HEMOSTASIS BLOOD PRODUCTS AND BLOOD TRANSFUSION RAKAN TELFAH

HEMOSTASIS, BLOOD PRODUCTS, AND BLOOD TRANSFUSION RAKAN TELFAH

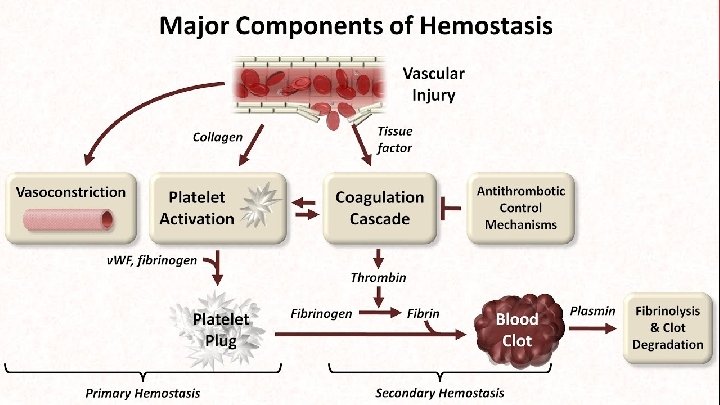
HEMOSTASIS Is a process to prevent and stop bleeding, meaning to keep blood within a damaged blood vessel (the opposite of hemostasis is hemorrhage).
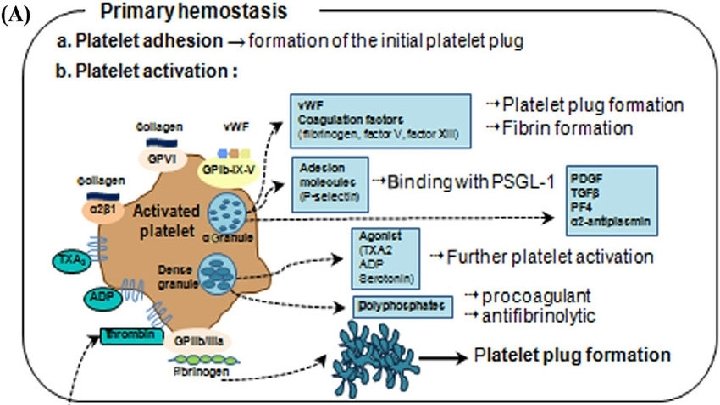

Red blood cells appear to play an important role in platelet adhesion and aggregation, potentially because of their physical capability to facilitate platelet transport to the surface. Therefore, adequate function of primary hemostasis is dependent on a sufficiently high hematocrit

membrane-associated glycoprotein that is not in contact with the blood under physiological circumstances **present at subendothelial sites.

fibrinolysis by various stimuli, including hypoxia and acidosis, as may occur during thrombotic occlusion. By protein C present in endothelial cells

● So An imbalance between activators and inhibitors of the fibrinolytic system, resulting in a net antifibrinolytic state, may contribute to the development of thrombosis ● The efficacy of postoperative pneumatic calf compression may be based not only on rheological advantages in the venous circulation but also result from the enhanced release of plasminogen activators from the vessel wall upon compression (and venous occlusion), thereby compensating for this fibrinolytic imbalance.

NATURAL ANTICOAGULANT MECHANISMS :

