High chloride containing fluids are a problem Quen

High chloride containing fluids are a problem Quen Mok Great Ormond Street Hospital

Chloride: Queen of electrolytes?

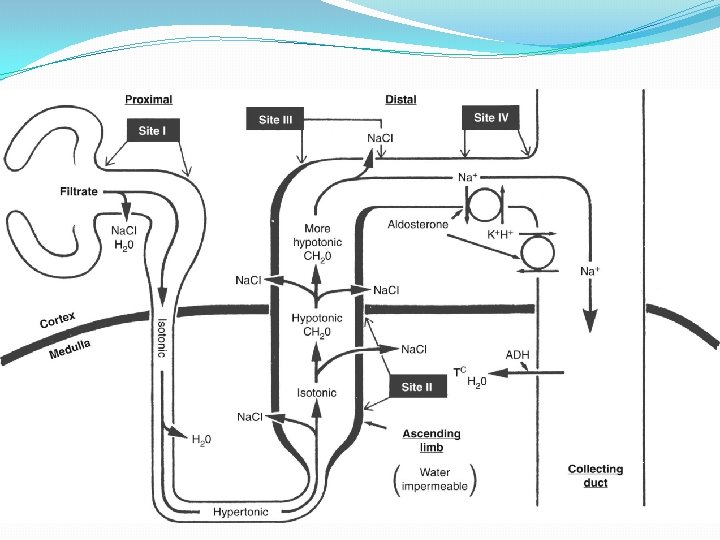
Renal handling of Chloride �Predominantly excreted by the kidneys � 99% reabsorbed � 60% passively in proximal tubules following active sodium transport � 15 -25% in loop of Henle � 5% in distal tubule - aldosterone

Renal excretion of Chloride

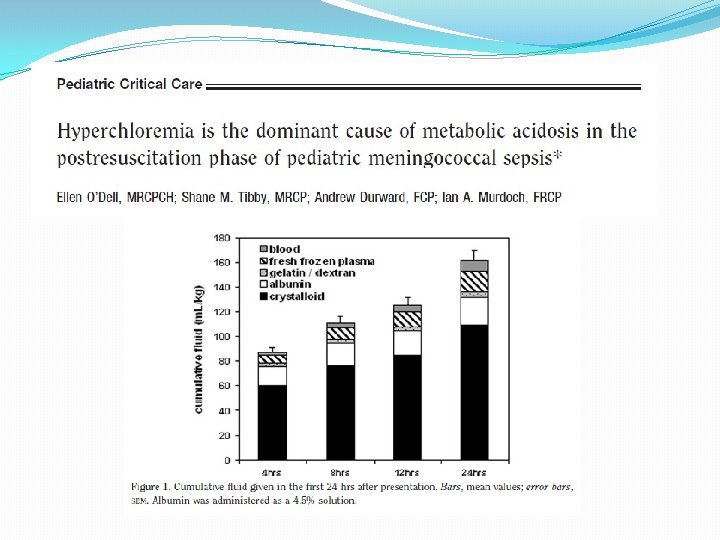
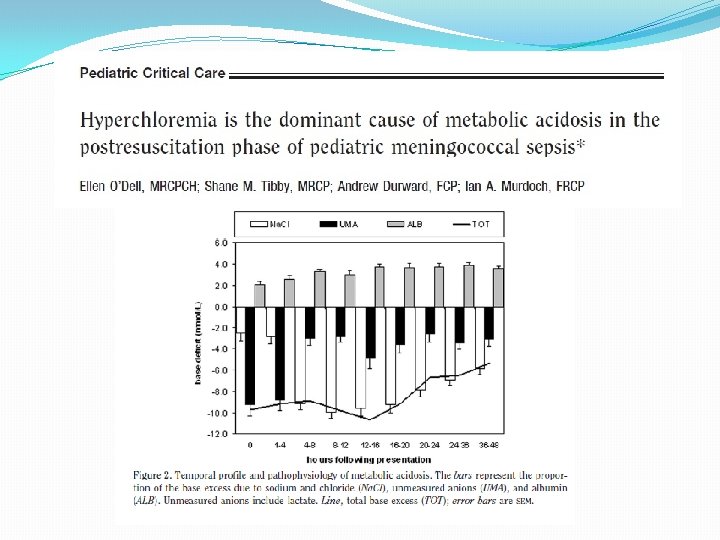
Hyperchloremic acidosis �So why is hyperchloremia a problem? �Immune activation and pro-inflammatory �Renal dysfunction – renal vasoconstriction and decreased GFR �Clotting abnormalities �Increased mortality
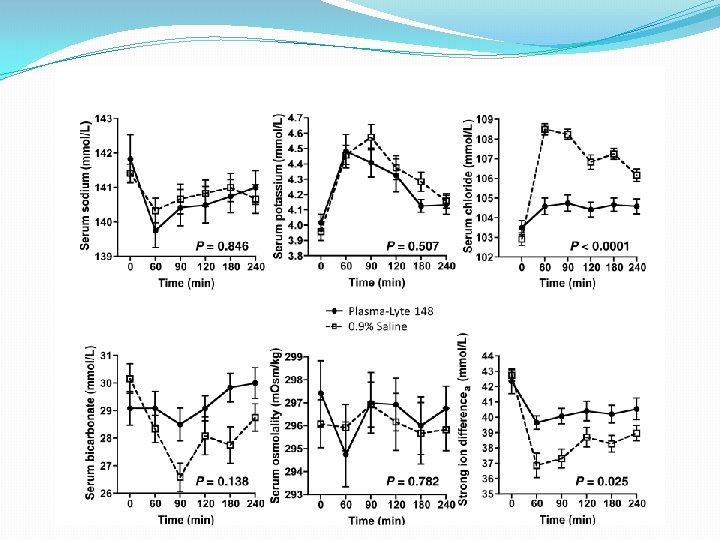

