HERNIA Presenter Golnaz Malekzadeh DEFENITION A hernia is































































- Slides: 100
HERNIA Presenter: Golnaz Malekzadeh
DEFENITION: Ø A hernia is an abnormal weakness or hole in an anatomical structure which allows something inside to protrude through. Ø It is commonly used to describe a weakness in the abdominal wall.
SIGNS AND SYMPTOMS The signs and symptoms of a hernia can range from noticing a painless lump to the painful, tender, swollen protrusion of tissue that you are unable to push back into the abdomen—possibly a strangulated hernia.
Hernias by themselves usually are harmless, but nearly all have a potential risk of having their blood supply cut off (becoming strangulated). Ø If the blood supply is cut off at the hernia opening in the abdominal wall, it becomes a medical and surgical emergency. Ø
CAUSES OF HERNIAS Any condition that increases the pressure of the abdominal cavity may contribute to the formation or worsening of a hernia. Obesity Heavy lifting Coughing Straining during a bowel movement or urination Chronic lung disease Fluid in the abdominal cavity Hereditary
COMPLICATIONS lordosis Ø Constipation Ø Urine retention Ø Difficulty in breathing Ø Compartment syndrome Ø And …. Ø
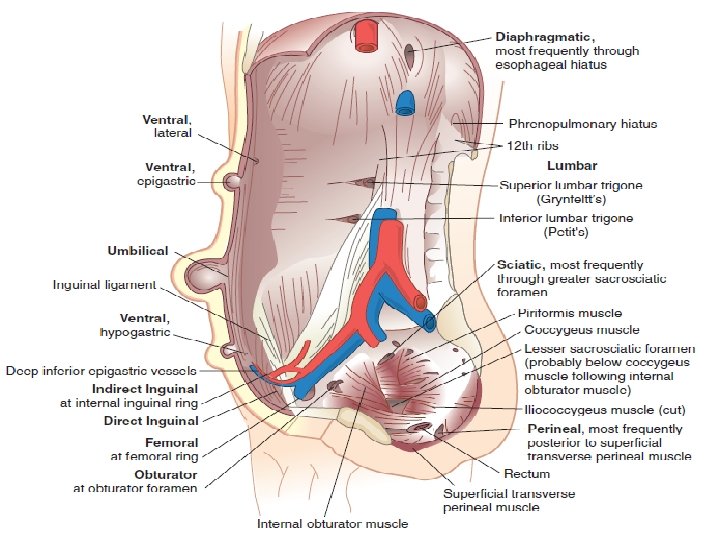
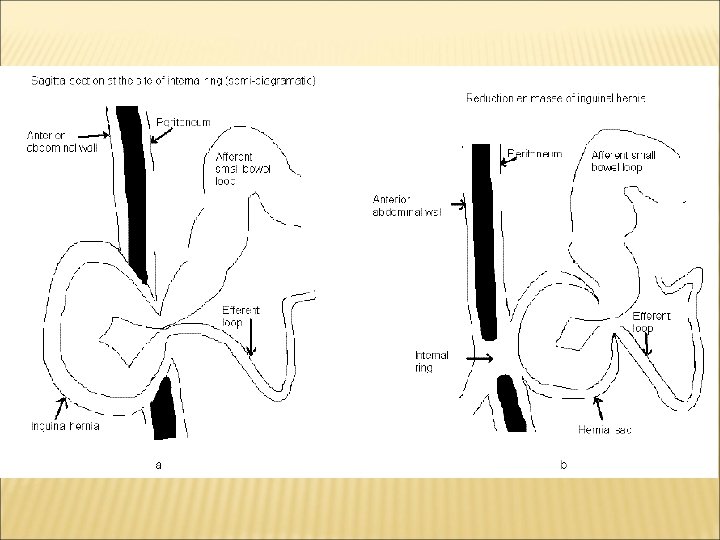
TYPES OF HERNIA 1. External 2. Internal 3. intermittent
CLINICAL TYPES OF HERNIA 1. reducible hernia is one in which the contents of the sac return to the abdomen spontaneously or with manual pressure when the patient is recumbent. 2. irreducible hernia is one whose contents or part of contents cannot be returned to the abdomen, without serious symptoms. hernias are trapped by the narrow neck
CLINICAL TYPES , CONTINUED… incarcerated hernia: is one whose contents cannot be returned to the abdomen, with severe symptoms. strangulated hernia: denotes compromise to the blood supply of the contents of the sac. incarcerated hernia and strangulated hernia are the two stages of a pathologic course Richter’s hernia (intestinal wall hernia ) a hernia that has strangulated or incarcerated a part of the intestinal wall without compromising the lumen. Sliding hernia is one in which the wall of a viscus forms a portion of the wall of the hernia sac. It is may be colon ( on the left), caccum (on the right) or bladder (on either side). Belongs to irreducible hernia Littre hernia: a hernia that has incarcerated the intestinal diverticulum (usually Meckel diverticulum).
