HERPESVRUS HUMANOS Os herpesvrus humanos conhecidos TIPO SINONIMIA

 TIPO SINONIMIA Sub-Família PATOFISIOLOGIA HHV-1 Vírus do Herpes simples (HSV-1)")




 SINAIS CLÍNICOS")
")
")
")



")

 Rápido: esfregaços de células e exame por")













 uso somente tópico - Aciclovir e análogos (guanosina acíclica)")


 - vírus")




 - Ig. M específica anti-ag capsídeo")





![Treatment includes dose-adjusted EPOCH with Rituxan (RITUXIMAB). [12] The effects of the CHEMOTHERAPY, as](https://slidetodoc.com/presentation_image_h/73bc532c6a3f88844a5d34de06b98296/image-50.jpg "Treatment includes dose-adjusted EPOCH with Rituxan (RITUXIMAB). [12] The effects of the CHEMOTHERAPY, as")
 – Roseolovírus (vírus da")
 - é um betaherpesvírus; HHV-5, um só sorotipo - infecção muito prevalente;")
 TRANSMISSÃO E EPIDEMIOLOGIA: - Acs em ~80% adultos - eliminação de vírus")







 - MI Paul Bunnel - negativa")





 1. Teste para antigenemia (CMV) - Antígenos do CMV detectados na")

 + anticorpo específico marcado com FITC")
")

 A apresentação clássica da roséola ocorre em crianças de 9")




 • Tumor associado à ocorrência do Sarcoma de Kaposi e")

- Slides: 82
HERPESVÍRUS HUMANOS
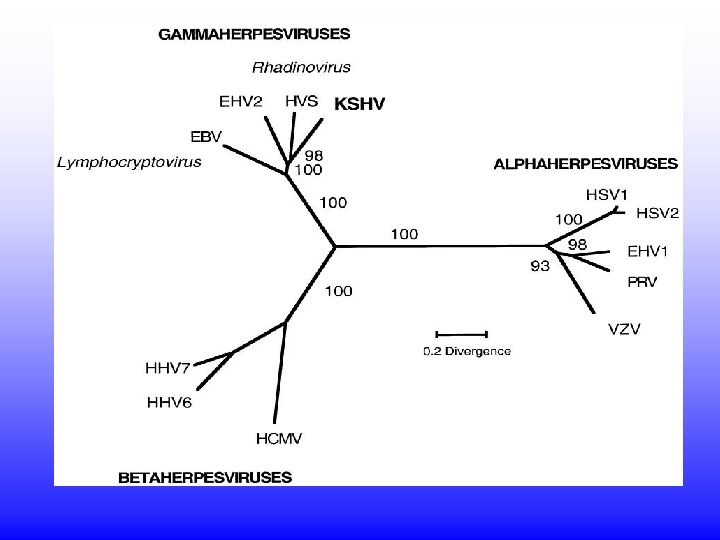
Os herpesvírus humanos (conhecidos) TIPO SINONIMIA Sub-Família PATOFISIOLOGIA HHV-1 Vírus do Herpes simples (HSV-1) Alfa (α) Herpes oral ou genital (predomina orofacial) HHV-2 Vírus do Herpes simples 2 (HSV-2) Alfa (α) Herpes oral ou genital (predomina genital) HHV-3 Vírus varicela-zoster Alfa (α) Varicela ou catapora, herpes zoster HHV-4 Epstein-Barr virus (EBV), lymphocryptovirus γ (Gamma) Mononucleose infecciosa, Linfoma de Burkitt, Linfoma do CNS em pacientes com AIDS, sindrome linfoproliferativa pós-transplante (PTLD), carcinoma nasofarínfgeo HHV-5 Cytomegalovirus (CMV) β (Beta) Síndrome ~ à mononucleose infecciosa, retinite, doença de inclusão citomegálica. HHV 6, 7 Roseolovirus β Sexta doença (roséola infantum ou exantema súbito) HHV-8 Herpesvírus associado ao sarcoma de Kaposi (KSHV), um tipo de rhadinovírus γ (Gamma) Sarcoma de Kaposi e outros tumores
Família Herpesviridae • Subfamília: • Alfaherpesvirinae – Simplexvirus (Herpes simples humano, ou HSV, ou HHV-1 e HHV-2 (human herpesvirus type 1 or 2) – Varicellovirus (vírus da varicela, ou catapora, ou varicela -zoster, VZV (varicella-zoster virus) ou HHV-3 (human herpesvirus type 3)
