Hemiplegic Shoulder Pain Update Andrew E Kirsteins M
")
- Focus on Post stroke �Diagnosis")







, Ph. D, Tom Fahey,")
")

 1036")







 �>3")
")

 find that HSP more common in")



 clinical diagnostic")


 HSP etiology Zeilig et al Pain. 2013 Feb; 154(2): 263")





 are")


- Slides: 41
Hemiplegic Shoulder Pain Update Andrew E. Kirsteins M. D. FAAPM&R (Sports and Neuromuscular Med) Cone Health Physical Medicine and Rehabilitation
Purpose �Review common causes of Hemiplegic Shoulder Pain (HSP)- Focus on Post stroke �Diagnosis using PE and Imaging Studies �Introduce Musculoskeletal Ultrasound (MSK US) as an aid to diagnosis of HSP �Hands on demo �Please check out Sept 2013 Am L PM&R Ozcakar et al- Utility of MSK US in Rehab settings
Shoulder Pain General Population Post Stroke Population � 3 rd most common MSK c/o in primary MD office � 2 nd most common reason for referral to Ortho/Sports �~70% pain is from Rotator cuff disorders �Occurs in up to 72% stroke pts in the first year-Van Ouwenaller C, Laplace PM, Chantraine A. Painful shoulder in hemiplegia. Arch Phys Med Rehabil. 1986; 67: 23– 26 �Common reason for poor rehab outcome, QOL �Several pain generators have been proposed, complex
Post Stroke Shoulder Pain=HSP �Overall prevalence 17% at 2 wks, 20% at 1 mo, 23% at 6 mo. Ratnasabaphthy et al 2003, Clinical Rehab �Prevalence Rehab pop. 60% @ 4 mo, 35% @ 6 mo
Post Stroke Shoulder Pain Risk Factors �Significant weakness �L neglect �Sensory deficits �Advanced age �Spasticity
Hemiplegic shoulder pain etiology Nociceptive Neuropathic �Subluxation theory �Subacromial Impingement �Bicipital tendon �Spasticity related �Adhesive capsulitis �RSD �Brachial plexopathy �Central Post stroke Pain
Nociceptive Shoulder Pain Hemiplegic Shoulder Pain Update
Does Subluxation Cause HSP? Pro Con �Traction on joint capsule during flaccid stage �Subluxation more common in Shoulder Hand Syndrome- �Most HSP occurs during spastic stage-Van Ouwenwaller et Dursun et al 2000 al 1986 �Neuromuscular Electrical Stim reduces pain but not subluxation- Yu et al �No correlation between pain and subluxation Bohannon et al 1990
Ultrasound measurement of shoulder subluxation X Ray Ultrasound �Xray evaluation requires multiple views, measurements after imaging �Long axis view allows measurement during image acquisition-Park GY, Kim JM, Sohn SI, et al. Ultrasonographic measurement of shoulder subluxation in patients with poststroke hemiplegia. J Rehabil Med 2007; 39:
Subacromial Impingement Syndrome Marwan Alqunaee, RCSI, Rose Galvin, BSc (Physio), Ph. D, Tom Fahey, MD, FRCGPDiagnostic Accuracy of Clinical Tests for Subacromial Impingement Syndrome: A Systematic Review and Meta-Analysis Archives of Physical Medicine and Rehabilitation, Volume 93, Issue 2, February 2012, Pages 229– 236 �Any rotator cuff pathology in the subacromial space �Includes Supraspinatus, Infraspinatus, Teres Minor and Subscapularis �Stages Include �Stage 1 -Bursitis �Stage 2 -Partial Tear �Stage 3 - Full thickness Tear
Sensitivity and Specificity �A Se. Nsitive test when Negative rules OUT=SNNOUT, (true positive identification) �A SPecific test when Positive rules IN=SPPIN’ (true negative identification) �Difficult to establish Sensitivity and specificity in studies if there is no “Gold Standard”, or if different “Gold Standards” are used �So for diagnostic PE or imaging studies either surgical findings or MRI is used as “Gold Standard”