HERNIA
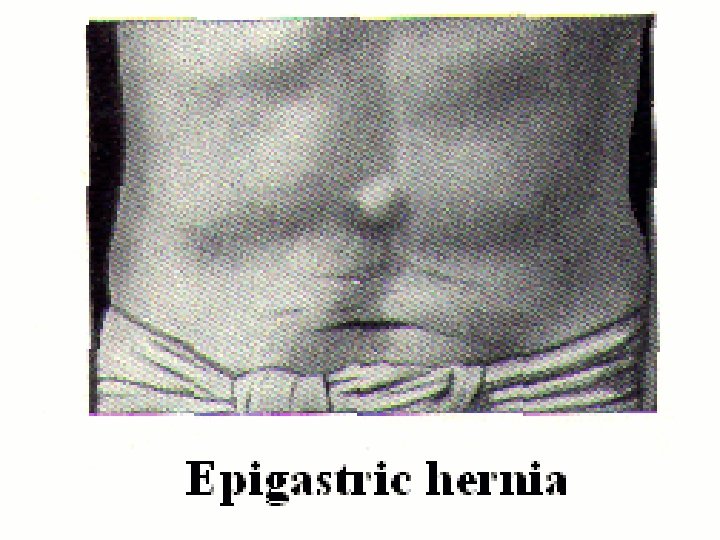
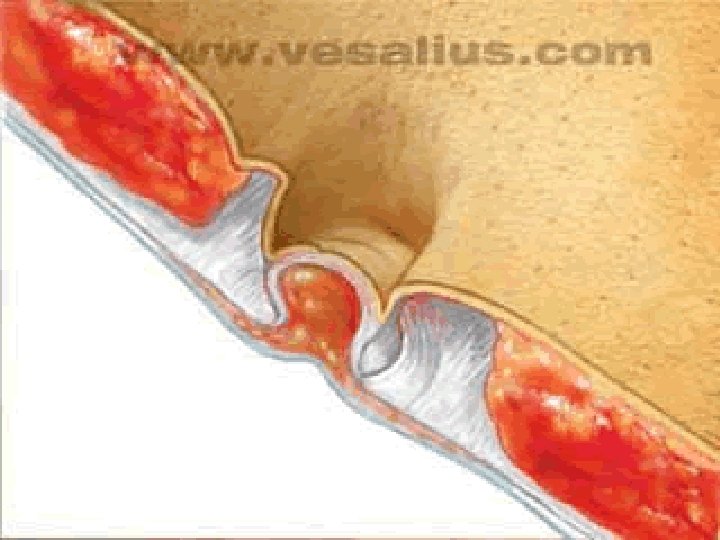
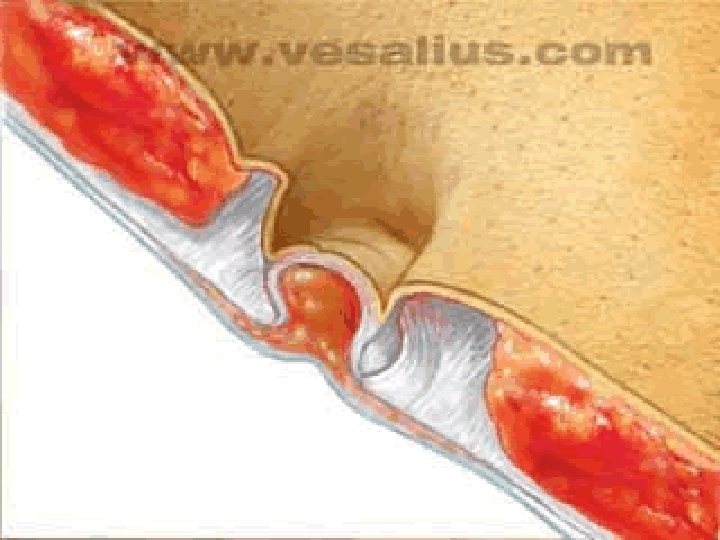
EPIGASTRIC HERNIA Occurring between the navel and the lower part of the rib cage in the midline of the abdomen, these hernias are composed usually of fatty tissue and rarely contain intestine. Ø Men > Women Ø these hernias are often painless and unable to be pushed back into the abdomen when first discovered. Ø
UMBILICAL HERNIA 1 - Congenital 2 - Adault acquired
CONGENITAL UMBELICAL HERNIA Common in infants Ø Close spontaneously if <1. 5 cm Ø Repair if > 2 cm or if persists at age 5 years Ø Ø Repair primarily or with mesh
