High Risk Newborns https www yenepoya edu in

High Risk Newborns https: //www. yenepoya. edu. in 11/5/2020 7: 24 AM Yenepoya Nursing College (NAME) 1

Leaning objectives • To define High Risk Newborns • Classification of High Risk Newborns • Clinical Manifestations of Diseases in Newborn Period • Basic Principles of Stabilisation & Transport of Sick Neonates 11/5/2020 7: 24 AM (NAME) 2

High Risk Newborns • Definition: Neonates who are at an increased risk morbidity and mortality due to various risk factors • 9 -10% of all newborns require special medical & nursing care and 1 -3% require NICU care • Include premature newborn <34 weeks & ill newborn infants • Requires early identification & close observation by experienced doctors & nurses • Early referral is important to reduce neonatal mortality 11/5/2020 7: 25 AM (NAME) 3

Which Newborns are at High Risk? 1. Demographic social factors • Maternal age <16 or >40 yr • Illicit drug, alcohol, cigarette use • Poverty • Unmarried • Emotional or physical stress

2. Past Medical History of Mother • Genetic disorders • DM • Asymptomatic bacteriuria • Rheumatologic conditions (SLE) • Long term medications

3. Previous Pregnancy • IUD • Neonatal death • IUGR • Congenital malformation • Prematurity, cervical incompetence • Blood group sensitisation, neonatal jaundice • Neonatal thrombocytopenia • Hydrops, inborn errors of metabolism

4. Labour & Delivery • Gestation • AFD • Breech presentation • Meconium stained liquor • Nuchal cord • Caesarean section • Forceps delivery • Poor Apgar score

5. Neonate Factors • Preterm • Post term • SGA, LGA • Born with symptoms & signs of sepsis • Born with congenital malformations

Classification of high risk newborn According to gestational age: • Preterm (born before 37 weeks) • Term (born between 38 and 42 weeks) • Postterm (born after 42 weeks) According to Birth Weight • Low birth weight (LBW) (<2500 g) • Very low birth weight (VLBW) (<1500 g) • Extremely low birth weight (ELBW) (<1000 g)
 ) infant")
According to Birth weight in relation to gestational age. • Appropriate-for-gestational-age (AGA) ) infant • Small-for-date (SFD) or small-for-gestational age (SGA) infant • Intrauterine growth restriction (IUGR) ü Symmetric IUGR: growth restriction in which the weight, length, and head circumference are all affected ü asymmetric IUGR: growth restriction in which the head circumference remains within normal parameters while the birth weight falls below the 10 th percentile • Large-for-gestational-age (LGA) infant
 infant: born before completion of 37 weeks")
according to Gestational age • Premature (preterm) infant: born before completion of 37 weeks of gestation, regardless of birth weight. • Full-term infant: an infant born between the beginning of the 38 weeks and the completion of the 42 weeks of gestation, regardless of birth weight. • Postmature (postterm) infant: an infant born after 42 weeks of gestational age , regardless of birth weight.

• Classification according to mortality • Live birth: birth in which the neonate manifests any heartbeat, breathes, or displays voluntary movement, regardless of gestational age. • Fetal death: death of the fetus after 20 weeks of gestation and before delivery, with absence of any signs of life after birth. • Neonatal death: death that occurs in the first 28 days of life; early neonatal death occurs in the first weeks of life ; late neonatal death occurs at 7 -27 days. • Perinatal mortality: total number of fetal and early neonatal deaths per 1000 live births

According to pathophysiologic problems • Associated with the state of maturity of the infant. • Chemical disturbances. eg: hypoglycemia, hypocalcaemia. • Immature organs and systems. eg hyperbilirubinemia, respiratory distress, hypothermia. • Newborn exposed to HIV/AIDS • Newborn with congenital anomalies

Preterm babies • birth <37 weeks gestation • At higher risk of complications following birth • Complications of Prematurity 1. Early complications: Hypothermia, RDS, apnoea, feeding intolerance, Necrotizing enterocolitis, Infection, IVH , Susceptible to hypovolaemic effects of blood loss. 2. Later complications: Bronchopulmonary dysplasia, Developmental delay and learning disabilities , Cerebral palsy , Retinopathy of prematurity, Behavioural/ psychological problems, Failure to thrive, feeding issues

Post Term Infants • Infants who are born >42 weeks gestation • Having appearance & behaviour of infant of 1 -3 weeks of age • Significantly increased risk of mortality when delivery is delayed >=3 weeks beyond term • Problems of post term infants: Intrauterine Asphyxia, Meconium Aspiration

SGA newborn • LBW< 2500 g, can be due to prematurity, or IUGR, or both • Associated problems of SGA babies: 1. Intra uterine death, 2. Perinatal asphyxia, 3. Hypoglycaemia , 4. Polycythemia – hyperviscosity , 5. Hypothermia