Subacromial Impingement Syndrome=SIS �History- pain with overhead activity, nocturnal pain �Exam-Hawkins Kennedy passive forward flexion/int rotation only useful test in a hemiplegic patient Sensitivity 74% �Imaging- Ultrasound can identify all 3 stages of SIS bursitis, partial tear and full thickness tear
Diagnostic accuracy of Ultrasound for RCT Smith et al, Clin Radiol 66 (2011) 1036 -1048 �Given limitation of history (communication deficit) and exam (given UE weakness), imaging assume greater importance �Partial thickness RCT Sen 84%, Sp 89% �Full thickness RCT Sen 96%, Sp 93%
PHYSICAL FINDINGS AND SONOGRAPHY OF HEMIPLEGIC SHOULDER IN PATIENTS after ACUTE STROKE DURING REHABILITATION-Huang et al J Rehabil Med 2010; 42: 21– 26 Methods Results at D/C �Pain: 68% Poor motor, 35% �N=57, cross sectional Good motor �Good vs Poor Motor groups �US abnormalities Poor based on Brunnstrom Motor- 50% biceps �Excluded prior shoulder tendinopathy, 47% problems Supraspinatus tear, 44% Subacromial bursitis �Recorded pain using VAS-but pain not an inclusion criteria �US abnormalities Good Motor – 30% biceps, 22% �Assessed at admission and subacromial bursitis, 17% discharge (LOS 27 d for supraspinatus good, 32 d for poor motor)
Sonography of Patients with Hemiplegic shoulder pain after stroke Lee et al Am J Roentgen 2009 Feb; 192(2): �n=71, 20 pts had bilateral shoulders scanned �Subacromial bursal effusion seen in 36 shoulders �Biceps tendon sheath effusion in 39 shoulders �Supraspinatus tendinosis (7), partial tear (6) and full tear (2) �Abnormalities more common in hemiplegic shoulder p=. 007 vs uninvolved side
Sonography and physical findings in stroke patients with hemiplegic shoulders: A longitudinal study Ya Ping Pong et al, J of Rehab med 2012, (44), 553 -557 � 76 first time CVA, no hx of shoulder problems �Scanned during acute rehab and at 6 mo �Underwent standard inpt rehab program 1 hour PT and 1 hr OT 5 d/wk �Brunnstrom score, ROM, Ashworth, 10 pt NRS
Sonography and physical findings in stroke patients with hemiplegic shoulders: A longitudinal study Ya Ping Pong et al, J of Rehab med 2012, (44), 553 -557 Acute (D/C from Rehab) Chronic (6 mo post D/C) �Subacromial effusion 30. 3% �Supraspinatus tear 30. 3% �Biceps tendon 39. 5% �Subscapularis 9. 2% �Pain score 2. 71/10 �Subacromial effusion 13. 2% �Supraspinatus tear 40. 8% �Biceps tendon 57. 9% �Subscapularis 22. 4% �Pain score 3. 99/10
Subacromial Bursitis
MRI findings in hemiplegic shoulder pain Shah et al Stroke 2008 June 39(6) �>3 mo since CVA, pain score >4, n=89, 65% L HP �Supraspinatus tear 26% partial, 6% Full �Supraspinatus tendinopathy 51% �Infraspinatus tear 13% partial, 2% Full �Infraspinatus tendinopathy 19% �Subscapularis tear 1% �Teres minor tear 1%
MRI findings in hemiplegic shoulder pain Shah et al Stroke 2008 June 39(6)
Adhesive Capsulitis or Frozen Shoulder �Few imaging studies �X ray Arthrogram Rizk et al, Arch Phys Med Rehabil. 1984; 65(5): 254 -6 �Arthrogram and Exam -Lo et al. , Arch Phys Med Rehabil. 84(12): 1786 -91, 2003 Dec � 32 pt with HSP<1 year post CVA � 30 Patients mean 3 months post CVA, Reduced ROM � 50% had adhesive and pain, electrically silent capsulitis EMG of shoulder muscles � 22% Rotator cuff tears � 23/30 had reduced � 16% Shoulder Hand capsular volume consistent �Greater ROM correlated with adhesive capsulitis with greater joint volume on arthrogram
HSP- Spasticity related �Older studies (eg Van Ouwenwaller) find that HSP more common in spastic shoulders �More recent study by Huang et al showed a weak correlation between spasticity and HSP �? Role of ultrasound imaging may be to guide needle for EMG into the subscapularis