UMBELICAL HERNIA Ø Ø Women > men Risk factors Multiple Pregnancies Prolonged labor Ascites Large Abdominal Tumors-CT scan may be indicated for some patients Activities which result in strenuous physical activity(occupational or recreational : example weight lifting)
UMBELICAL HERNIA REPAIR Ø Morbitiy and incarceration rate considered to be high enough to warrant repair. One study showed incarceration twice that of femoral hernia. Ø Unfortunately, recurrence rates as high as 20 -28 % have been recorded. Ø patients with ascites ? ? ?
. . Desktopventral herniaher. L 5175 umb 6
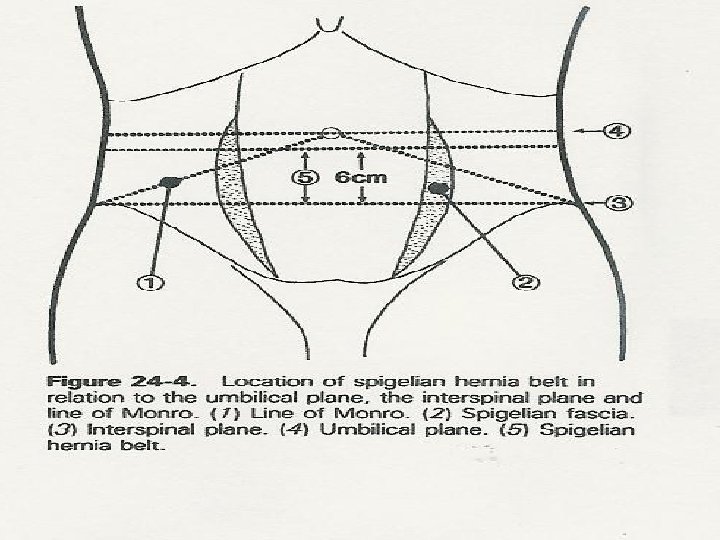
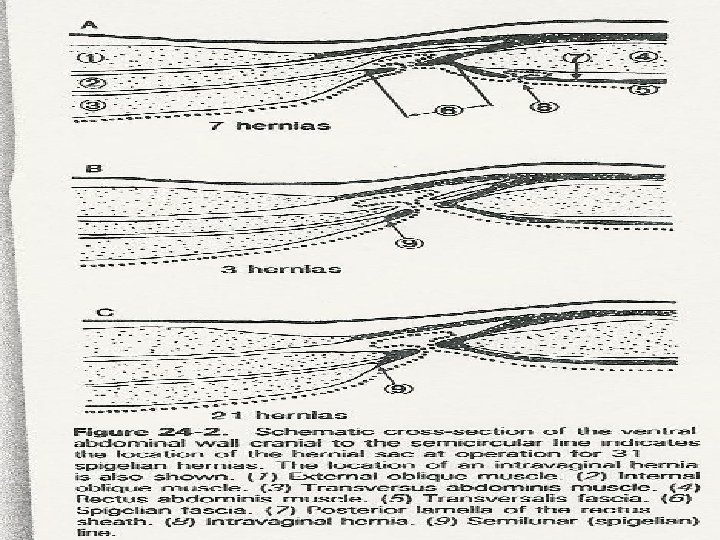
SPIEGHELIAN HERNIA
SPIGELIAN HERNIA Ø Ø Rare Hernia through subumbilical portion of semi-lunar line Difficult to diagnose –Abdominal