Vírus do Herpes Simples Humano - são alfaherpesvírus, latencia em neurônios - envelopados - Capsídeo icosaédrico, 162 capsômeros - codifica cerca de 70 polipeptídeos - tipos 1 e 2 muito semelhantes - multiplicação intranuclear Ver structure em: F: ENSINOAnimaçõesHSVzipped exe
Latência Infecção Primária Gânglio Nervoso Genoma celular Terminações nervosas Núcleo Mini-cromossomo – Genoma Viral+ Histonas
Reativação Com ou sem lesões neurônios Pele/ mucosas Gânglio Nervoso regional
• Herpes humanos tipos 1 e 2 (HHV-1 e 2) SINAIS CLÍNICOS
HSV tipo 1; HHV-1: Doenças associadas: Herpes labial Queratite Estomatites (Aftas)
Herpes labial (HSV tipo 1; HHV-1)
Herpes labial (HSV tipo 1; HHV-1)
Lesões herpéticas
Herpes
Herpes neonatal Lesões cutâneas Encefalites
Herpes genital (HSV tipo 2; HHV-2)
Herpes genital
Herpes DIAGNÓSTICO Clínico Diagnóstico laboratorial clássico: 1) Rápido: esfregaços de células e exame por imunofluorescência 2) Isolamento de vírus: fluido vesicular, suabes orais, nasais, conjuntivais, tecidos de abortos, fragmentos de encéfalo, LCR inoculação em células Vero, HEP e muitas outras efeito citopático (ECP) característico em 1 -3 dias
Genoma viral Diagnóstico atual: PCR para detecção de fragmentos de genoma viral 1 Eletroforese 1100 pb Região alvo PCR Desenho de primers (18 -20 nts) 1100 pb 2 3 1: positivo 2: marcador 3: negativo
Diagnóstico sorológico Soroneutralização: em laboratórios especializados Enzyme linked immunosorbent assay – ELISA Permite inclusive diferenciar infecções por HSV-1 ou HSV-2 Positivos Negativos
Família Herpesviridae • Subfamília: • Alfaherpesvirinae – Simplexvirus (Herpes simples humano, ou HSV, ou HHV-1 e 2) – Varicellovirus (vírus da varicela, ou catapora, ou varicela-zoster, VZV, ou HHV-3)
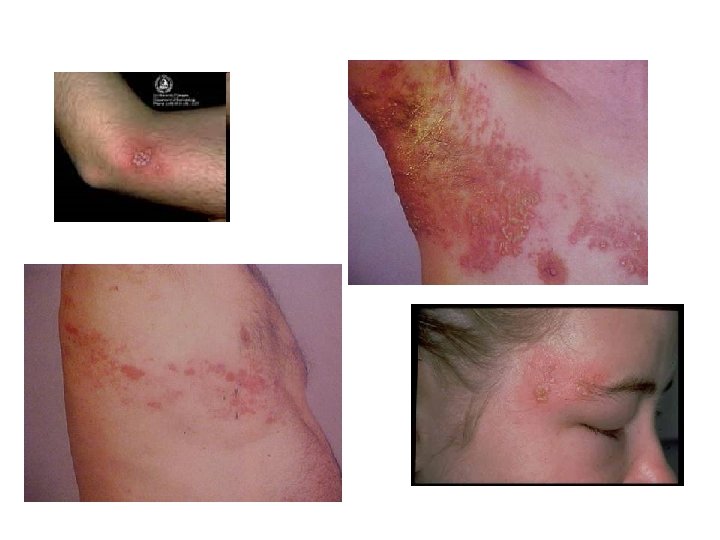
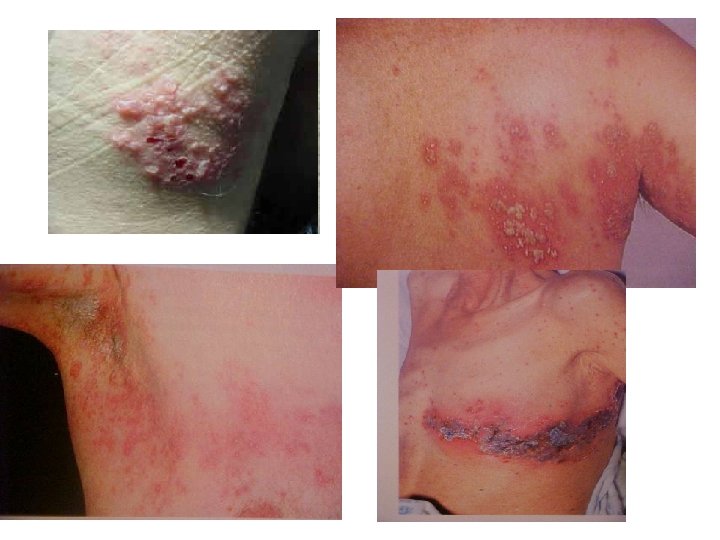
VARICELA ou “Catapora” p. i. 14 -20 DIAS EVOLUÇÃO RÁPIDA ALTAMENTE CONTAGIOSA LESÕES EM DIFERENTES ESTÁGIOS
VARICELA Lesões
VARICELA
Zoster
Zoster
VARICELA DIAGNÓSTICO: Geralmente clínico em imunocompetentes No laboratório: diagn. rápido em células da lesão (início): IF, IPX células gigantes leucopenia Isolamento em células: VERO, BHK, RK 13 1árias de rim de macaco ECP em 2 a 14 dias
HERPES Tratamento - Idoxuridina (IDU) uso somente tópico - Aciclovir e análogos (guanosina acíclica) ação sobre a timidina quinase viral - a longo prazo - efeito na recorrência - ocular : idoxuridina, trifluridina (tópicos) (resistentes: ácido fosfonofórmico) NENHUMA DROGA EVITA COMPLETAMENTE RECORRÊNCIAS ! NENHUMA DROGA AGE SOBRE A LATÊNCIA !
