HEPATITIS VIRUS 5 medically important hepatitis viruses 1








")

 Pre-Icteric phase: fever, nausea , vomiting Icteric")



")


 PROPERTIES DNA virus, Hepadnaviridae Family Icosahedral nucleocapsid")
 HBs. Ag was first discovered in serum")


 • Australia Ag • Detected in")
 ‘a’ – group specific antigen ‘d’")













")


 HBs. Ag-")



 First Ab to be elevated following infection Appears")

 Imaging of liver for evidence of hepatoma etc.")
, tenofovir -")

 made in bakers")

 High titer of HBs. Ab prepared from sera of")

 -Boiling water 5 mins -dry")











")















- Slides: 100
HEPATITIS VIRUS
5 medically important hepatitis viruses: 1. Hepatitis A: infectious heptitis 2. Hepatitis B: Serum hepatitis 3. Non-A, Non-B: HCV 4. Hepatitis D (delta agent) 5. Hepatitis E : Enteric Hepatitis 6. Post transfusion: HGV Other viral causes: EB virus, CMV, Yellow fever, Enterovirus, Herpes virus
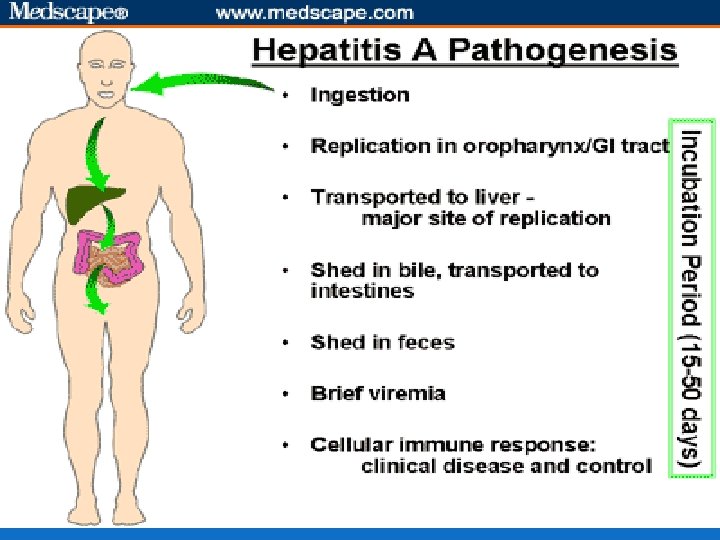
HEPATITIS A VIRUS Causes Hepatitis A It is a enterovirus, family picornaviridae Recently classified under Hepatoviruses ss RNA, non-enveloped. Icosahedral nucleocapsid Replicates in the cytoplasm of the cell
Also known as enterovirus 72 It has 1 serotype It has no antigenic relationship b/w hepatitis B or other hepatitis viruses Replication- similar to enteroviruses. Eg-polio virus.
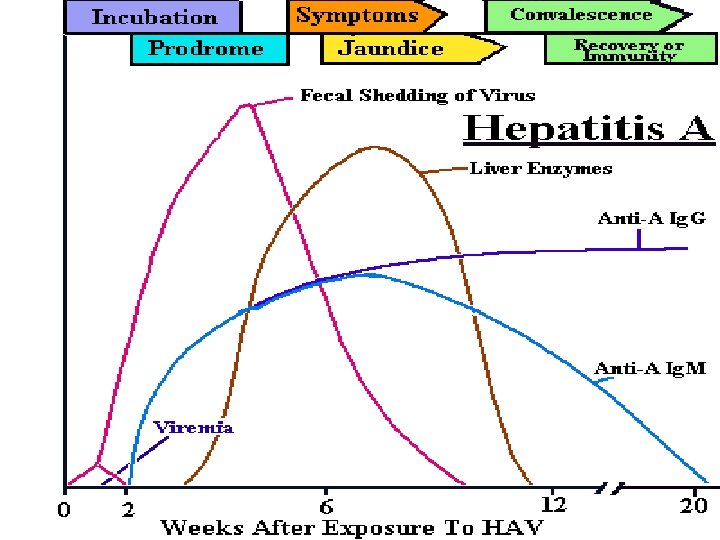
Transmission and Epidemiology Faeco-oral route Reservoir : - humans Children adolescents more commonly infected (an-icteric subclinical infection) Adults: icteric manifestations Virus is shed 2 weeks before & after appearance of symptoms.
Institutional outbreaks recorded. Eg- day care centres, hostels, ICU Outbreaks directly related to sanitation. Eg - fecal contamination of drinking water, food grown in polluted water, street food. Rarely transmitted by blood. Eg- seen rarely with haemophiliacs transfused with blood products
There is no chronic infection unlike in HBV or HCV because generally level of viremia is low. Many people maybe infected and recovered (Ig. A seen in 50 -70% of population) Secondary attack rate in house hold contacts common
Pathogenesis and immunity Virus replicates in GI tract and spread to liver hematogenously Hepatocytes are infected but mechanism of cell damage is unclear. Cytotoxic T-cells may damage the hepatocytes infected with virus. If infection is cleared damage will be repaired and there is no chronic infection
Hepatitis from other virus usually indistinguishable pathologically (all look the same histo-pathologically)
Immune response Ig. M is detected at the appearance of jaundice Peaks 2 -3 weeks, disappears in 3 -4 months So Ig. M Ab to HAV is important in diagnosis of HAV. 1 -3 weeks after the Ig. M appears Ig. G is seen. Ig. G : provides life long immunity
Clinical features Incubation period (2 -4 weeks) Pre-Icteric phase: fever, nausea , vomiting Icteric Phase: jaundice, dark urine, pale stools, eleavted transaminases.