NATURAL ANTICOAGULANT MECHANISMS : ● ● Activation of the coagulation system is regulated at various points. Inhibition of the tissue factor–factor VIIa complex may occur by the action of tissue factor pathway inhibitor (TFPI), a surface-associated protease inhibitor. ● Further regulation takes place by the protein C system. Activated protein C, assisted by its essential cofactor (protein S), proteolytically degrades the important cofactors V and VIII. Activated protein C is formed upon activation of circulating protein C by the endothelial cellbound enzyme thrombomodulin in association with thrombin. Hence, thrombin not only plays a pivotal role in coagulation activation but is also involved in the inhibition of blood coagulation. Both protein C and protein S are vitamin K-dependent proteins. ● A third inhibitory system is formed by antithrombin III: This serine protease inhibitor forms complexes with thrombin and factor Xa, thereby losing their coagulant activity. >>The inhibitory action of antithrombin III on thrombin and factor Xa is strongly amplified in the presence of heparin. ● A situation in which there is normal functional protein C but an impaired sensitivity of factor V to protein C is called activated protein C resistance (APC resistance) and is caused by a point mutation in factor V (factor V Leiden). The prevalence of this mutation is about 3% to 5% in the general population and may account for about 30% of all idiopathic venous thromboembolism.
 History 2) Physical examination Investigations: Pre OP clinics These are done for")
Approach: 1) History 2) Physical examination Investigations: Pre OP clinics These are done for etiological Factors in bleeding LABORATORY MONITORING OF BLEEDING AND COAGULATION: Peripheral platelet count: at least should be 30 to 50 *10 ^9. Counts of less than 10, 000 μL are dangerous and may lead to spontaneous bleeding as bleeding from the urinary system, GI, or from any simple trauma there will be bleeding from the skin. [These are signs of platelets problem]

Prior to surgery, platelet count should be raised depending on the site of surgery. Ex. surgery on gallbladder you can do the surgery even if the platelet count was 50, 000 μL while if going to work on tonsils you must be sure that the platelets count is high. Thrombocytosis is diagnosed when count is more than 500, 000 μL

BLEEDING TIME usually shorter than 8 minutes if prolonged : low plasma level of v. WF /IX /V use of antiplatelets drugs [Aspirin] presence of lupus-like antibodies platelet functional impairment. Fibrinogenemia.

COAGULATION TESTS: Coagulation tests must be performed on plasma rather than serum, because clotting factors are removed during serum preparation along with the clotted cellular elements. PT [Prothrombin Time] (extrinsic system) Factor VII (11 -13 seconds). monitoring of warfarin treatment. • INR = [Patient PT ÷ Control PT]ISI Unlike the PT, the results of the INR will be similar on a blood sample tested in any laboratory using any thromboplastin reagent/instrument system when calibrated correctly

USES OF THE PT/INR Clinical uses of the PT include the following: ●Evaluation of unexplained bleeding ●Diagnosing disseminated intravascular coagulation ●Obtaining a baseline value prior to initiating anticoagulation ●Monitoring warfarin therapy ●Assessment of liver synthetic function
![PTT [Partial Thromboplastin Time] (intrinsic pathway) Factors XII, XI, IX, VIII (25 -35 seconds).](http://slidetodoc.com/presentation_image_h2/7dd74ea4221d05771a8f9d79dcc13443/image-16.jpg "PTT [Partial Thromboplastin Time] (intrinsic pathway) Factors XII, XI, IX, VIII (25 -35 seconds).")
PTT [Partial Thromboplastin Time] (intrinsic pathway) Factors XII, XI, IX, VIII (25 -35 seconds).

USES OF THE APTT Clinical uses of the a. PTT include the following: ●Evaluation of unexplained bleeding ●Diagnosing disseminated intravascular coagulation (DIC) ●Monitoring therapy with unfractionated heparin ●Monitoring therapy with parenteral direct thrombin inhibitors “dabigatran” Of note, low molecular weight (LMW) heparins often do not prolong the a. PTT.

While the PT and a. PTT provide an overall assessment of clot formation, they do not provide information about fibrin cross linking or clot dissolution and will thus be insensitive to abnormalities of factor XIII function or abnormal fibrinolysis.

READING RESULTS normal PT and PTT, --- vessels or platelets. PT and PTT are prolonged, --- common pathway PTT is prolonged and PT is normal, --- intrinsic pathway Prolonged PT and normal PTT --- factor VII
. defect in clotting mechanism (hereditary/")
BLEEDING DISORDERS Vascular defect platelet defect (thrombocythemia/ thrombocytopenia/ thrombasthenia). defect in clotting mechanism (hereditary/ acquired).