Família Herpesviridae • Subfamília: Gammaherpesvirinae – Lymphocryptovirus (vírus Epstein-Barr, EBV, ou herpesvírus humano tipo 4 (HHV-4) - Latência em células linfóides
MONONUCLEOSE INFECCIOSA “Clássica” ou “Mononucleose Paul-Bunnel positiva” Definição: - Causada pelo vírus Epstein-Barr (EBV 1 e 2) gamaherpesvírus (gênero lymphocryptovirus); - HHV 4 A mononucleose = São linfócitos T atípicos, maiores, com citoplasma vacuolizado e núcleo deformado e lobulado.
Mononucleose infecciosa Transmissão / Patogenia - transmissão por saliva (90% adultos +) - vírus intermitente na saliva - 10 -5 a 10 -6 linfócitos infectados - orofaringe => linf. B => Linf T reagem => muitas cópias do genoma no citoplasma; poucas integradas no genoma.
Mononucleose infecciosa
Mononucleose Infecciosa
Mononucleose Infecciosa Células alvo = Linfócitos B não sensibilizados - 10 genes (EBNA 1 -6, LMP 1, 2 a e 2 b, EBER 1 e 2) mantém a infecção latente em células linfóides - Linfóc. B -> estimulados a proliferar continuamente - podem se multiplicar seriadamente e dar origem a linhagens linfoblastóides - disseminação esporádica pela saliva - linfócitos infectados se comportam como linfócitos sensibilizados com Ag: secretam proteínas, Igs, sofrem trocas de classe
Mononucleose infecciosa Latência em três formas: I e II = antígenos nucleares expressos: EBNA 1; LMP 1, 2 a e 2 b III = os 6 EBNA são expressos EBNA 1: único expresso em todas as formas sem ele não há latência
Mononucleose infecciosa Diagnóstico: - Paul Bunnel (Ac heterófilos) - Ig. M específica anti-ag capsídeo viral (ACV) - Ig. G anti- ACV em elevação - anti-EBNA: 3 -4 semanas p. i. e persiste por toda a vida
Exemplos de placas de ELISAs Revelada com OPD Cor= + Sem cor= Mais cor = mais positivo
Mononucleose infecciosa - EBV Associação com cânceres linfóides: Linfoma de Burkitt em crianças africanas Carcinoma nasofaríngeo (CNF) => (China) Resto do mundo: CNF < 1/ 100 000 China: 15 a 30/ 100 000 Carcinoma de timo nos EUA Hodgkins: EBV presente em 50% dos tumores
Linfoma de Burkitt
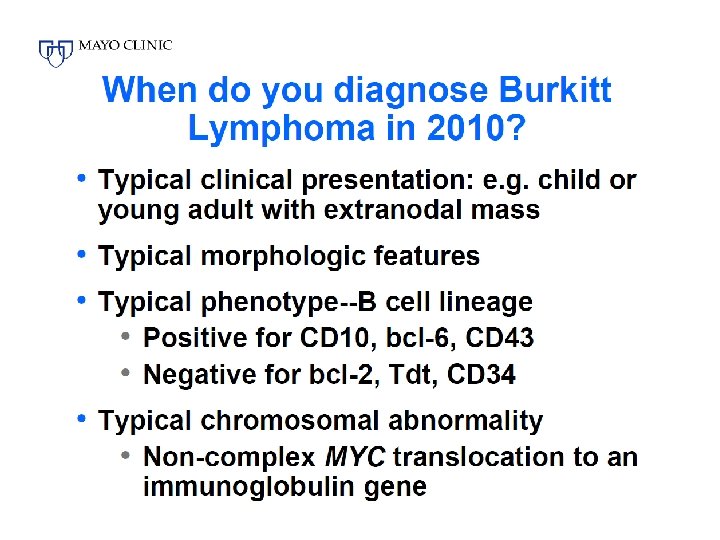