Spontaneous recovery is the rule in 2 -3 weeks time Most of the cases maybe asymptomatic (maybe solely detected on basis of Ig. G Ab) No chronic hepatitis or chronic carrier state So no predisposition to hepatocellular carcinoma
Laboratory diagnosis 1. Biochemical investigations- LFT 2. Detection of anti HAV Ig. M, Ig. G: persists for decades 3. Detection of HAV particles: IEM of faeces, liver, bile 4. HAV antigen detection: by ELISA 5. Isolation in cell culture possible but not routinely done 6. PCR: viral RNA
Serological tests for Hepatitis A virus Stage of infection Ig. M Ig. G Acute HAV infection + ---- Previous HAV infection __ +
Treatment and prevention No antiviral therapy Formaldehyde inactivated vaccine: (virus grown in cell culture) given to children above 12 months & adults- initial dose and booster dose 6 -12 months later
Live attenuated vaccine: single dose , S/c Detection of HAV antibody prior to vaccination is cost-effective Passive immunization with immunoglobulin (HAV Ig) for post exposure prophylaxis can prevent disease in close household contacts & travellers
Proper hygiene and superior sewage disposal, hand washing after bowel movements etc Good sanitation help prevent (like for any food/water borne diseases) Chlorination of water also helps.
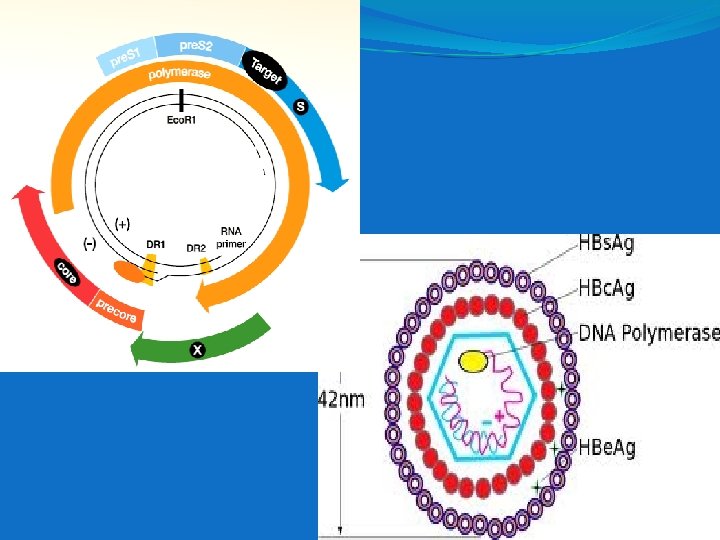
HEPATITIS B VIRUS Causes Hepatitis B (HBV) PROPERTIES DNA virus, Hepadnaviridae Family Icosahedral nucleocapsid containing partially ds circular DNA genome. (all other Hepatitis group are RNA viruses).
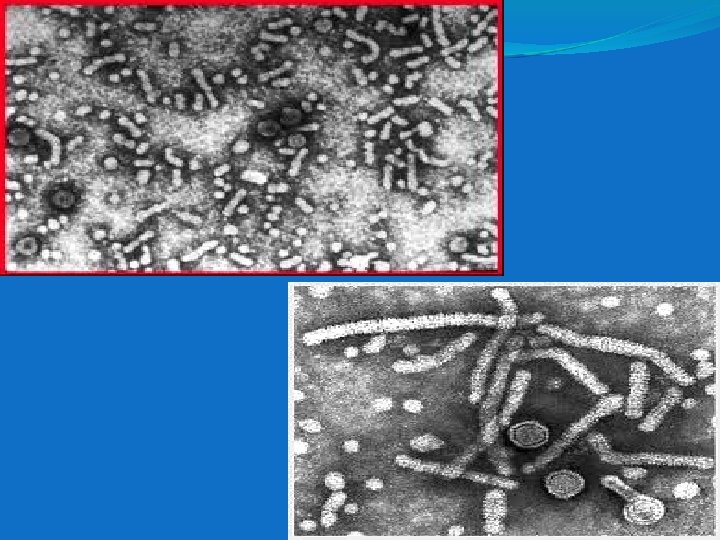
Envelope contains protein surface antigen(HBs. Ag) HBs. Ag was first discovered in serum of Australian aborigine. So it is called Australia Antigen.
MORPHOLOGY: EM of serum from infected patients reveals 3 morphologic forms: Spherical forms: Most numerous 22 nm diamter, made of HBs. Ag Tubular/ filamentous 200 nm long forms: Made of HBs. Ag Complete form/ DANE particle: 42 nm spherical virions Made of HBs. Ag, HBc. Ag, HBe. Ag & partially ds DNA
4 genes –S, C , P, X S- region S- codes for major S S+pre S 2 - codes for M - HBs. Ag S+ pre S 1 and S 2 - codes for L C- region C - C+pre C P - - HBc. Ag - HBe. Ag - DNA polymerase X - enhance HBx. Ag - maybe to exist as coinfection in AIDS, In chronic hepatitis, in hepato-cellular carcinoma
VIRAL ANTIGENS Hepatitis B surface Ag (HBs. Ag) • Australia Ag • Detected in serum Coded by S gene Hepatitis B core • Intracellular core protein Coded by Ag (HBc. Ag) • Not secreted into serum C gene • Found in hepatocytes Hepatitis B pre- • Non particulate soluble Ag Coded by core Ag • Present in circulation Pre C gene (HBe. Ag)
Epidemiologically: 4 serotypes of HBV (HBs. Ag) ‘a’ – group specific antigen ‘d’ or ‘y’ 2 sets of neutrally exclusive epitopes ‘w’ or ‘r’ adw, adr, ayw and ayr are the serotypes ayw- West Asia, Mid-east to West & North India adw- Europe, Australia, Americas adr- South and East India, Far East. ayr- very rare.