DIC: Disseminated Intravascular Coagulation, or Acquired Hypofibrinogenemia Systemic activation of coagulation pathways Excessive Thrombin generation • Diffuse microthrombi • Consumption and depletion of Platelets and coagulation factors • Classic picture of diffuse bleeding DIC Diagnosis: • The presence of inciting underlying pathology • Low Platelets • Prolonged PT/PTT • Low Fibrinogen levels • high FDPs. Measurement of fibrinogen is commonly performed but has shown to be of no value for the diagnosis of DIC, especially because the acute-phase reactant properties of fibrinogen in many clinical situations may completely obscure ongoing fibrinogen consumption. DIC Treatment: • Relieving inciting factor • Adequate perfusion • FFP • Cryoprecipitate, Platelets and/or Factor supplements.

most common cause + strong predictor of death
………")
COAGULOPATHY OF LIVER DISEASE • Prolonged PT • Thromboses (protein C and S deficiency)……… disturbance in the balance between procoagulant and anticoagulant pathways…. both increased bleeding risk and increased thrombotic risk thrombocytopenia and impaired humoral coagulation function manifested as prolongation PT/INR • . The etiology of thrombocytopenia in patients with liver disease • 1) hypersplenism • 2) reduced production of thrombopoietin • 3) immune-mediated destruction of platelet

● Platelet transfusions are the mainstay of therapy; however, the effect typically lasts only several hours…. risk of antibodies ● ● administration of interleukin-11 (IL-11), a cytokine that stimulates proliferation of hematopoietic stem cells and megakaryocyte progenitors. (cancer patient and cirrhotic patient) splenectomy or splenic embolization to reduce hypersplenism. (less used)
 acidosis >> decrease o 2 supplement •")
COAGULOPATHY OF TRAUMA due to • 1) acidosis >> decrease o 2 supplement • 2) hypothermia, • 3) dilution of coagulation factors.

• Local Hemostasis : • Digital pressure • Tourniquet • Packing • Biological agents that help platelets adhesion
 bleeding who undergo")
PRO HEMOSTATIC AGENT in patients with : coagulation defects severe (postoperative) bleeding who undergo procedures known to be associated with major blood loss • PLATELETS, PLASMA, AND COAGULATION FACTOR.
. After")
PLATELETS usually contain a mixture of the platelet from six donors (6 units). After platelet transfusion, the platelet count should rise by at least 5*10^9 /l per unit of platelets transfused. Indications: Amegakaryocytic thrombocytopenia, Drug or radiation induced hypoplasia, functional platelet abnormalities, viral diseases associated with thrombocytopenia e. g. Dengue, Disseminated intravascular coagulation. Dengue 1. platelet consumption during ongoing coagulopathy process 2. activation of the complement system 3. increased peripheral sequestration

FRESH FROZEN PLASMA plasma separated from whole blood donation within 6 hours and then rapidly frozen to – 25°C or colder, shelf life up to 1 year contains factor VIII, factor IX, v. WF and other clotting factors. Fibrinogen Dosage: Initial dose of 15 ml/kg. Labile coagulation factors rapidly degrade; use within 6 hours of thawing. Indications: -

CRYOPRECIPITATE Storage: At – 25°C or colder for up to 1 year Must be infused within 6 hours of thawing Each unit of Cryo raises Factor VIII by 2%, to achieve plasma factor VIII rise of 20%, 10 units/kg have to be infused. Indications: in the treatment of inherited deficiencies of von Willebrand Factor (von Willebrand’s disease) / Factor VIII (haemophilia A) / Factor XIII As a source of fibrinogen in acquired coagulopathies: e. g. disseminated intravascular coagulation (DIC)
 factor")
SPECIFIC FACTORS “PURIFIED CONCENTRATES” factor VIII in (hemophilia A and von Willebrand’s disease) factor IX in (hemophilia B or Christmas disease) In general, activity levels should be restored to 30% to 40% for mild hemorrhage, 50% for severe bleeding, and 80% to 100% for lifethreatening bleeding.