pain or mass noted in abdominal wall. Frequently tender over area Clinical suspicion (location) CT scan Repair primarily or with mesh
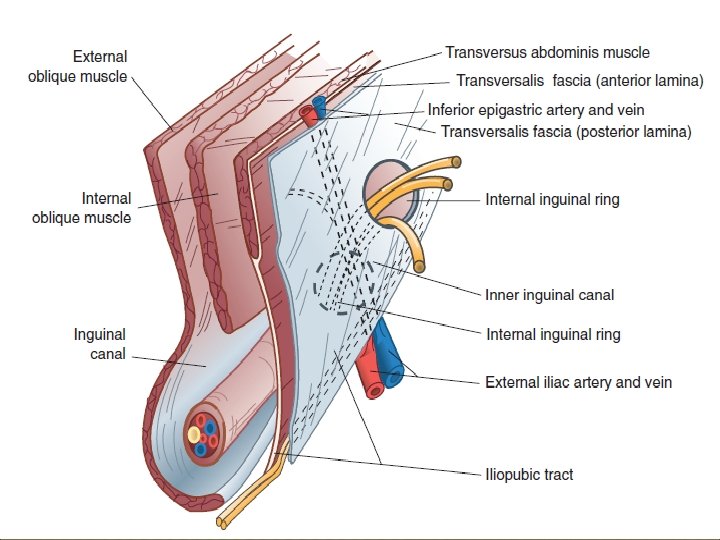
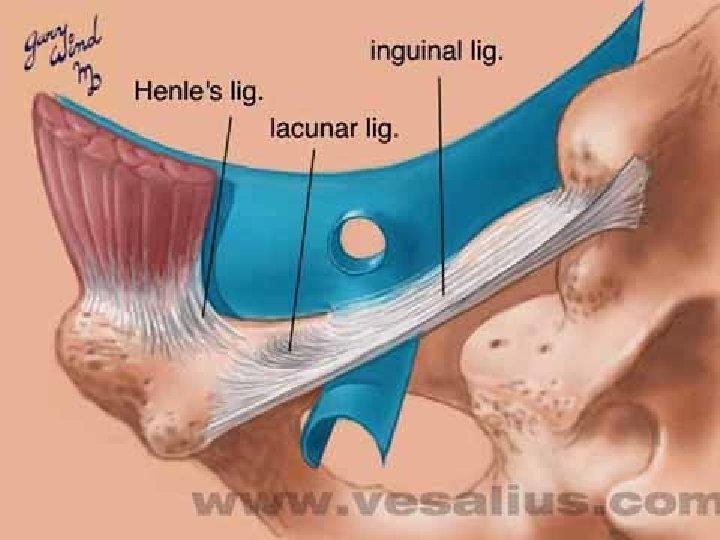
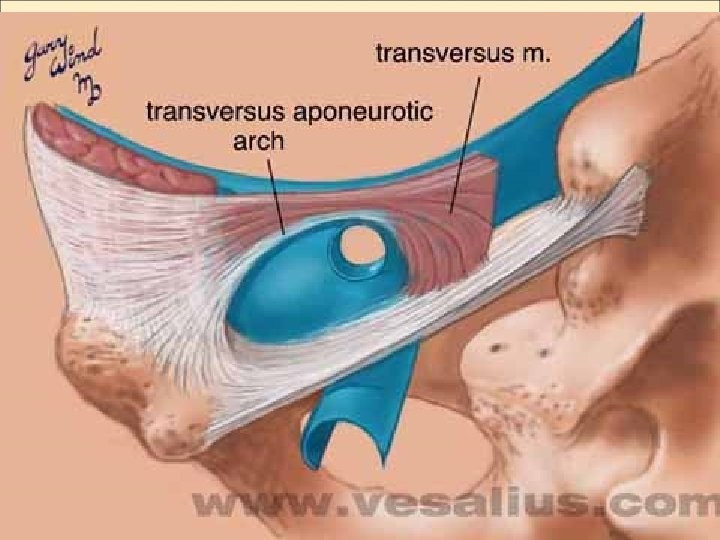
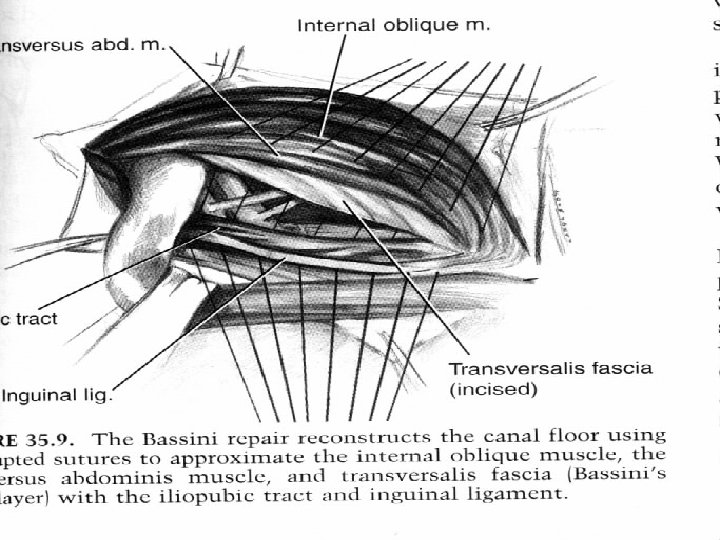
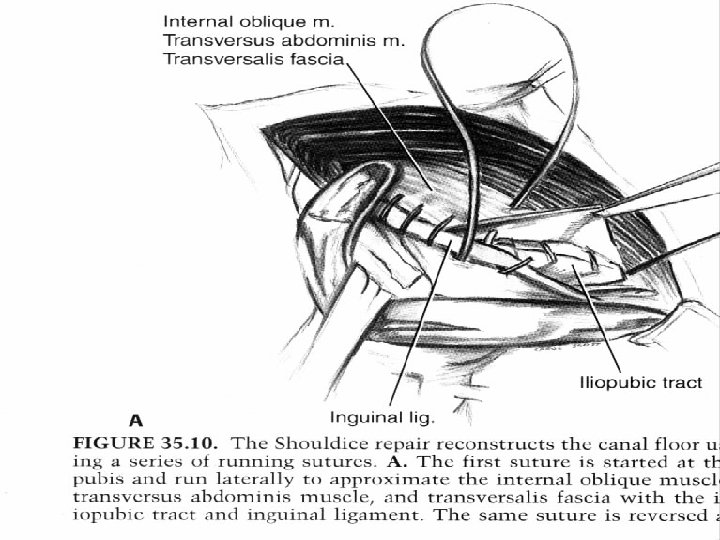
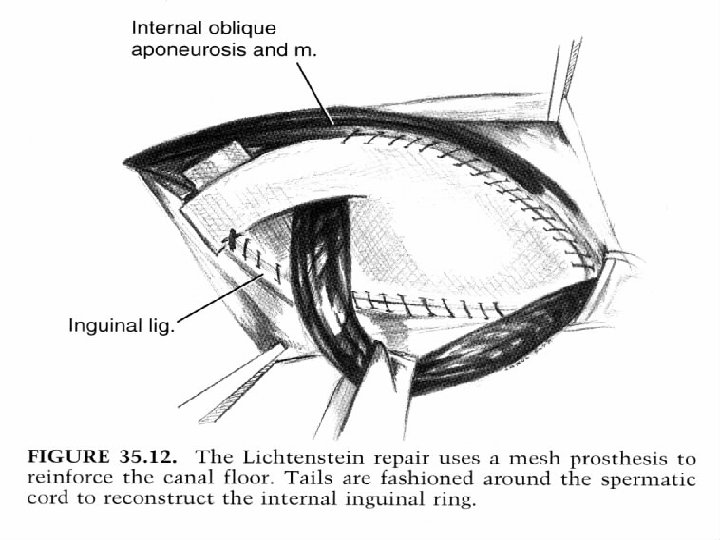
INGUINAL HERNIA a protrusion of part of the contents of the abdomen through the inguinal region of the abdominal wall.
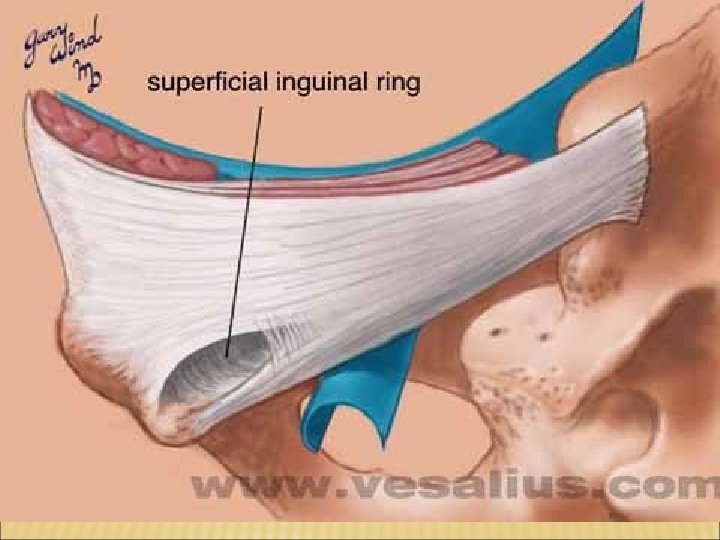
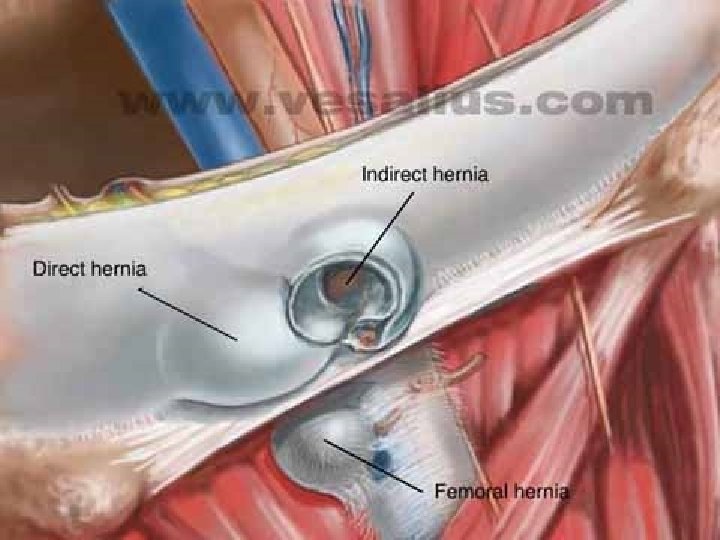
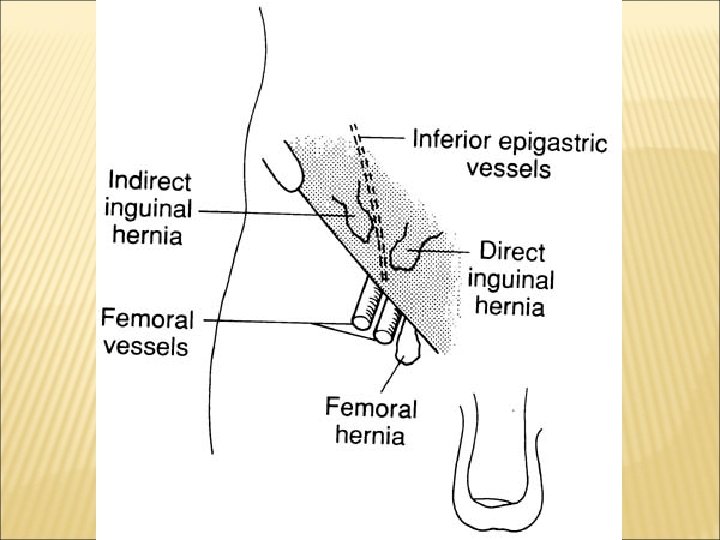
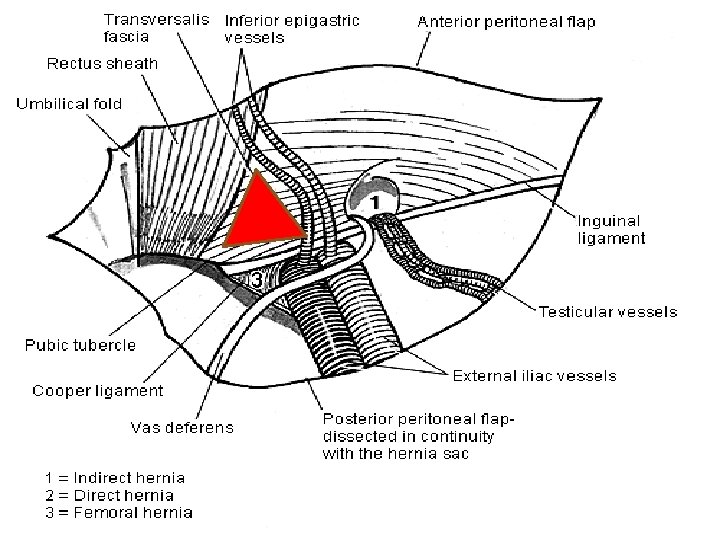