Transmission and epidemiology 3 main modes- Blood, blood products, IV drug abuse - Sexual contact - Peri-natally from mother to new born - Very small amount of blood necessary for transmission. Eg. Needle stick injury
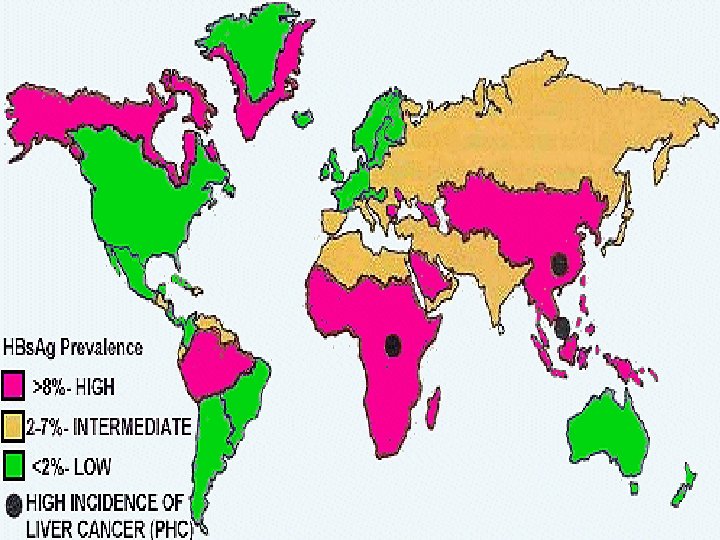
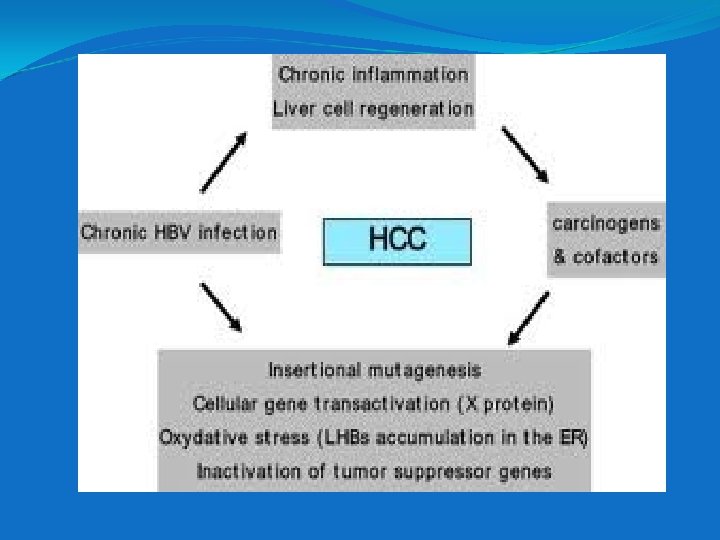
Distribution Worldwide, particularly prevalent in the oriental countries- including India. These areas have high incidence of hepatocellular carcinoma- hepatoma. HBV is a tumor associated virus Immunization against HBV in Taiwan has decreased the incidence of hepatoma. HBV vaccine: first vaccine against human cancer
Mutants- Few cases of Hepatitis B will be with mutant virus Called as pre core mutants – so unable to synthesize HBc. Ag Escape mutants – found in those with combined immunization- also called as ‘a’ antigen mutation. They may pose problem in prophylactic immunization.
PATHOGENESIS OF HEPATITIS B: Why is Hep B virus specific for liver cells? 1. Because virus specific receptor on cell membrane facilitates entry. 2. Transcription factors facilitating viral m. RNA synthesis.
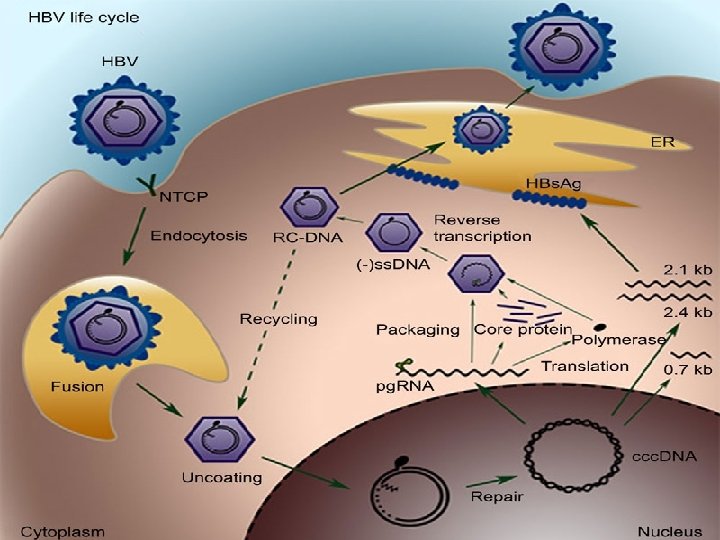
Summary of the Replicative cycle 1. Viral entry- uncoating 2. Viral DNA polymerase synthesize missing portion of DNA 3. Closed ds. DNA formed in nucleus of host cell 4. This DNA will act as template for m. RNA synthesis with help of cellular m. RNA polymerase 5. The m. RNA formed functions for protein synthesis and also template for positive strand of DNA
Next RNA dependant DNA synthesis occurs within the newly assembled virion core in the cytoplasm Hepadna virus are the only virus that produces the genome DNA by reverse transcription with m. RNA as template. (the process is similar but different from process in Retrovirus)
Some of the viral DNA interacts to the host cell genome- so a likely explanation is, that this integrated DNA maintains the carrier state. The progeny HBV with its HBs. Ag envelope is released from the cell by budding through cell membrane It can also infect adjacent cells by intracellular bridges