Linfoma de Burkitt: três formas Currently Burkitt's lymphoma can be divided into three main clinical variants: the endemic, the sporadic and the immunodeficiency-associated variants. The endemic variant occurs in equatorial Africa. It is the most common malignancy of children in this area. Children affected with the disease often also had chronic malaria, which is believed to have reduced resistance to EBV, allowing it to take hold. The disease characteristically involves the jaw or other facial bone, distal ileum, cecum, ovaries, kidney or the breast. The sporadic type of Burkitt lymphoma (also known as "non-African") is another form of non. Hodgkin lymphoma found outside of Africa. The tumor cells have a similar appearance to the cancer cells of classical African or endemic Burkitt lymphoma. Again it is believed that impaired immunity provides an opening for development of the Epstein Barr virus. Non-Hodgkin lymphoma, which includes Burkitt's, accounts for 30 -50% of childhood lymphoma. The jaw is less commonly involved, compared to the endemic variant. The íleo-cecal region is the common site of involvement. Immunodeficiency-associated Burkitt lymphoma is usually associated with HIV infection[3] or occurs in the setting of post-transplant patients who are taking immunosuppressive drugs. Burkitt lymphoma can be one of the diseases associated with the initial manifestation of AIDS. By MORPHOLOGY(i. e. microscopic appearance) or immunophenotype, it is almost impossible to differentiate these three clinical variants. Immunodeficiency-associated Burkitt lymphoma may demonstrate more plasmacytic appearance or more pleomorphism, but these features are not specific. Of all cancers involving the same class of blood cell, 2% of cases are Burkitt's lymphoma.
The tumor consists of sheets of a monotonous (i. e. similar in size and morphology) population of medium size lymphoid cells with high proliferative activity and apoptotic activity. The "starry sky" appearance seen[5] under low power is due to scattered tingible body-laden macrophages (macrophages containing dead body of apoptotic tumor cells). The old descriptive term of "small non-cleaved cell" is misleading. The tumor cells are mostly medium in size (i. e. tumor nuclei size similar to that of histiocytes or endothelial cells. "Small non-cleaved cells" are compared to "large non-cleaved cells" of normal germinal center lymphocytes. Tumor cells possess small amount of basophilic cytoplasm. The cellular outline usually appears squared off. Immunohistochemistry The tumor cells in Burkitt