CLINICAL TYPES OF INGUINAL HERNIA indirect inguinal hernia: the internal inguinal ring the inguinal canal external inguinal ring scrotum Ø direct inguinal hernia: Hesselbach’s triangle Ø Pantaloon type Ø
RISK FACTORS Ø Ø Ø Ø Hereditary Smoking CDH Sedentary life style acquired weakness or defect of abdominal wall Increased intra abdominal pressure And ….
DIFFERENCES BETWEEN INDIRECT AND DIRECT HERNIA feature indirect age children, young people aged people pathway of protrusion coming down the inguinal canal, may enter the scrotum pass through Hesselbach’s triangle, rarely enter the scrotum contours of sac elliptic, pear-shaped semispheric, wide base Relationship of spermatic cord with sac Posterior to the sac Anterior and lateral to the sac Relationship of sac neck with inferior epigastric artery Sac neck is lateral to it Sac neck is medial to it Incarcerated incidence high low
PHYSICAL EXAM
SILK GLOVE SIGN Ø Palpation of hernia sac on spermatic cord
DIFFERENTIAL DIAGNOSIS Ø Ø lymph node lipoma saphenous varicosity mass
SURGERY COMPLICATIONS Recurrence Neuralgia Ilioinguinal Iliohypogastric Genitofemoral Lateral cutaneous Ischemic orchitis Injury to vas deference Wound infection Bleeding
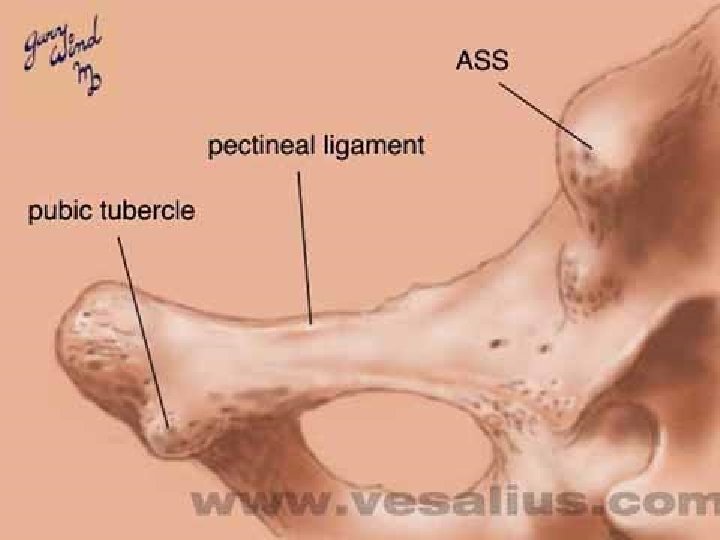
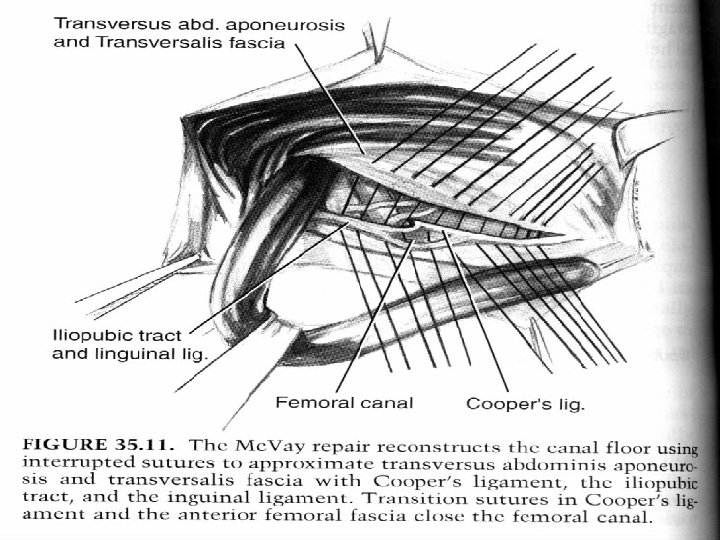
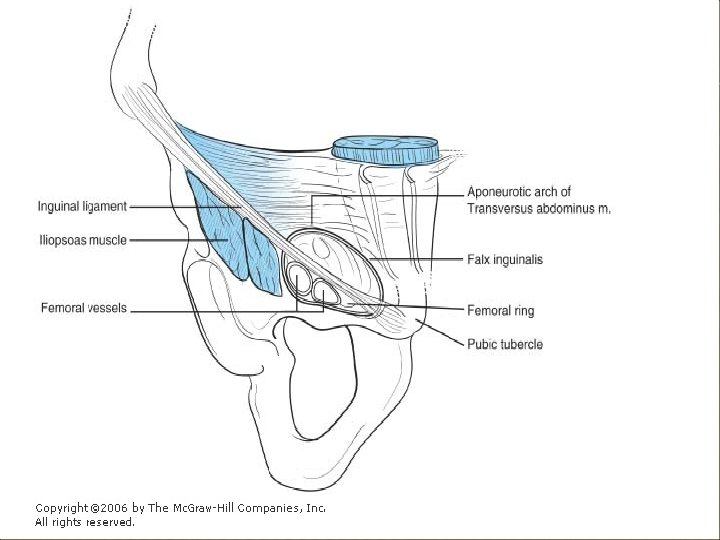
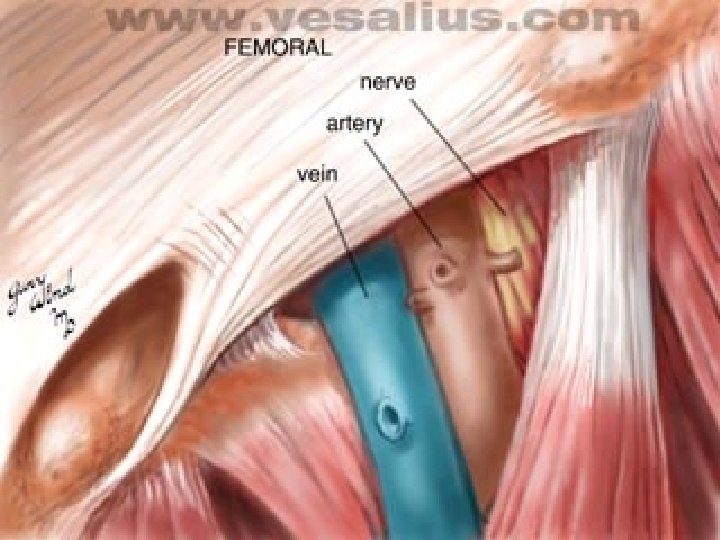
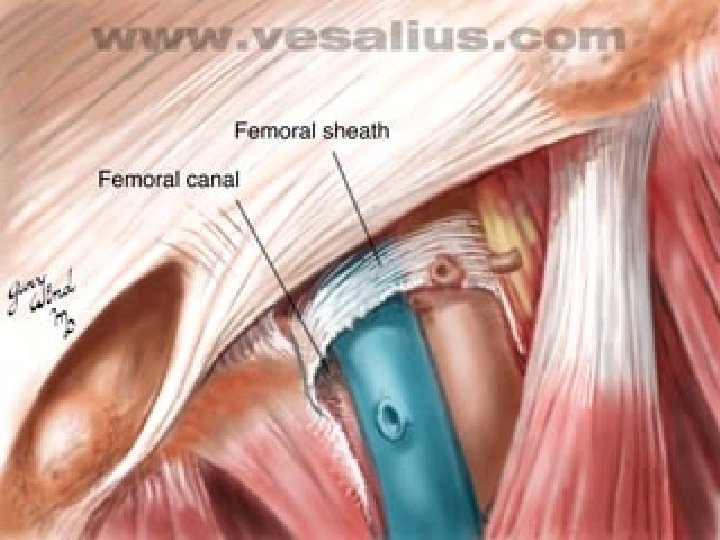
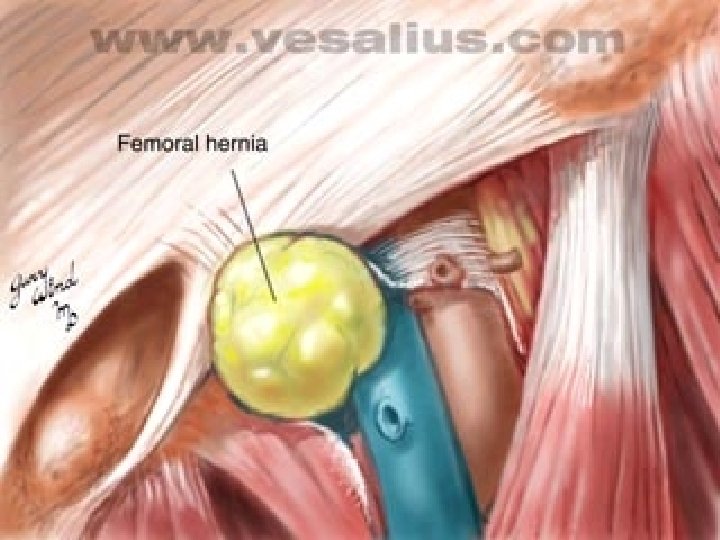
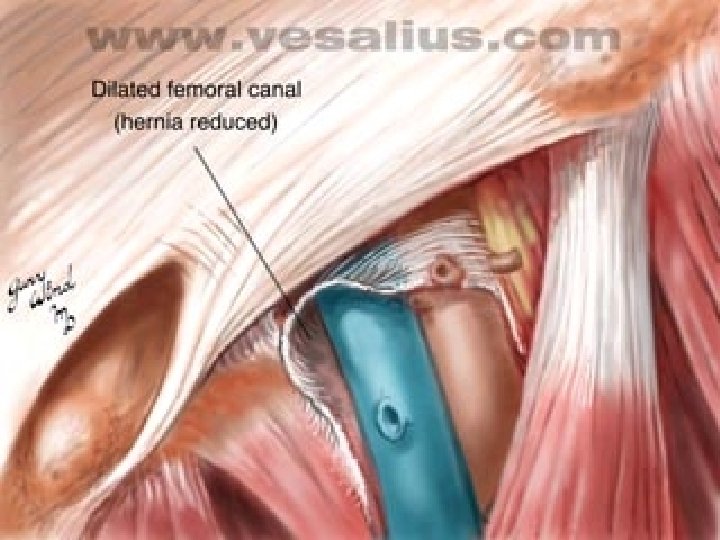
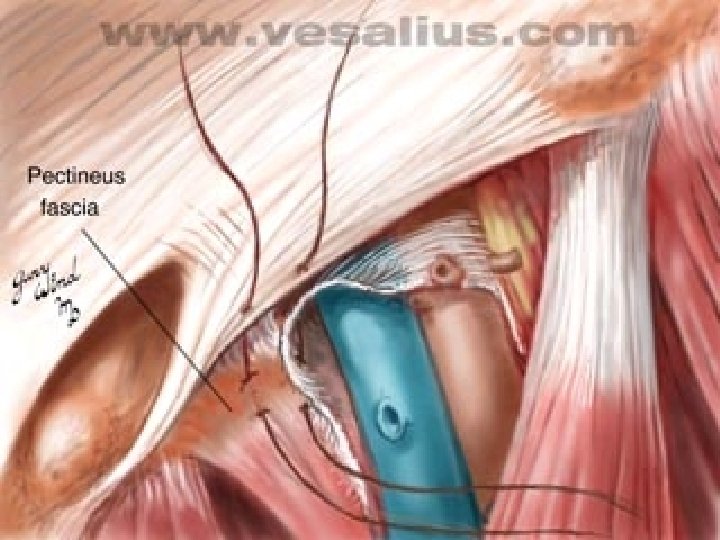