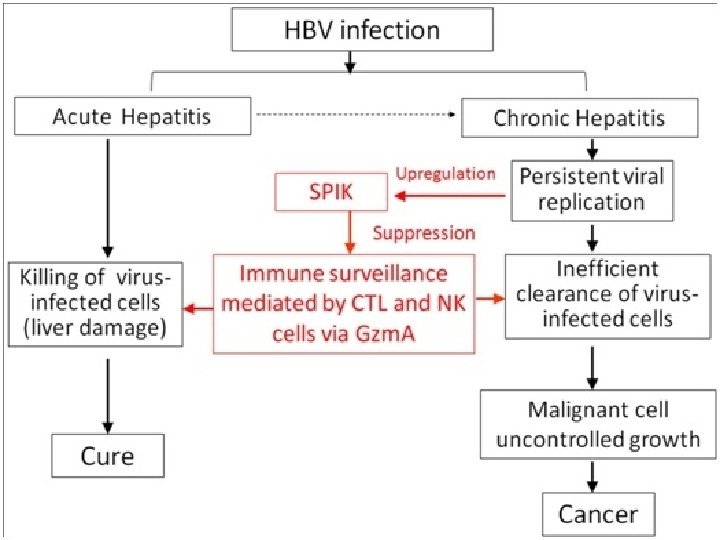
Pathogenesis and immunity Virus enters blood----- infects hepatocytes Viral antigens are displayed on the surface of cells- cytotoxic T cell mount an immune attack against infected hepatocytes- inflammation and necrosis Immune attack mediated by cytotoxic T cell So pathogenesis maybe due to cell mediated immune injury
Direct injury is not seen as we know that HBV show no CPE in lab cell line. Ag-Ab complexes also cause some early symptoms, eg. Arthralgia Complication of chronic hepatitis e. g. Immune complex glomerulonephritis and vasculitis(type III)
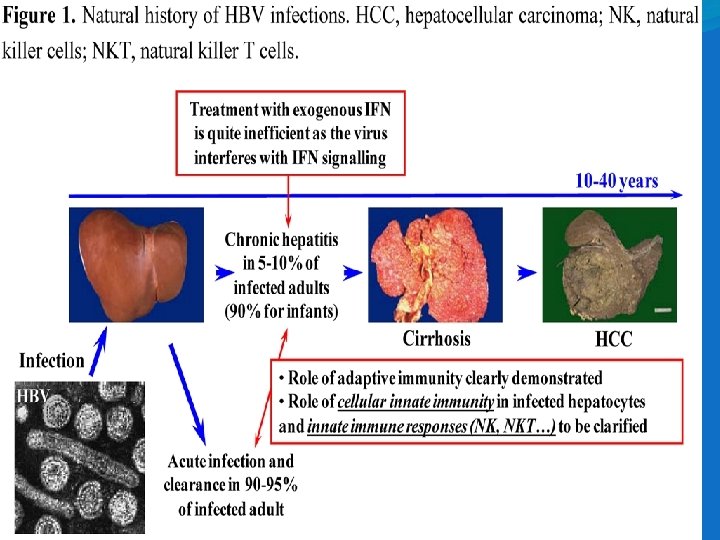
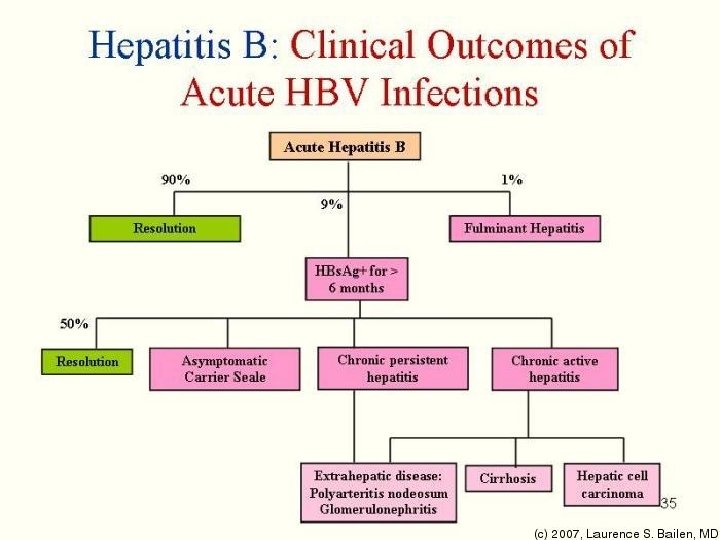
CARRIER STATE 5% of Hep B infection lead to chronic carrier state Chronic carrier is defined as HBs. Ag positivity in the blood for at least 6 months- meaning prolonged presence of HBV and HBs. Ag in blood Reasons- persistent infection of hepatocytes leading to prolonged presence of HBV and HBs. Ag in blood
Adequacy of cytotoxic T cell response i. e. whether a person can clear the infection or become a chronic carrier HBV DNA exists as an episome in the cytoplasm of persistently infected cells. A small no. of copies of HBV DNA is integrated to the host cell DNA. High rate of hepato cellular carcinoma occurs in chronic carriers
HBV genome has no oncogene Carcinoma maybe due to persistent cellular regeneration that attempts to replace the dead hepatocytes or due to insertional mutagenesis. Chronic carriage is more likely if infection is in newborn than adults , as immune system is less competent than in adults 90% of those infected as neonates become chronic carrier
If recovery- life long immunity after natural infection because humoral Ab against HBs. Ag. Antibody to HBc. Ag is not protective.