lymphoma generally strongly express markers of B cell differentiation (CD 20, CD 22, CD 19) as well as CD 10, and BCL 6. The tumour cells are generally negative for BCL 2 and Td. T. The high mitotic activity of Burkitt lymphoma is confirmed by nearly 100% of the cells staining positive for Ki 67. Genetics All types of Burkitt's lymphoma are characterized by disregulation of the c-myc gene by one of three chromosomal translocations. [7] This gene is found at 8 q 24. The most common variant is t(8; 14)(q 24; q 32), which accounts for approximately 85%[7] of cases. This involves c-myc and IGH@. A variant of this, a three-way translocation, t(8; 14; 18), has also been identified. [8] A rare variant is at t(2; 8)(p 12; q 24). [9] This involves IGK@ and c-myc. Another rare variant is t(8; 22)(q 24; q 11). [9] This involves IGL@ and c-myc. Combined, the two less-common translocations, t(2; 8)(p 12; q 24) and t(8; 22)(q 24; q 11), account for the remaining 15% of cases not due to the t(8; 14)(q 24; q 32) translocation. [7]
Treatment includes dose-adjusted EPOCH with Rituxan (RITUXIMAB). [12] The effects of the CHEMOTHERAPY, as with all cancers, depend on the time of diagnosis. With faster growing cancers, such as Burkitt's, the cancer actually responds faster than with slower growing cancers. This rapid response to chemotherapy can be hazardous to the patient, as a phenomenon called “tumor lysis syndrome" could occur. Close monitoring of the patient and adequate hydration is essential during the process. Chemotherapy Cyclophosphamide Doxorubicin Vincristine Methotrextate cytarabine ifosfamide etoposide rituximab Other treatments are immunotherapy, bone marrow transplants, stem cell transplant, surgery to remove the tumor and radiotherapy. Prognosis Treatment with dose-adjusted EPOCH with Rituxan (rituximab) has shown an 8 year survival rate of 91% for low risk, 90% for low-intermediate risk, 67% for highintermediate risk, and 31% for high risk cases with few of the side effects associated with Burkitt's lymphoma chemotherapy. [12
Família Herpesviridae • Subfamília Betaherpesvirinae – Citomegalovírus (CMV ou HHV-5) – Roseolovírus (vírus da roséola, HHV-6)
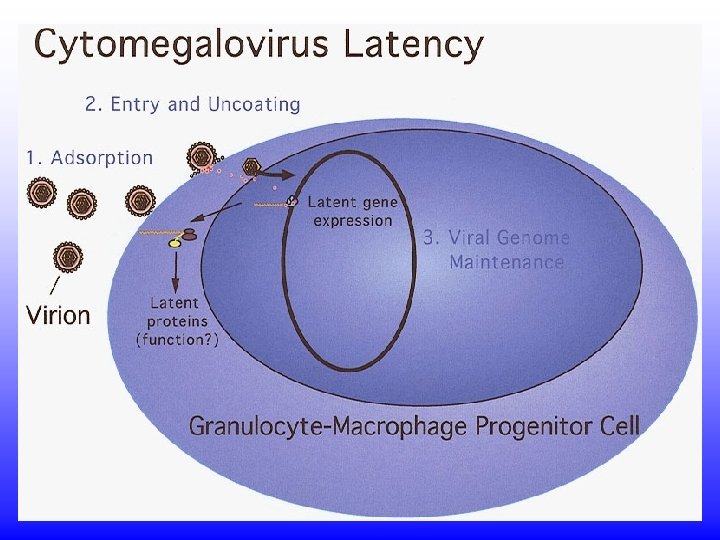
Citomegalovírus (CMV) - é um betaherpesvírus; HHV-5, um só sorotipo - infecção muito prevalente; doença muito rara - neonatos: doença de inclusão citomegálica - mononucleose infecciosa negativa para Acs. Heterófilos - pneumonia em imunocomprometidos - células gigantes => inclusão citomegálica - Latência em células linfóides