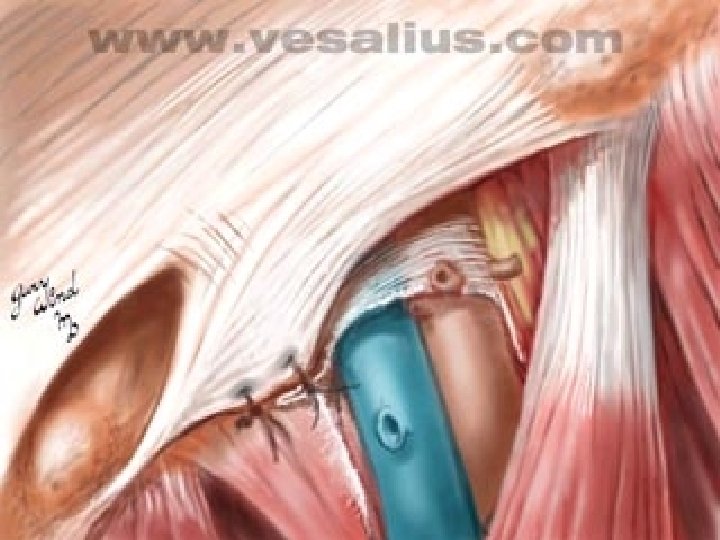
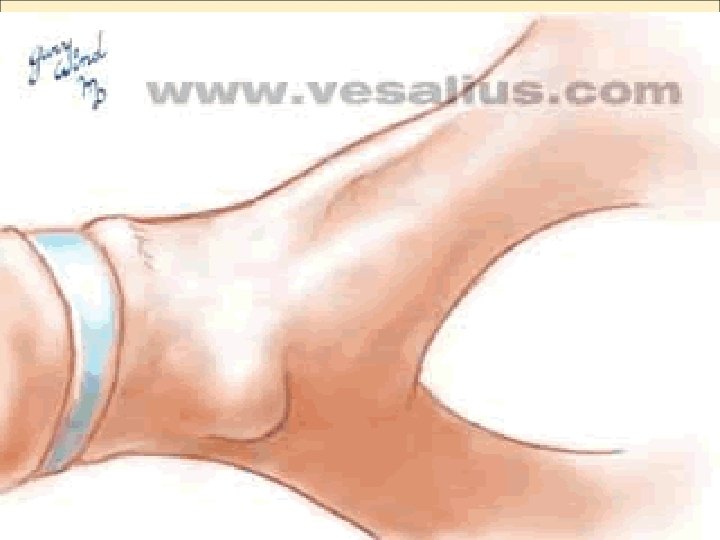
FEMORAL HERNIA
FEMORAL HERNIA All are acquired. Ø Are secondary to an expanded femoral ring. Ø Probably due to increased intra abdominal pressure Ø Diagnosis by physical exam. Ø
DIFFERENTIAL DIAGNOSIS 1. indirect inguinal hernia 2. lipoma 3. groin lymph nodes 4. long saphenous varix 5. iliolumbar tuberculous abscess
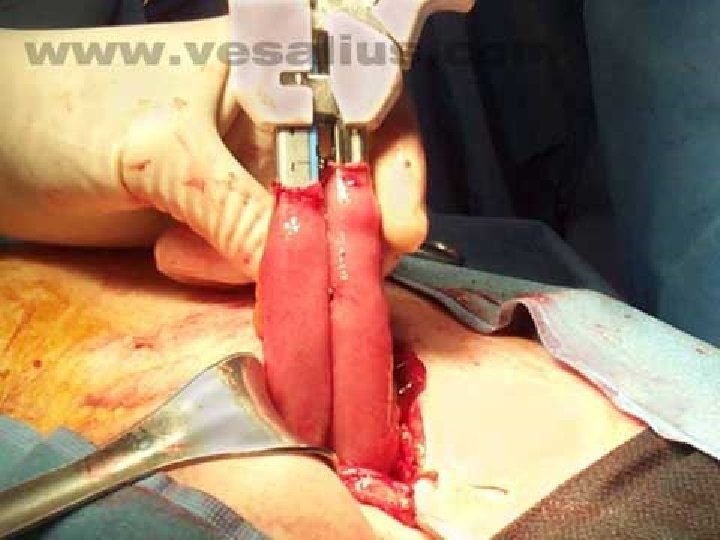
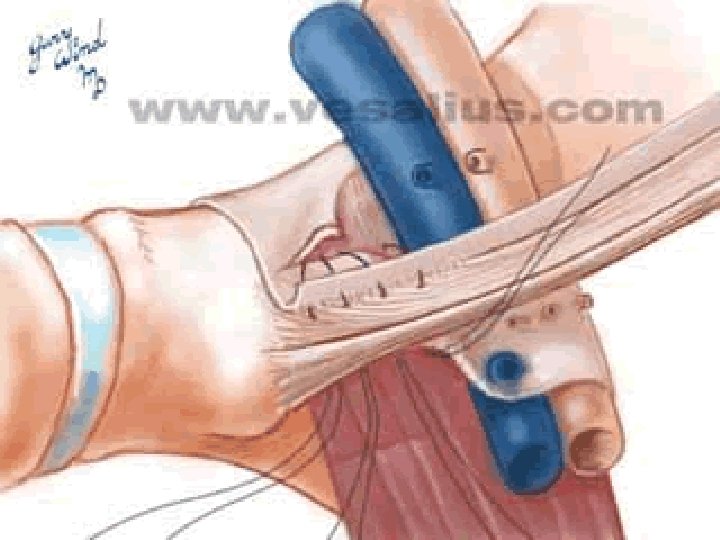
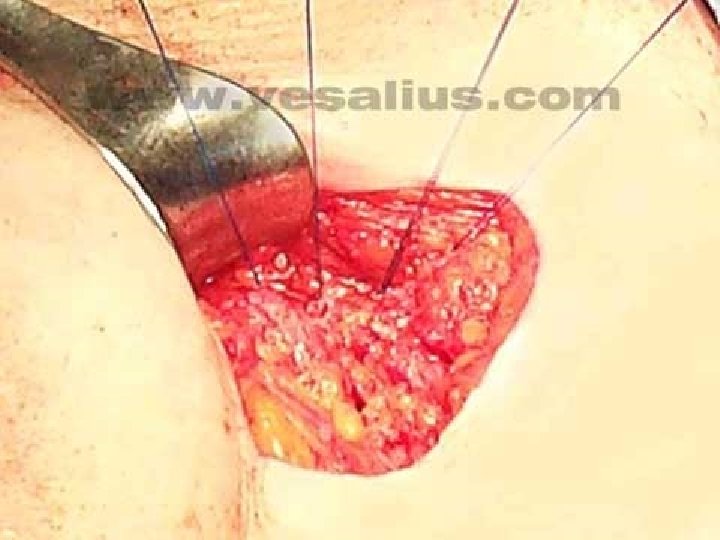
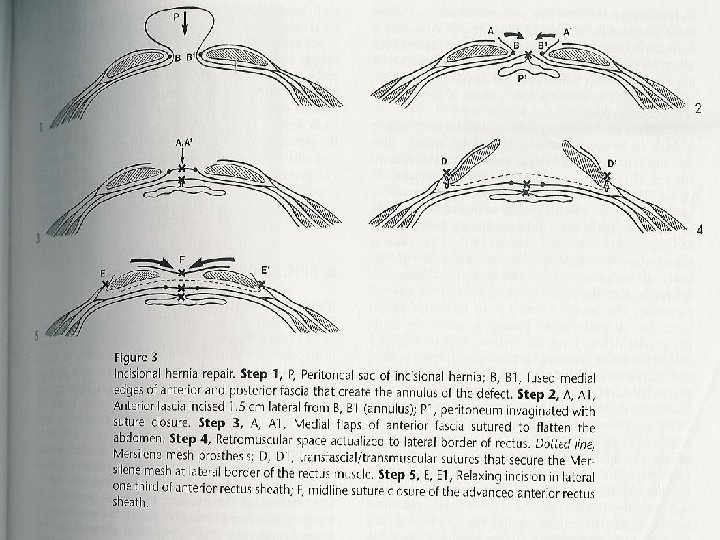
INCISIONAL HERNIA an abnormal protrusion of a viscus through the musculoaponeurotic layers of a surgical scar. Ø Swelling and mass in the incision Ø Rarely incarcerate Ø