Clinical findings Mean incubation 10 -12 weeks, much longer than HAV. (3 -4 weeks) 1. Pre-icteric phase: GI symptoms 2. Icteric phase Surrogate markers- Transaminase levels increase, so LFT needs to be performed. Clinical outcome: carrier state or complete recovery
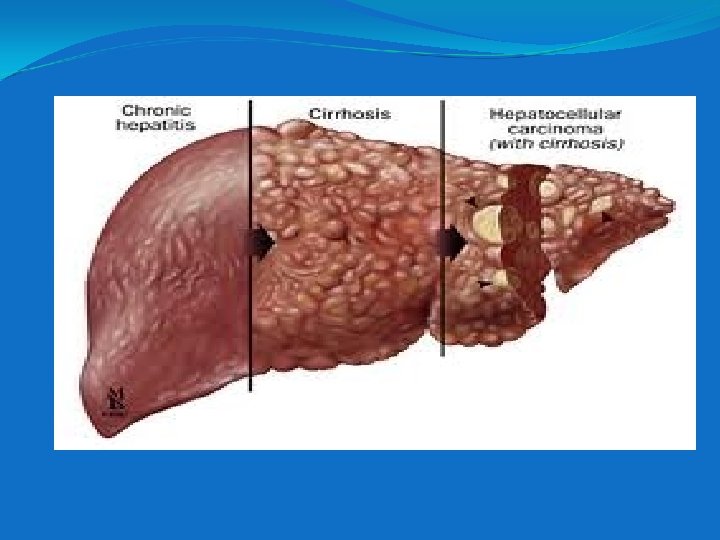
Hepatic complications: fulminant hepatitis or cirrhosis or Hepato-cellular carcinoma Extra-hepatic complications: during prodromal phase: serum sickness like syndrome ( arthritis, rash, angioedema, proteinuria) in 5 -10% patients due to Immune complex deposition.
LAB DIAGNOSIS
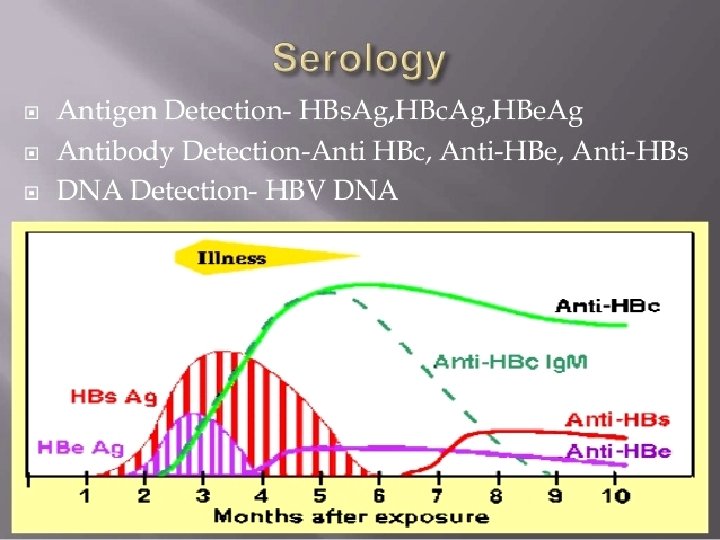
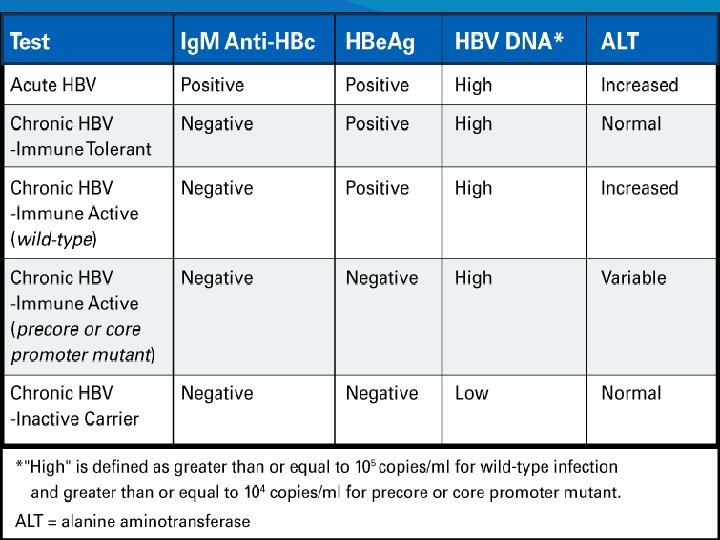
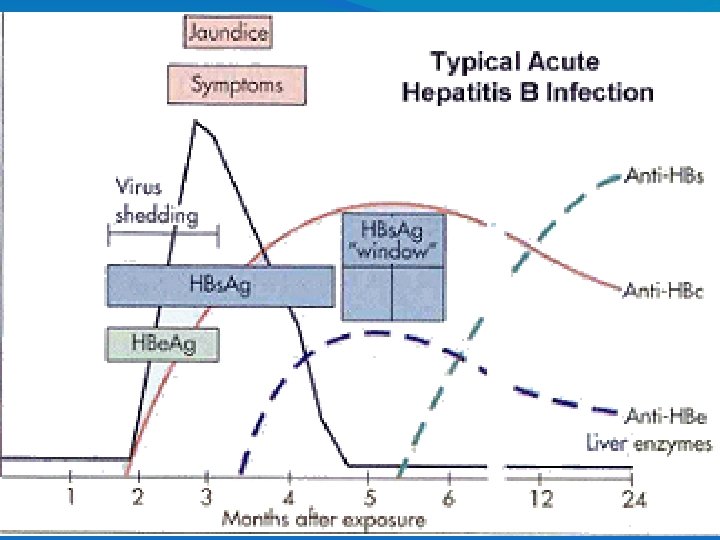
HBs. Ag: First marker to be elevated (8 -12 wks post infection) HBs. Ag- it appears during the incubation period (2 -6 wks before clinical & biochemical evidence of hepatitis) HBs. Ag +ve: indicates active infection Becomes negative in 1 -2 months after jaundice Persisting > 6 mths: carrier state/ chronic hepatitis HBs. Ag: epidemiological marker
HBs. Ab or Anti HBs Corresponding Antibody of HBs. Ag Remains elevated indefinitely Indicates recovery, immunity & non infectivity Only marker of Hep B vaccination
HBe. Ag & HBV DNA Appear shortly after appearance of HBs. Ag in serum Markers of 1. Active viral replication 2. High viral infectivity 3. Present in acute & chronic active hepatitis or super carriers
HBc. Ag: Hidden antigen due to surrounding HBs. Ag Non secretory, hence not detected in blood Detected in hepatocytes by immunoflourescence test
HBc. Ab Ig. M (Anti HBc) First Ab to be elevated following infection Appears within 1 -2 wks following HBs. Ag & persists for 3 -6 mths Indicates acute infection Only marker during WINDOW PERIOD HBc. Ab Ig. G: Appears during late acute stage & remains +ve during chronic & carrier state & recovery Epidemiological marker
Anti HBe. Ab Appear after clearance of HBe. Ag Presence signifies low viral replication & low infectivity
Others – Transaminase levels (LFT) Imaging of liver for evidence of hepatoma etc.
