and struggled against societal expectations of an acceptable role of a young woman. • Denounced by her family for choosing the nursing profession • She noted high mortality rate of soldiers transferred to the field hospital during Crimean war. • Recognized as foremost expert in England on hospital construction and operations.

• She reduced risk of death from 32% to 2% by improving food, water, clothing and reducing overcrowding in the wards and introducing improved ventilation. • Collaborated with Dr. William Farr to improved health services by publishing mortality rates of all English hospitals and noted differential mortality rates by number of patients in a room (8/1000 when 8 patients/rm vs 3. 4/1000 when 4 patients/rm).
 • Graduated from Harvard Medical School in 1895 and systematized")
Ernest Codman (1869 -1940) • Graduated from Harvard Medical School in 1895 and systematized his practice of medicine by recording the number of deaths during anesthesia and examined each death. • Reduced mortality rates at En Result Hospital • Introduced End Result Idea: all patients should be followed long enough to determine the outcome of their medical care including whether their life improved. • Advocated for public release of information to assist patients in selecting their provider

Lessons Learned by Early Pioneers • Measurement and statistical analysis are necessary for quality improvement. • Release of data is met with the common criticism that the numbers are wrong and the statistical methods are unsound. • Focus on quality often stirs up vested interests which may lead to personal attacks to discredit the effort and/or person. • Establishing Firm scientific basis for medical practice, standardizing practice and establishing accountability remains a work in progress. • Administrative system requires reform for quality efforts and systems to succeed.

Magnitude of the Problem • Institute of Medicine released two landmark reports (To Err is Human in 1999 and Crossing the Quality Chasm in 2001) which discussed unintended harm and unnecessary deaths: 1. 98, 000 death/year due to medical injuries. 2. Two million patients per year suffer hospital acquired infections. • Study by Dr Martin Makary at Hopkins published in 2016 lists medical errors as third leading cause of death (250, 000/yr).

Magnitude of Problem: Medications • 82% of American adults take at least one medication while 29% take 5 or more. • 700, 000 visits to the ED and 120, 000 admissions are due to ADE annually. • Estimated cost of ADE is 3. 5 billion/yr. • Estimated that 40% of ambulatory costs due to ADE are preventable. • We do not know the statistics for actual medication errors but are estimated to harm 1. 3 million people/yr in US alone.

AIMS • IOM Aims: Safety Effectiveness Patient-centered Timeliness Efficiency Equity • IHI Aims No needless deaths No needless pain No unwanted waits No helplessness No waste No one left out

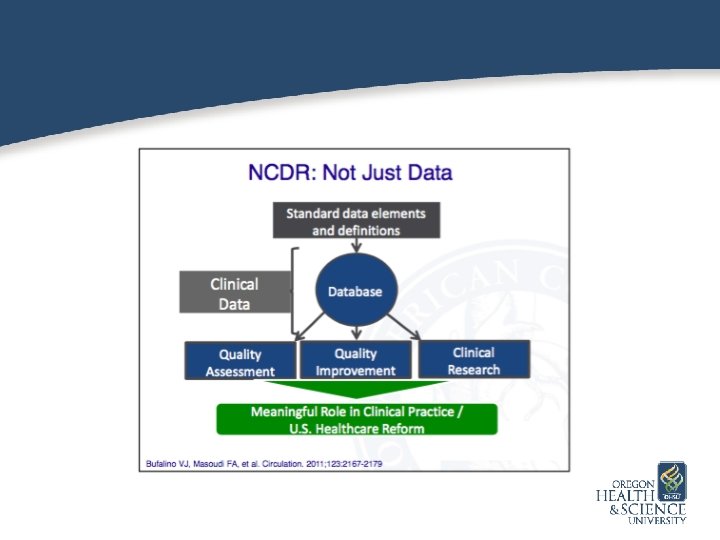
• • • Scientific Evidence ACC/AHA Guidelines Registries Development of Appropriate Use Criteria Development of Value Based Methodology

Existing Structures: Guidelines and Registries

Capacity of Evidence of Inform Practice Maddox et al JACC May 2015

Challenges in Replicated Trials of Primary PCI

Analysis of Action Registry: Medication Errors

NCDR and Medication Errors

TVT: From Clinical Trials to Real World Practice

New Challenges Necessitate New Structures • Transition from individual to team • Patient centric-care for individual patient but set goals for quality improvement based on program level data • Make data visible and use data to prioritize action items and goals • Transition from trying hard despite system to utilizing system and transparency to mitigate variation and improve reliability

Conclusions • Quality structure should improve reliability • Engineer systems of care to improve the consistency of care • Review data and processes consistently in order to celebrate good outcomes and assess gaps to identify opportunities • Create a culture which rewards teamwork and promotes outstanding care and recognition of defects in care.
- Slides: 26