Large for Gestational Age • Also known as macrosomia with BW>4 kg • Neonatal mortality rates decreases with increasing birth weight upto 4 kg, after which mortality increases • Causes for LGA-Post term infants , Maternal diabetes during pregnancy , Fetal disorder of transposition of the great vessels. , Genetic factors , Obesity , Multiparous mother

Complications of LGA Newborns • Risk for birth injuries (e. g. , clavicle fracture, brachial plexus injury, cephalohaematomas) • May need caesarean birth • Hypoglycemia • Polycythemia (HCT>65%) • RDS • Congenital defects (congenital heart defects, tracheoesophageal fistula & CNS anomalies)

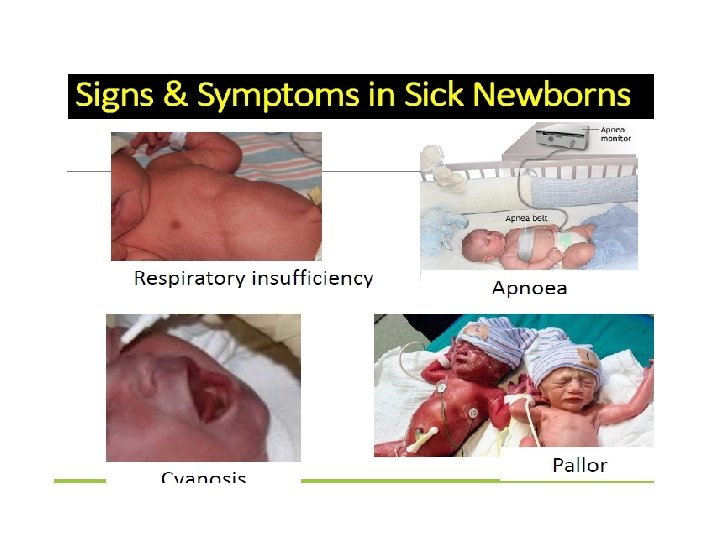
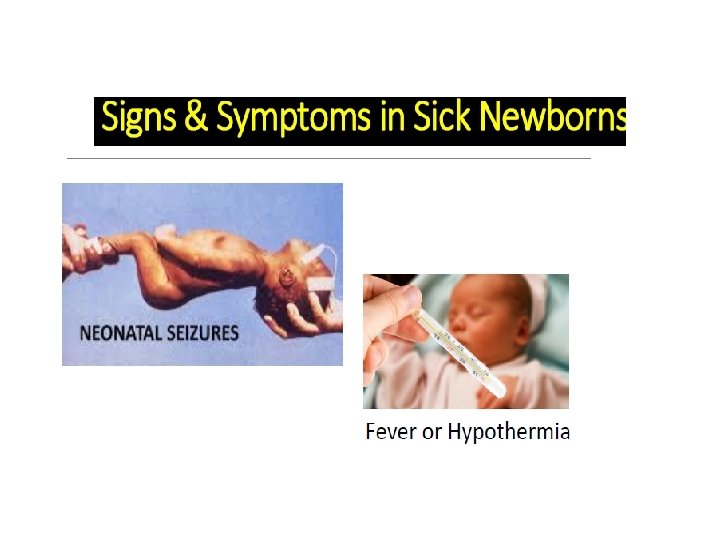
Clinical Manifestations of Diseases in Newborn Period Diseases that affect the newborn may originate: in utero, during birth, or in the immediate postnatal period • Recognition of diseases in newborn infants depends on knowledge of the diseases and evaluation of a limited number of non-specific clinical signs & symptoms


MANAGEMENT OF HIGH RISK NEWBORN NICU for high risk neonates • When the birth of a high risk neonate is expected the mother should be delivered in an institution where Level-III perinatal care is available. • Infant transported to the nursery in a transport incubator or radiant warmer along with a trained personnel • When the birth of high risk neonate had not been expected, the newborn must be transported to facility where optimal care can be provided

Communication • Good communication aids proper pre-transfer stabilization, coordination, timing of transfer, & preparedness of receiving hospital • Involves teamwork: referring doctor, escorting team, neonatologist/ paediatrician +/- paediatric surgeon, ED staff of receiving hospital • Provide detailed info about patient & relevant transfer details

Assessment and monitoring of high risk newborn • All the team members must assess the changes in the baby’s condition promptly and provide appropriate care. • One nurse is responsible to care only one acutely ill newborn • Once the baby is recovered shift to intermediate care where one nurse can take care of 3 to 4 babies • Maintenanace of controlled thermal environment • Monitoring HR, respiratory rate and BP • Collection of specimens

General nursing Management • • Maintenanace of body temperature Prevention of infection and INJURY Feeding Fluid therapy Drugs- as required Documentation Communication




- Slides: 30