Treatment and prevention 1. Pegylated interferon 2. Nucleoside/ nucleotide analogues- Lamivudine (thiocytadine), tenofovir - inhibit reverse transcriptase of HIV and also effective against HBV. The drugs help to reduce hepatic inflammation and lower levels of HBV in chronic carriers.
Prevention Immunization- Active – vaccine Passive – Immunoglobulins Combined- both
Hepatitis B Vaccine – recombinant subunit vaccine HBs. Ag (vaccine candidate) made in bakers yeast by DNA recombinant technology Indication- those frequently exposed to blood or blood products. E. g – HCW, Patients who require multiple transfusions, dialysis, frequent STDs, drug abuses
-Recommended for all new born and adolescents Dose: 10 -20 ug/dose , 3 doses (0, 1, 6 mths) IM injection Marker of protection: Anti HBs. Ag Ab titre of > 10 IU/ml Booster doses if Ab titre falls
Hepatitis B immune serum (HBIg) High titer of HBs. Ab prepared from sera of patients recovered from Hep B. Provides immediate, passive protection to individuals exposed to HBs. Ag positive blood- e. g. needle stick injury
For needle stick injury both vaccine and HBIg given at separate sites. - for new born whose mother is HBs. Ag positive - immediate HBIg followed by vaccination after delivery. There is immediate and long term protection.
Inactivation -autoclaving (1210 C for 20 mins, 5 lb) -Boiling water 5 mins -dry heat 1800 C for 1 hour. -UV light for 1 minute at 1. 1 watts -formalin 1: 40000 for 3 days at 370 C. Chlorine 10 -15 ppm for 30 mins. -heating food for more than 850 C for 1 min. -surfaces – 1: 100 chlorine bleach.
Non A, Non B Hepatitis Previously described as to those cases of hepatitis in which existing serological tests had ruled out all known causes of hepatitis by viral agents. Nowadays main cause is determined as Hepatitis C virus or HCV. In addition Hepatitis E, Hepatitis D have been described. Cross protection experiments using chimpanzees indicates additional Hepatitis virus exist
HEPATITIS C Hepatitis C virus causes Hepatitis C. Properties Flavivirus, enveloped, genome with ss positive polarity RNA. No RNA polymerase. Multiple serotypes exists. Gene encoding envelope glycoprotein has hypervariable regions similar to HIV.