Citomegalovírus (CMV) TRANSMISSÃO E EPIDEMIOLOGIA: - Acs em ~80% adultos - eliminação de vírus esporádica - infecções: -congênita -pós-natal
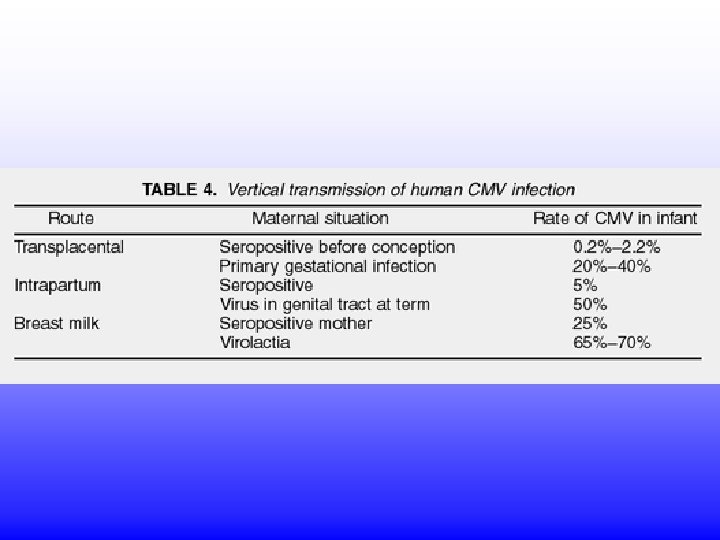
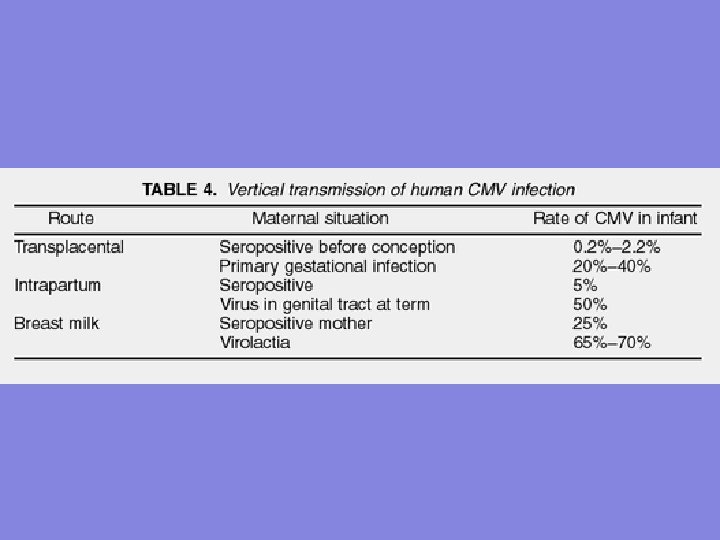
CMV INFECÇÃO PRÉ-NATAL: - em qualquer estágio da gestação - risco de transmissão: 0, 2 a 2% - 5 a 15% destes podem apresentar lesões congênitas - infecção intrauterina => crianças disseminam o vírus por mais tempo - > risco = infecção 1ária na gestação - infecção prévia = risco muito baixo
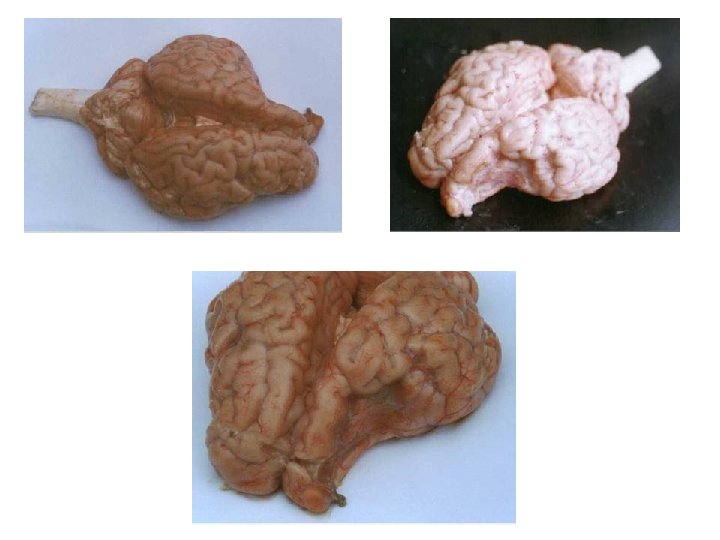
SÍNDROME CONGÊNITA • Mãe infectada com reativação do vírus, reinfecção ou persistente infecção primária. • Causa danos severos no sistema nervoso, afeta a formação de diferentes órgãos e tecidos (ouvidos, olhos, fígado, rins, pele, etc), • Anemia, trombocitopenia e leucopenia. • Pode afetar a placenta.
RECÉM NASCIDO COM SÍNDROME CONGÊNITA
RECÉM NASCIDO INFECTADO POR CMV
Retinite por CMV
CMV Infecção intrauterina ou pré-natal Achados clínicos: - microcefalia - convulsões - icterícia - hepatosplenomegalia - retardo mental - surdez (mais comum)
CMV Congênito Doença de inclusão citomegálica
INFECÇÃO PÓS-NATAL: - geralmente na infância (MI rara) - MI Paul Bunnel - negativa - infecção em adultos > chance de MI - pode ocorrer durante o parto - através do leite => mais comum - transmissão sexual (sêmen, secr. cervicais) - transmissão por hemoderivados - transplantados renais: reativação e disseminação do vírus CMV
Retinite por CMV
Doença de inclusão citomegálica
CMV EBV
CMV Infecção pós-natal: - MI heterófilo- negativa; - Febre, letargia, linfócitos anormais no sangue periférico; - usualmente sem faringite ou linfadenopatia -retinites - às vezes após transfusão com sangue fresco (vírus inativado em refrigeração)
CMV Em imunodeprimidos: - infecções frequentes - transplantes renais: assintomáticas - grave em transplantados de medula e coração => pneumonia intersticial e retinite
Diagnóstico laboratorial (2) 1. Teste para antigenemia (CMV) - Antígenos do CMV detectados na superfície de leucócitos polimorfonucleares por imunoperoxidase (IPX) ou imunofluorescência direta (IFD). 2. Polymerase chain reaction (PCR) – é hoje o método de escolha. 3. aumento de Ig. G e presença de Ig. M.