ETIOLOGY Operative factors: - types of incision: vertical incision, transrectus incision, midline incision, standard paramedian incision - technique of closure - suture material Postoperative factors: - increased intra-abdominal pressure - Obesity - Malnutrition - Smoking -Immune dificiency
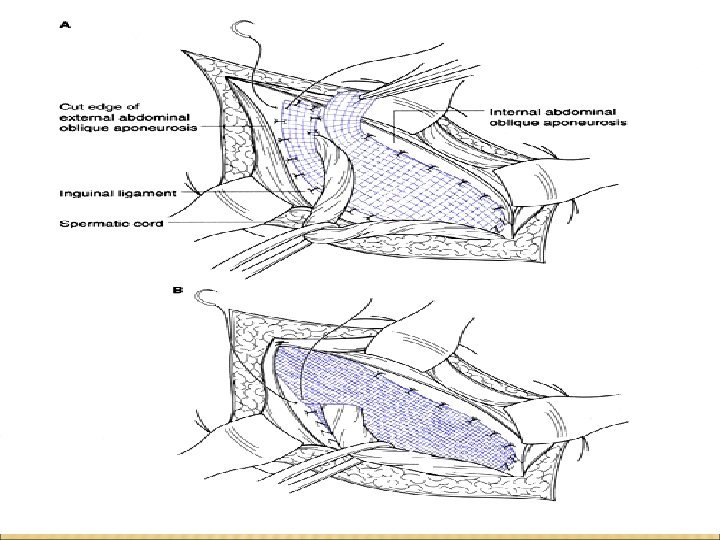
REPAIR Bring together fresh fascial edges after trimming sac Clean off fascial edges at least 1 cm back Close with interrupted or continuous sutures Even with careful technique recurrence rates as high as 50% have been reported
TAXIS 1 - Trendelenberg position 2 -morphin+ diazpam 3 -ice bag
TAXIS Contra indications: Fever Lococytosis Positive abdominal sign Erythema of skin