Neuropathic shoulder pain Hemiplegic Shoulder Pain Update
HSP Neuropathic-CRPS �CRPS type 1= RSD �Shoulder hand syndrome subtype occurs after CVA �Incidence reported as 12 -25% (Edgley SR et al, PM&R Supp 1 March 2009 S 28) �Wide variation due to method of diagnosis (some studies reported much higher incidence with less strcit diagnostic criteria)
Sensitivity and Specificity �A Se. Nsitive test when Negative rules OUT=SNNOUT �A SPecific test when Positive rules IN=SPPIN �Difficult to establish Sensitivity and specificity in studies if there is no “Gold Standard”, or if different “Gold Standards” are used
RSD=CRPS Type 1 � International Association for the Study of Pain (IASP) clinical diagnostic criteria (Revised Budapest criteria) � continuing pain disproportionate to original injury � must have reports of at least 1 symptom in 3 of 4 categories � sensory - allodynia and/or hyperesthesia � vasomotor - temperature asymmetry and/or skin color changes and/or skin color asymmetry � sudomotor/edema - edema and/or sweating changes and/or sweating asymmetry � motor/trophic - decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (in hair, nails, or skin) � must have at least 1 sign at time of evaluation in 2 or more categories � sensory - allodynia (to light touch and/or temperature and/or deep somatic pressure and/or joint movement) and/or hyperalgesia (to pinprick) � vasomotor - evidence of temperature asymmetry (> 1 degree C [1. 8 degrees F]) and/or skin color changes and/or skin color asymmetry � sudomotor/edema -evidence of edema and/or sweating changes and/or sweating asymmetry � motor/trophic - evidence of decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (in hair, nails, or skin) � no other diagnosis can better explain signs or symptoms � sensitivity 0. 85 and specificity 0. 69 � Reference - Pain Med 2007 May-Jun; 8(4): 326, editorial can be found in Pain Med 2007 May. Jun; 8(4): 289, commentary can be found in Pain Med 2009 Apr; 10(3): 598
Bone scan for diagnosis of RSD Review of Hi quality studies � pooled diagnostic performance of bone scintigraphy for CRPS type I in analysis of 21 studies �sensitivity 79% (range 14%-100%) �specificity 88% (range 60%-100%) � criteria for CRPS on triple-phase bone scan included diffusely increased uptake, especially increased periarticular uptake in multiple joints Reference - J Hand Surg Am 2012 Feb; 37(2): 288 Review of Low quality studies � systematic review of 12 diagnostic cohort studies evaluating bone scintigraphy (3 phase scintigraphy in 11 studies, 5 phase scintigraphy in 1 study) for diagnosis of CRPS type I in 882 patients � all studies had ≥ methodologic limitation including � 6 studies lacked valid reference standard for CRPS 1 � unclear if index test interpretation was blinded to reference standard in all studies � pooled diagnostic performance of 3 -phase bone scintigraphy for CRPS type I in analysis of 6 studies with valid reference standard �sensitivity 80% (95% CI 44%-95%) �specificity 73% (95% CI 40%-91%) � positive likelihood ratio 2. 92 (95% CI 1. 33 -6. 43) � negative likelihood ratio 0. 28 (95% CI 0. 1 -0. 76) � Reference - Eur J Pain 2012 Nov; 16(10): 1347