Imunoperoxidase
Imunofluorescência Direta anticorpo marcado sobre material infectado (suspeito) + anticorpo específico marcado com FITC + luz UV ____________________ reação colorida
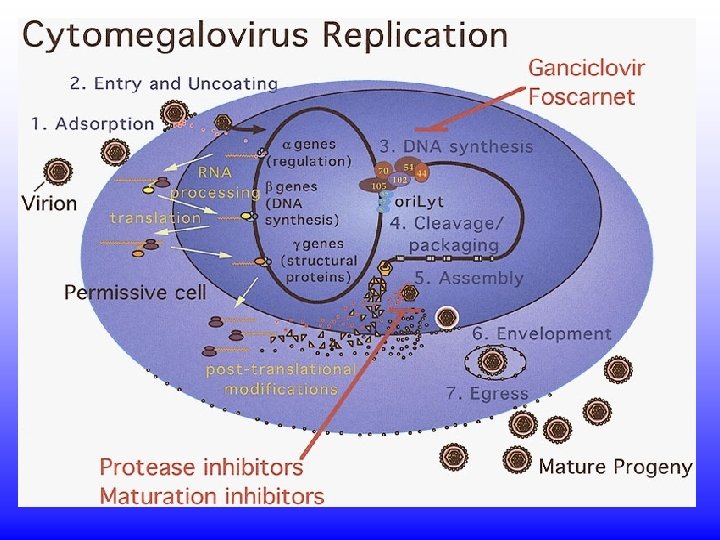
CMV Tratamento: - acyclovir : não muito eficaz - ganciclovir (em pneumonias e retinites) - foscarnet (retinites): inibidor da DNA polimerase viral
CMV Prevenção: - não há vacina - Acompanhar a evolução da infecção em transplantados e imunodeprimidos Iniciar tratamento se viremia ocorrer.
Roséola (HHV-6 e HHV-7) A apresentação clássica da roséola ocorre em crianças de 9 - a 12 meses que desenvolvem uma febre aguda e seguidamente uma convulsão febril. Após 3 dias , uma rápida defervescência ocorre e um exantema morbiliforme aparece.
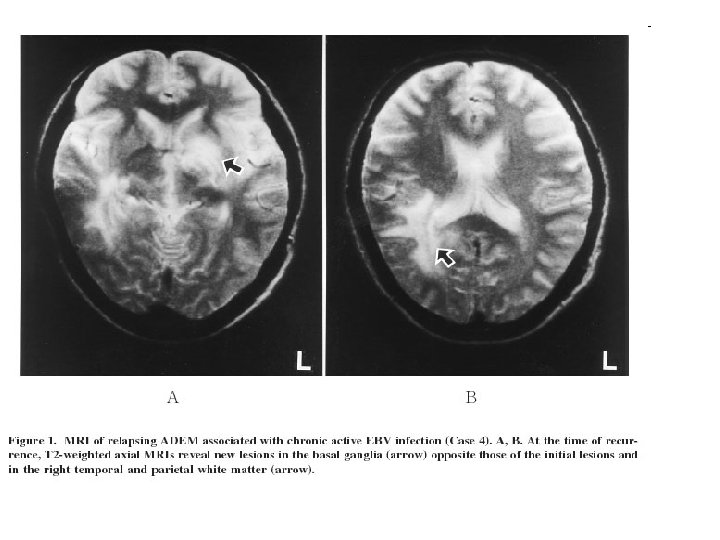
Roséola Patofisiologia In the primary infection, replication of the virus occurs in the leukocytes and the salivary glands. HHV-6 is present in saliva. Early invasion of the CNS is believed to occur, thus accounting for seizures and other CNS complications. Although rare in the primary disease of infancy, generalized organ involvement has been reported with gastrointestinal, hematopathic syndromes; hepatitis; and hepatosplenomegaly. Following the acute primary infection, HHV-6 remains latent in lymphocytes and monocytes and has been found in low levels in many tissues. Peripheral blood mononuclear cell cultures develop enlarged balloonlike cells. Cells supporting virus growth are CD 4+ T lymphocytes. HHV-6 downregulates the host immune response through several mechanisms, including molecular mimicry by production of functional chemokine and chemokine receptors. The 2 variants of HHV-6 are A and B. The genomes of HHV-6 A/B have been sequenced. HHV-6 B, the main cause of roseola, consists of 97 unique genes. CD 46 is the cell receptor for HHV-6, which imparts the virus' broad tissue tropism. A possible association of HHV-6 and multiple sclerosis has been suggested but is still inconclusive. HHV-6 has been isolated in Kaposi’s sarcoma (caused by human herpesvirus 8), in which it may contribute to tumor progression. HHV-6 may facilitate oncogenic potential in lymphoma and has been associated with chronic fatigue syndrome.