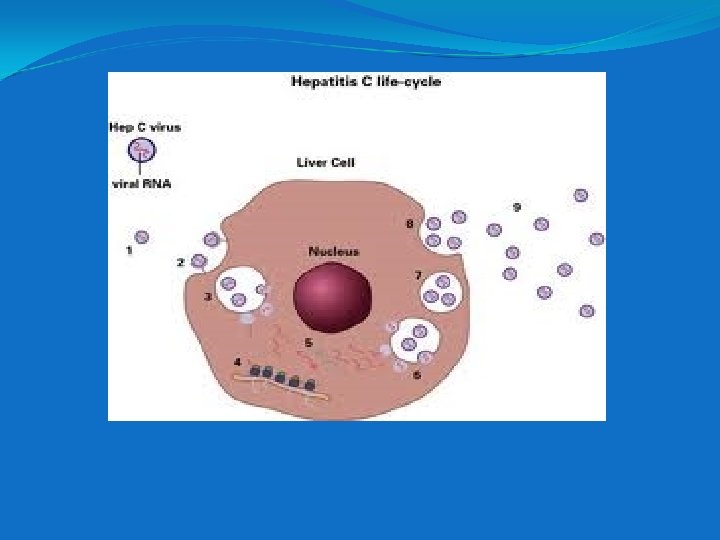
REPLICATION Unclear because not grown in cell culture but Flavivirus usually replicate in cytoplasm and translate their genome RNA into large polyprotein. From this functional proteins are cleaved. So Hep C likely may have similar program of replication
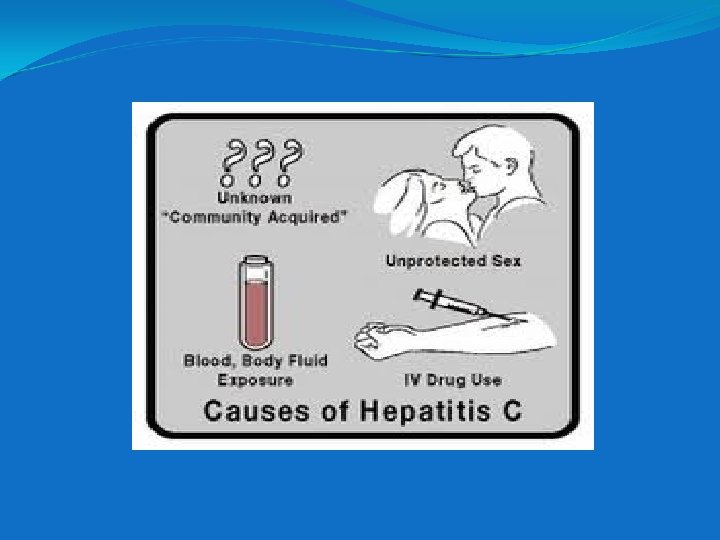
Transmission and epidemiology Humans are reservoirs Modes- blood, sexually, mother to child. Uncertainty exists whether maternal transmission is through placenta or during birth. No evidence of insect vector unlike other Flavi virus e. g. yellow fever is transmitted by mosquito. (also infects liver)
1% donors in USA have antibodies against HCV. In India unknown. People with addiction to IV drugs infected commonly. Commonly preparation of Immunoglobulin is generally safe. But instances of transmission of HCV recorded This is one example of infection transmitted by immunoglobulin
Pathogenesis and immunity Primarily HCV infects hepatocytes No evidence of CPE of liver cells Death of hepatocytes caused by immune attack mediated by cyto T cell No evidence of oncogene in viral genome or their insertion into cancer cell DNA. Still it strongly predispose to hepatocellular carcinoma.
Antibody to HCV is made 75% of patients are chronically infected. They also produce virus for years. Chronic carriage of HCV is higher than HBV. 10% cases go in for chronic active hepatitis and cirrhosis Those who clear the infection in them there is no evidence whethere is re-infection or life long immunity.
Clinical findings Appears milder than HBV Fever, nausea, anorexia, vomiting, jaundice- common Dark urine, pale faeces, increase transaminases levels seen It resembles HBV in predisposing hepatocellular carcinoma or chronic liver disease Chronic carrier state occurs like in HBV
Many infections are asymptomatic detected by presence of antibody Mean incubation period in 8 weeks.
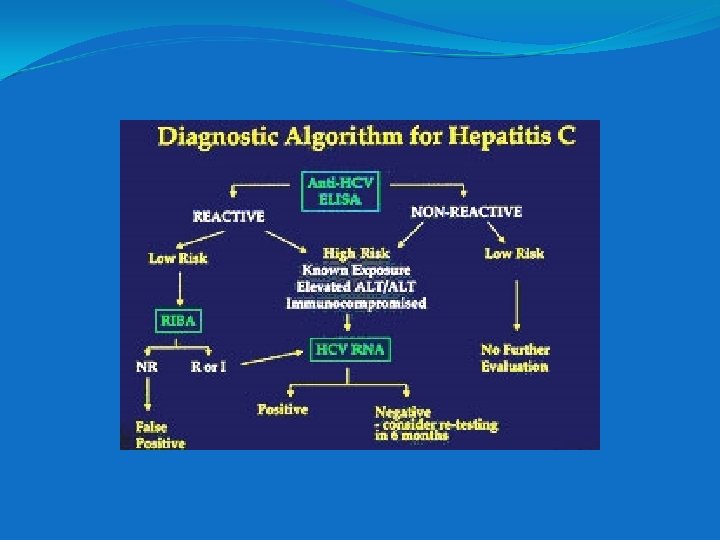
Lab diagnosis Detection of Ab HCV by ELISA Ag used is a recombinant protein formed from 3 immunological stable HCV protein Envelope is highly variable antigen so not included. This ELISA test does not distinguish Ig. M or Ig. G Many cases of false positive occur.
So confirm by RIBA (Recombinant Immuno Blot Assay)
If RIBA is positive further confirmation by PCR based test to detect viral RNA in serum. It also detects active disease exists or not Isolation of virus is usually not done. Prophylaxis- General, blood screening No vaccine Treatment- α interferon doubtful Ribovarin
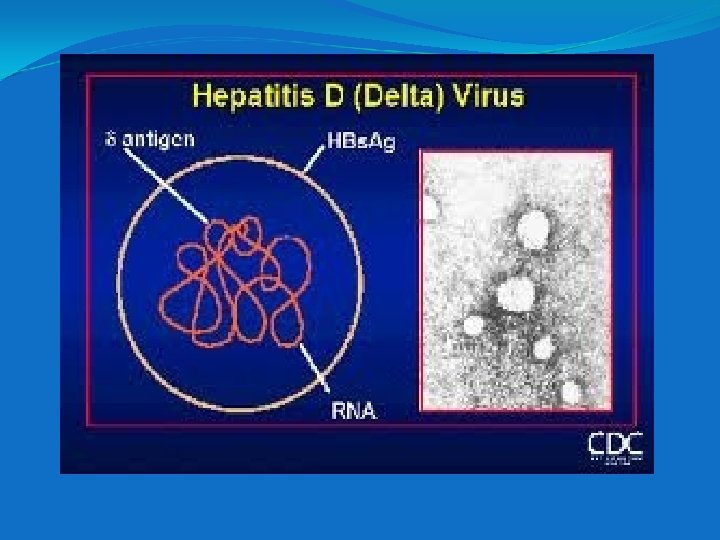
Hepatitis D Causes Hepatitis D or Delta Hepatitis. Rizetto and colleagues isolated it first Properties- Unusual virus because it is a defective virus It cannot replicate by itself as it has no genes for envelope HDV replicates in cells which is infected by Hep B virus.
