Hemodialysis Back to the basic Department of Nephrology

Hemodialysis - Back to the basic Department of Nephrology R 1 이해경

Introduction • Cause of ESRD – – – DM : 55% HTN : 33% Glomerulonephritis Polycystic kidney disease Obstructive uropathy • Mortality rate on dialysis : 18– 20%/year • 5 -year survival rate : 30– 35% • Cause of deaths – Cardiovascular diseases(50%) – Infections (15%)

Criteria for Dialysis • Uremic symptoms • Hyperkalemia unresponsive to conservative measures • Persistent extracellular volume expansion despite diuretic therapy • Acidosis refractory to medical therapy • Bleeding diathesis • Creatinine clearance or estimated GFR<10 m. L/min per 1. 73 m 2
 • Peritoneal dialysis –")
Dialysis options • Hemodialysis – Most common for ESRD (>90%) • Peritoneal dialysis – Continuous – Less efficient in solute clearance • Outcomes of both therapies are similar in most reports • Decision is based on personal preferences and quality-of-life considerations

Principle • Diffusion • Ultrafiltration • Convection

Diffusion • Solute proceeds down a concentration gradient • Occurs via pores located within fiber of dialysis membrane • Blood & dialysate flow in opposite direction → maintain concentration gradient • The larger, the slower its rate of transfer across the membrane • Small molecule(ex. Urea) → substantial clearance • Larger molecule(ex. Creatinine) is cleared less efficiently

Ultrafiltration • Fluid removal via hydrostatic pressure gradient across the membrane generated by the dialysis machine • Blood : High pressure • Dialysate : Low pressure • Coefficient correlates directly with membrane permeability

Convection • Solutes are dragged along with fluid • High rate of fluid transport from blood to dialysate

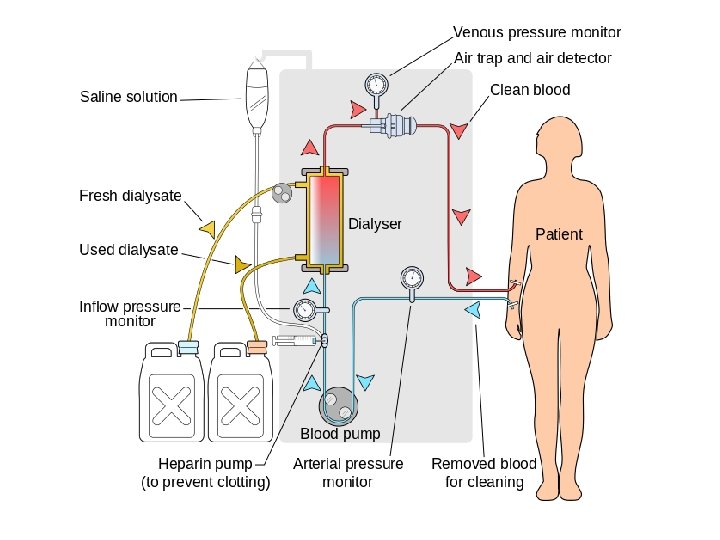
Three essential components • Dialyzer • Dialysate • Blood delivery system

Dialyzer • Plastic chamber • Perfuse blood and dialysate simultaneously at very high flow rates • Bundles of capillary tubes through which blood circulates while dialysate travels on the outside of the fiber bundle • Dialysis membranes – cellulose, substituted cellulose, cellulosynthetic, synthetic – Synthetic membranes • more biocompatible • absence of these hydroxyl groups

Dialysate • K : 0 to 4 mmol/L • Ca : 1. 25 mmol/L 2. 5 meq/L (e. g. , hypocalcemia) • Na : 140 mmol/L • Water of dialysate is subjected to filtration, softening, deionization, reverse osmosis • Reverse osmosis – Water is forced through a semipermeable membrane at very high pressure – Remove microbiologic contaminants and >90% of dissolved ions

Dialysate contamination • Aluminum – Outbreak of dementia in dialysis patient → Improved methods of water purification • Copper&Chloramine – Hemolytic anemia → Carbon tank • Bacteria – Membrane provides physical barrier – Dialysate dose not have to be completely sterile – Maximum level for bacteria : 200 CFU/m. L(AAMI) or 100 CFU/m. L(EPS) • Endotoxin – High efficiency dialysis membrane – Bicarbonate containing dialysate

Blood delivery system • Extracorporeal circuit in the dialysis machine • Dialysis access • Blood pump moves blood from the access site, through the dialyzer, and back to the patient • Negative hydrostatic pressure on the dialysate – To achieve ultrafiltration • Monitors pressure, temperature, conductivity, flow of dialysate

Dialysis access • Fistula – Fistula first – Not mature sufficiently to provide reliable access to the circulation – Thrombose early – Brachiobasilic fistula with transposition of basilic vein fistula to the arm surface have increased • Graft – Smaller-caliber veins – Damaged by repeated venipuncture – Thrombosis : The most important complication of AV grafts – Much higher rates of infection than fistula

Dialysis access • Intravenous large-bore catheters – Tunnel reduces bacterial translocation from the skin → Infection ↓ – Most placed in the internal jugular veins – Avoid placement in the subclavian veins • Subclavian stenosis • Prohibit permanent vascular access in the ipsilateral extremity

Complication • Hypotension • Muscle cramp • Anaphylactoid reaction

Hypotension • Most common acute complication • Particularly with diabetes mellitus • Excessive ultrafiltration with inadequate compensatory vascular filling • Impaired vasoactive or autonomic responses • Overzealous use of antihypertensive agents • Reduced cardiac reserve
, 23% saturated")
Hypotension • Management – Discontinue ultrafiltration – Isotonic saline(100 -250 m. L), 23% saturated hypertonic saline(10 m. L), salt-poor albumin – Careful evaluation of the dry weight – Ultrafiltration modeling • More fluid is removed at the beginning rather than the end of the dialysis – Avoid heavy meals during dialysis – Midodrine, a selective alpha-1 adrenergic pressor agent

Muscle cramp • Etiology : obscure – Excessively aggressive volume removal – Use of low-sodium–containing dialysate • Prevention – Reduce volume removal during dialysis – Ultrafiltration profile – Higher concentrations of sodium in the dialysate

Anaphylactoid reaction • Type A reaction – Ig. E-mediated reaction to ethylene oxide – Occurs soon after the initiation of a treatment – Severe symptom → Steroid or epinephrine • Type B reaction – Nonspecific chest and back pain – Result from complement activation and cytokine release – Resolve over time with continued dialysis
 – T =")
Dialysis adequacy • Kt/V – K = Dialyzer clearance(ml/min or L/hr) – T = Time(min or hr) – V = Distribution volume of urea(ml or L) – – – =-ln(R-0. 008 Xt) + (4 -3. 5 XR)X 0. 55 XUF/W R = postdialysis BUN/predialysis BUN UF = Ultrafiltration volume in liters W = Patient postdialysis weight >1. 2 or 1. 05 • URR(Urea reduction ratio) – =100 X(1 -postdialysis BUN/predialysis BUN) – >65 -70%

References • Harrison 18 th • Uptodate – Overview of the hemodialysis apparatus – Kt/V and the adequacy of hemodialysis – Contaminants in water used for hemodialysis
- Slides: 23