HHV-7 • • Signs and symptoms HHV-6 B and HHV-7, as well as other viruses, can cause a skin condition in infants known as exantema subitum , although HHV-7 causes the disease less frequently than HHV-6 B. [4] HHV-7 infection also leads to or is associated with a number of other symptoms, including acute febrile respiratory disease, fever, rash, vomiting, diarrhea, low lymphocyte counts, [5] and febrile seizures, [6] though most often no symptoms present at all. [7] There are indications that HHV-7 can contribute to the development of syndrome de hipersensibilidade induzida por medicamentos, [8] encefalopatia[9] sindrome hemiplegia, hemiconvulsão- epiplepsia, [10] hepatite, [11] postinfectious myeloradiculoneuropathy, [12] pitiríase rósea, [13] e reativação de EBV HHV-4, levando a doença “mononucleose-like". [14] Complications with HHV-7 infection has been shown to be a factor in a great variety of transplant types. [
HHV-7 • • • Structure A mature virus particle measures about 170 nanometres (1, 700 Å) in diameter. [15] The genome of HHV-7 is very similar to that of HHV-6, although it is about 10% smaller, [16] with a DNA genome of about 145, 000 base pairs. [7] There a number of key differences between the genome of HHV-7 and that of HHV-6, but the importance of them for viral DNA replication is not yet known. [7] Cellular effects HHV-7 resides mostly in CD 4+ T cells[17] albeit only in certain strains of them. [18] To enter CD 4+ T cells, HHV-7, unlike HHV-6, uses CD 4 and possibly some cellsurface glycoproteins to enter CD 4+ T cells. [19] About a week after HHV-7 has infected a cell, it begins to downregulate CD 4 transcription, [20] which interferes with HIV-1 infection[21] but may reactivate HHV-6 infection. [22] It is however unclear exactly what effect HHV-7 has on HIV infection. [7] HHV-7 also has a number of other effects on cells. Among these include membrane leaking, the presence of lityic syncytia, [23] occasional apoptosis, [24] the supporting of latent infection, [25] and increases and decreases in levels of certain cytokines. [26]
HHV-7 • • • Diagnóstico e tratamento Em adultos, os effects de HHV-7 separados de HHV-6 ainda não são bem documentados. Isto porque a detecção de HHV-7 era inicialmente difícil de ser feita rapidamente. Uma técnica denominada loop-mediated isothermal amplification (LAMP) foi recentemente introduzida. No reliable serological test has been developed yet for HHV-7 alone, but multiple are in the process of being developed. [7] The use of PCR assays to test for HHV-7 is also being explored. [7][29] No treatment for HHV-7 infection exists, but no clinical situation where such treatment would be useful has yet been discovered. [7] Epidemiological Over 95% of adults have been infected and are immune to HHV-7, [30] and over three quarters of those were infected before the age of six. [31] Primary infection of HHV-7 among children generally occurs between the ages of 2 and 5, which means it occurs after primary infection of HHV-6. [32]
Herpesvírus Humano 8 (HHV-8) • Tumor associado à ocorrência do Sarcoma de Kaposi e outros linfomas menos conhecidos (doença de Castleman e outros). • Tumor prevalente em homossexuais masculinos com AIDS. • DNA do vírus encontrado em 100% dos casos de KS. • A maioria dos pacientes com KS tem anticorpos anti-HHV-8. • A soroprevalência de anticorpos anti-HHV-8 é baixa na população em geral, mas alta em suscetíveis ao KS, como homossexuais masculinos. • O tratamento com anti-retrovirais leva à regressão rápida dos tumores • Diferente dos demais herpes humanos, o HHV-8 não tem distribuição ubíqua.
Consulte nossa home page • • • www 6. ufrgs. br/labvir Referências adicionais: Wikipedia Site do CDC Site: All the virology in the web (ATV) Site de Vincent Racaniello (virology blog): www. virology. ws