Hyperchloremic acidosis Infusions of 0. 9% Saline and Plasmalyte on renal blood flow velocity and renal cortical tissue perfusion Chowdhury AH et al Ann Surg 2012; 256: 18 -24

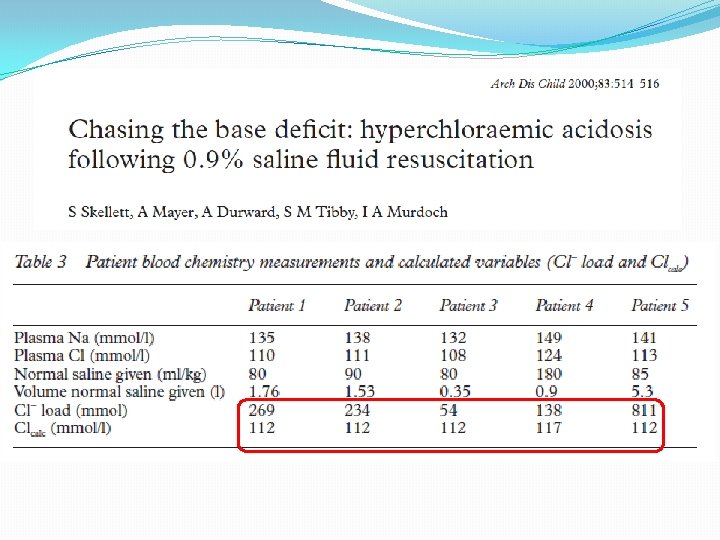
Chloride rich solutions �Serum chloride 97 -110 mmol/l � 0. 9% saline – 154 mmol/l chloride � 4. 5% Albumin – up to 160 mmol/l chloride �Hence large volumes potentiate metabolic acidosis regardless of the underlying disease process �Often unrecognised and poorly managed �Misdiagnosed as inadequate perfusion �Base deficit used as a key prognostic variable in paediatric mortality risk score
 – difference between")
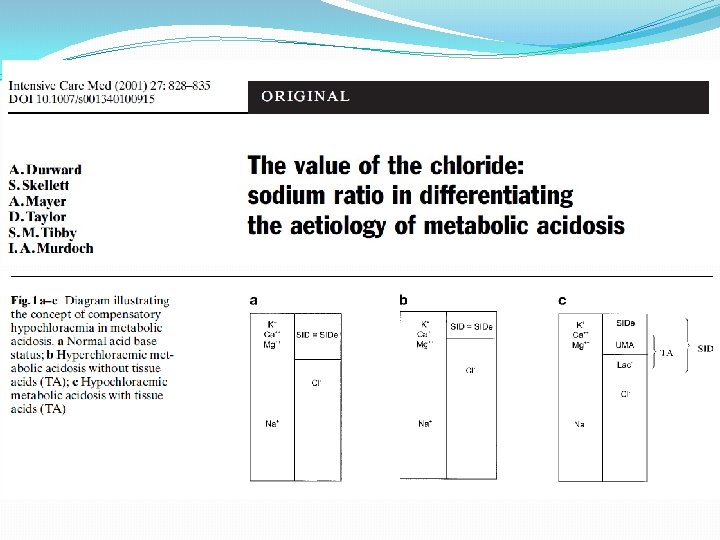
Stewart approach �Plasma p. H determined by �Strong ion difference (SID) – difference between strong cations (Na, K, Ca, Mg) and strong anions (Cl and lactate) �Pa. CO 2 �Weak acids (Atot) – mainly albumin and inorganic phosphate �Decreased SID has acidifying effect as changes degree of water dissociation into hydrogen ions

Strong ion difference

Electrolyte composition of common IV fluids Cations Anions Osm Na K Ca Mg Cl Acetate Plasma 135 -145 3. 5 -5. 0 4. 4 -5. 2 1. 6 -2. 4 98 -106 Bicarbonate 21 -30 Na. Cl 154 Ringer lactate 130 Ringer acetate 0 154 4. 0 3. 0 109 130 4. 0 Hartmann ’s 131 5. 0 4. 0 Plasmalyte 140 5. 0 0 2. 0 110 98 Gluconate 273 30 277 29 27 mosmol /l 280 -300 28 111 3. 0 Lactate 278 23 295
 �Lower if potassium")
Dialysis Replacement solutions �All contain high chloride levels (108 -125 mmol/l) �Lower if potassium free bicarbonate solutions �Serum electrolytes equilibrate with replacement fluid

Conclusions �Chloride is a major strong anion in the extracellular fluid space �Hyperchloremic acidosis causes renal vasoconstriction and decreased GFR �May be misinterpreted as inadequate tissue perfusion �Consider use of balanced solutions �Serum electrolyte equilibrate with dialysis replacement fluid

Not the case with chloride…….
- Slides: 19