It uses the HBs. Ag as its envelope protein HBV is helper virus for HDV is enveloped virus with RNA genome. (ss negative polarity, covalently closed circle) RNA genome is small encodes one protein only. This protein is the internal core protein called delta antigen. HDV genome has no sequence homology to HBV genome DNA. HDV has no virion polymerase.
Genome RNA is replicated and transcribed by host cell RNA polymerase. HDV genome RNA is a Ribozyme i. e. it has ability to self cleave and self ligate which is useful in replication of the genome. HDV replicates in the nucleus. But specific replication is complex HDV has one serotype as HBs. Ag is one serotype
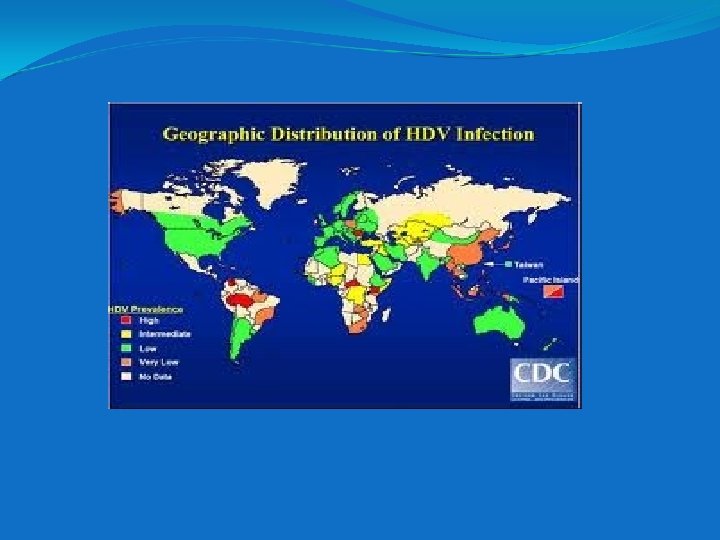
There is no existence of animal reservoir. Transmission and Epidemiology Same as HBV. IV drug abusers mostly infected distribution similar to HBV and is worldwide.
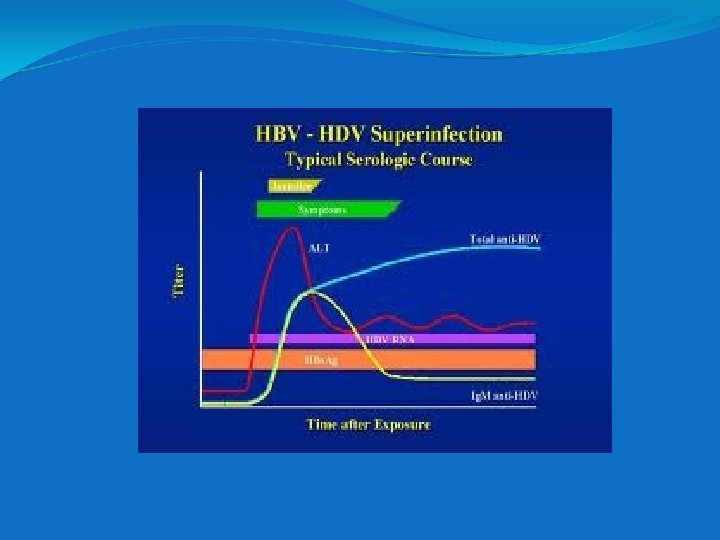
But in a chronic carrier with HBV super-infected with HDV has a significantly higher case of severe, fulminant, life threatening liver failure. Lab Diagnosis-detecting delta antigen or Ig. M antibody to delta antigen in patient’s serum by PCR and ELISA respectively.
Pathogenesis and immunity Likely that pathogenesis is same as HBV. Damage due to cytotoxic T cell Some evidence suggesting delta agent is cytopathogenic to hepatocytes is there. Ig. G Ab to delta antigen is not detected for long periods after infection. So it is uncertain whether long term immunity to HDV exists.
Clinical features Hepatitis delta can occur only in persons infected with HBV. Since it replicates only in hepatocytes also infected with HBV. The person can be infected with both HDV and HBV – co-infected. Or infected previously with HBV then with HDV – super-infected. Co-infection is more severe than with HBV alone. Incidence of chronic hepatitis is the same.
Treatment α- interferon can mitigate some of the chronic hepatitis by HDV, but does not eradicate the chronic carrier state. No specific anti-viral therapy, no vaccine. But people immunised against Hepatitis B are protected.
HEPATITIS E Major cause of enterically transmitted Hepatitis. Common cause of water-borne epidemics in Asia, Africa, India and Mexico. There was an outbreak in New Delhi in 1955
HEV is non-enveloped, ss. RNA tentatively classified as Calcivirus.
Clinically resembles Hep A Exception is, it has a high mortality rate in pregnant women. Chronic liver disease does not occur. There is no prolonged carrier state.
Tests for HEV not readily available. So diagnosis typically made by excluding HAV and other causes There is no antiviral treatment. IEM of faeces, bile can be done. ELISA Ig. M, Ig. G can also be done.
HEPATITIS G It was first isolated in patients with post-transfusion hepatitis in 1996. HGV is member of Flavivirus family like HCV. But unlike HCV, HGV is not known to cause acute hepatitis and chronic active hepatitis and predisposes to hepatocellular carcinoma. HGV role in causation of liver disease is not yet established.