Hemodynamics II When The Waves Dont Look Right





































 (Pv sat – Pa sat)")
 (100% – 87%) 2. 56 * MV sat")

- Slides: 41
Hemodynamics II … When The Waves Don’t Look Right … Chris Pan, MD. MBA. MS. Interventional Cardiology University of California, Irvine
Disclosures None
Content • Valvular heart disease o Aortic disease o Mimicker of aortic stenosis o Mitral disease • Pericardial disease o Constrictive vs Restrictive • Intracardiac shunt
LHC + RHC measurement • RHC: chamber pressure, cardiac output, valve area • LVEDP: Fluid status / HF • LV-Ao measurement: Aortic disease • LV-PCWP measurement: Mitral disease • LV-RV response: Pericardial disease • Saturations: intracardiac shunt
Case 1 70 M presented with shortness of breath • Diastolic murmur along sternal border • Visible strong carotid pulse • Head bobbing
Ren X , Banki N M Circulation 2012; 126: e 28 -e 29
Wide Pulse Pressure Aortic tracing Ren X , Banki N M Circulation 2012; 126: e 28 -e 29 LV tracing
Rapid Rise of LV Diastolic Pressure Aortic tracing Ren X , Banki N M Circulation 2012; 126: e 28 -e 29 LV tracing
Near Equalization of Diastolic LV and Ao Aortic tracing Ren X , Banki N M Circulation 2012; 126: e 28 -e 29 LV tracing
Aortic Regurgitation Key Hemodynamic Findings: • Wide pulse pressure: High systolic +Low diastolic AO • Rapid rise in LV diastolic pressure • LVEDP ~ AOEDP • LVEDP is much higher than PCWP (esp. in acute AR)
Case 2 70 M presented with shortness of breath Cath findings: • Normal coronary arteries • LVgram: EF ~ 30%
WWYD? 70 M with SOB, normal coronary arteries, depressed EF, and aortic stenosis with aortic gradient ~ 30 mm. Hg • Right heart catheterization • Re-cross aortic valve to measure gradient with a Langston dual lumen catheter • Determine the true severity of the aortic stenosis o Pseudo aortic stenosis (2/t low flow or gradient) vs o True fixed aortic stenosis
Ao. V Area Formula Gorlin Formula: Hakki Formula
Moderate or Severe AS? Valve Replacement? P-P gradient 30 mm. Hg CO = 3. 2 l/m Fick AVA = 0. 7 cm 2
Dobutamine Challenge True fixed stenosis Nishimura R A , Carabello B A Circulation 2012; 125: 2138 -2150 vs Pseudo variable stenos
Dobutamine Challenge Base 10 Dob+Pace 80 20 Dob + Pace 95
S/p Aortic valvuloplasty … What happened? AS AR
Case 3 70 M presented with shortness of breath Cath findings: • Normal coronary arteries • Normal ejection fraction
Aortic Stenosis?
Still Aortic Stenosis? Distal LV Sub-Aortic
Spike & Dome
Hypertrophic Cardiomyopathy Nishimura R A , Carabello B A Circulation 2012; 125: 2138 -2150
Brockenbrough-Braunwald-Morrow Sign AS 1. Decreased arterial pulse pressure 2. Increased systolic peak gradient HCM Nishimura R A , Carabello B A Circulation 2012; 125: 2138 -2150 3. Spike and Dome
Case 4 70 M evaluated for shortness of breath • Admitted for inferior STEMI s/p DES to mid RCA • Developed acute HF symptoms and new systolic murmur 24 hrs after PCI
Large V wave
Large V wave Definition: • Peak V wave > 40 mm. Hg • Peak V wave – PCWP > 10 mm. Hg • Peak V wave : PCWP > 2 Etiologies: • Sudden increase of LA pressure/volume o o Acute MR (from ruptured chordae): 3 x > normal Septal defects Hypervolemia Atrial infarction
Case 5 70 M evaluated for shortness of breath Cath findings: • Normal coronary arteries • Normal ejection fraction
Mitral Stenosis
Mitral Stenosis • Commonly measured by simultaneous LV and PCWP pressures • Often overestimate the true transmitral gradient o Delay in transmission of the change in pressure contour o Phase shift o Heart rate
Overestimate Mitral Stenosis Nishimura R A , Carabello B A Circulation 2012; 125: 2138 -2150
Overestimate Mitral Stenosis Rogers, J. “Hemodynamics in the Cath Lab: A Forgotten Art? ”
Case 6 70 M evaluated for shortness of breath • Lung cancer on chemo-radiation therapy • Recurrent pericardial effusion
Which Tracing Requires Pericardiocentesis? A. B. https: //thoracickey. com/5 -the-atrial-waveform/
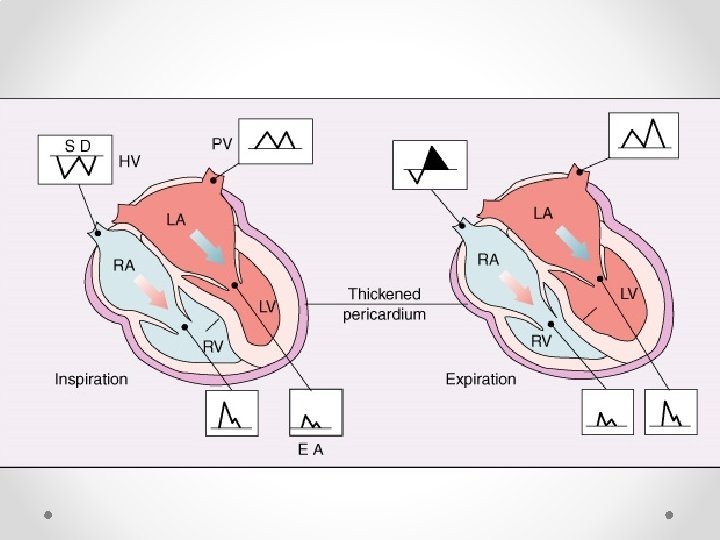
B. Tampondade vs Constrictive Pericarditis http: //www. brown. edu/Courses/Bio_281 -cardio/handout 6 c. htm
Constrictive Restrictive LV RV
Case 7 Does he need ASD repair ? 70 M evaluated for shortness of breath • Known ASD • Saturations: SVC: 68% IVC: 63% RA: 65% RV: 87% PA: 87% FA: 100% PV: 100%
L R shunt: • ASD VSD PDA • RV failure R L shunt: • To. F Eisenmenger’s Transposition • Hypoxia
Shunt Calculation Qp Qs (Ao sat – Mv sat) (Pv sat – Pa sat) • Mv sat = (3 SVC + IVC) / 4 • Pulm vein sat = LV O 2 sat if shunt exists • Qp/Qs > 2 = severe shunt = repair • Qp/Qs < 1 = R L shunt = irreversible = no repair
Qp Qs (100% – 66. 75%*) (100% – 87%) 2. 56 * MV sat = (3 x 68% + 63%) / 4 = 66. 75% SVC: 68% IVC: 63% RA: 65% RV: 87% PA: 87% FA: 100% PV: 100%
Questions & Comments THANK YOU