Bone Scan RSD �based on 3 diagnostic cohort studies with inconsistent results all 3 studies had lack of reporting if index test interpretation was blinded to reference standard 116 with suspected CRPS had clinical evaluation and were assessed using 3 -phase bone scintigraphy � 69 (59. 5%) had CRPS using Budapest diagnostic criteria as reference standard �for diagnosis of CRPS, 3 -phase bone scintigraphy had �sensitivity 40% �specificity 76. 5% �positive likelihood ratio 1. 73 �negative likelihood ratio 0. 78 �Reference - Br J Anaesth 2012 Apr; 108(4): 655
Neuropathic (non RSD) HSP etiology Zeilig et al Pain. 2013 Feb; 154(2): 263 -71 � 30 CVA pts N=14 HSP, 16 without HSP> 6 mo post � 15 healthy controls �HSP group had increased parietal involvement �HSP group had higher pain/temp threshold vs CVA pt without HSP in UE and LE �No vasomotor or sudomotor signs (no RSD) �Is HSP part of a central post stroke pain syndrome?
Fig. 3 Higher rates of pathologically evoked pain were found in the affected shoulder of the hemiplegic shoulder pain (HSP) group compared to that of the nonhemiplegic shoulder pain (NHSP) group, including: hyperpathia ( ∗p<. 05, ***p<. 001 Gabi Zeilig , Michal Rivel , Harold Weingarden , Evgeni Gaidoukov , Ruth Defrin Hemiplegic shoulder pain: Evidence of a neuropathic origin PAIN Volume 154, Issue 2 2013 263 - 271 http: //dx. doi. org/10. 1016/j. pain. 2012. 10. 026
Case study- Mr. H � 60 yo M admitted with R hemi due to L PLIC infarct- MMT 3 -/5 L deltoid, biceps, MAS 3 in biceps, no swelling in hand, no sensory change �Shoulder pain started during acute rehab-tx with limb protection, analgesics, diclofenac gel �Pain with abd, arm flex, persisted as outpatient, no relief with subacromial injection
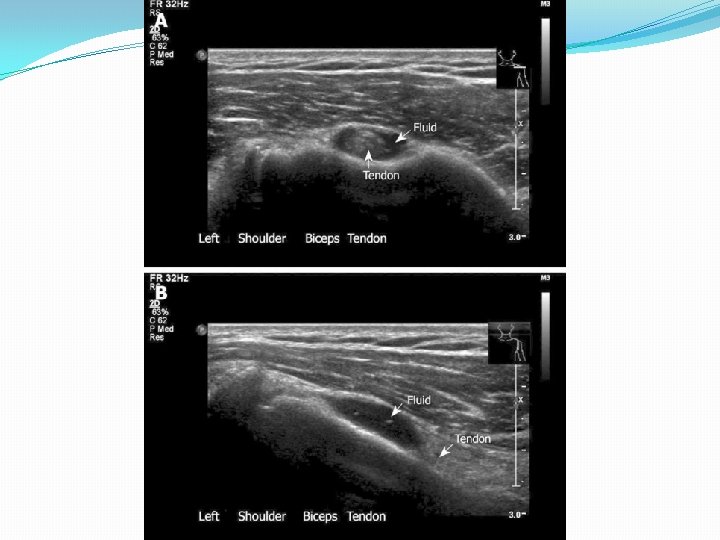
Case study Mr. H �Ultrasound R shoulder- 3 mm fluid surrounding the R biceps tendon in the groove on SAX/LAX views, no cuff abnormalities, AC joint ok �R biceps tendon sheath injection under ultrasound guidance �Resolution of R shoulder pain �Completed outpatient PT/OT- no recurrence �Still gets botox injections to forearm and biceps q 3 months
Case study Mrs. B � 75 yo F with R MCA infarct causing L HP, L neglect, L hemisensory deficits, cognitive def �L shoulder pain, limited ROM, pain with all motions of shoulder, no hand swelling �Completed inpt rehab, d/c to SNF, received additional PT/OT �Outpt clinic f/u continued pain requesting more pain meds (on Oxy IR n SNF)
Case Study Mrs. B �Intra-articular injection of minimal benefit �Pectoralis and biceps botox of helped biceps tone but no improvements with shoulder pain or ROM �Ultrasound of L shoulder-limited study due to problems with positioning shoulder, no evidence of biceps tenosynovitis, + rotator cuff arthropathy (cortical irregularity at supraspinatus insertion) �Multifactorial HSP- adhesive capsulitis, +sensory dysesthesias
Summary HSP �HSP is a complex symptom to evaluate �Some cases (? 50%) are musculoskeletal �RSD about 10 -15% �Sensory dysesthesias may be related to a central post stroke pain syndrome or to more localized spinothalamic involvement (1 -10%) �Multifactorial may account for about 30 -40% of cases and may be the most difficult to eval/tx
HSP Summary �New tools such as MSK ultrasound may improve accuracy of HSP diagnosis �Bicipital tendinopathy/tenosynovitis more common than previously thought �Subscapularis tear more common than previously thought in chronic stage �Improved diagnosis can improve treatment
Hands on Demonstration �Kris Gellert OTR-Hands on Demo of OT eval and treatment of HSP �Anne Kirchmayer MD (FAAPMR Sports and Neuromuscular Med)- MSK US of biceps tendon and subscapularis �Andy Kirsteins MD- MSK of supraspinatus and infraspinatus