INDICATIONS OF BLOOD TRANSFUSION : In general , blood loss or low hemoglobin. • 1) Improvement in Oxygen-Carrying Capacity. • 2) Treatment of Anemia • 3) Volume Replacement


BANKED WHOLE BLOOD ● shelf life of red blood cells is now 42 days. ● The changes in the red blood cells that occur during storage include reduction of intracellular ADP and 2, 3 -diphosphoglycerate (2, 3 DPG), which alters the oxygen dissociation curve of hemoglobin, resulting in a decrease in oxygen transport ● Stored RBCs progressively becomes acidic with elevated levels of lactate, potassium, and ammonia. ● Whole blood is only indicated for the treatment of acute hemorrhage.

RED BLOOD CELLS AND FROZEN RED BLOOD CELLS ● Red blood cells are the product of choice for most clinical situations requiring resuscitation. ● Concentrated suspensions of red blood cells can be prepared by removing most of the supernatant plasma after centrifugation. ● not currently available for use in emergencies, as the thawing and preparation time is measured in hours. ● The red blood cell viability is improved, and the ATP and 2, 3 -DPG concentrations are maintained. ● The preparation reduces but does not eliminate reactions caused by plasma components.

HAZARDS OF TRANSFUSION • 10% of all transfusions • Less than 0. 5% are serious • Non hemolytic reactions • 1% • Rise in Temp. more than 1 C ……………antibodies directed against donor leukocytes and HLA antigens • Bacterial contamination • Allergic reactions • Respiratory(TACO). . Transfusion-associated circulatory overload • TRALI • Hemolytic reactions



IMMEDIATE HEMOLYTIC TRANSFUSION REACTION: ABO incompatibility Fatal in 6% of cases Hemoglobinemia and Hemoglobinuria (usually acidic ) Deaths occur from DIC and acute renal failure
![Clinical presentation in Immediate hemolytic reaction: [in order] Burning sensation at the transfusion site](http://slidetodoc.com/presentation_image_h2/7dd74ea4221d05771a8f9d79dcc13443/image-41.jpg "Clinical presentation in Immediate hemolytic reaction: [in order] Burning sensation at the transfusion site")
Clinical presentation in Immediate hemolytic reaction: [in order] Burning sensation at the transfusion site followed by Anxiety, Chest pain (tightness), Back pain, headache, Dyspnea, Rigors [Chills], Vomiting, Diarrhea, Restlessness, Tachycardia, Hypotension, Shock.

Treatment: 1. Stop transfusion immediately. 2. Give Hydrocortisone 100 -200 mg I. V. 3. Anti-histamine (chlorpheneramine 10 mg) I. V. 4. Intravenous fluid to maintain the blood volume and urinary flow. 5. In case of intravenous coagulation give Heparin.

DELAYED HEMOLYTIC TRANSFUSION REACTION: Occurs 1 -3 weeks after transfusion. Clinical presentation in Delayed hemolytic reaction: Patient comes with Urticaria [due to Plasma proteins] esp. in people with Ig. A deficiency, jaundice, fever, anemia, arthralgia and myalgia [muscle pain]. Treatment: None in required just observation.



MASSIVE BLOOD TRANSFUSION ● It is most often defined as the need to transfuse the patient’s total estimated blood volume in less than 24 h, or one-half the patient’s total estimated blood volume in 1 h. For most adult patients, the total estimated blood volume is the equivalent of 10 to 20 units. The approach to massive transfusion (and to lesser degrees of transfusion) elucidates that the outcomes have improved with concurrent transfusion of (packed red cells, FFP, and platelets) to avoid dilutional coagulopathy ……. . (1: 1: 1)

THANK YOU
- Slides: 47