Heme metabolism Structure of heme Heme is a

Heme metabolism

• Structure of heme: • Heme is a derivative of porphyrin. Porphyrins are cyclic compound formed by fusion of four pyrrole rings • . An atom of iron is present in the center. • Heme consists of one ferrous (Fe 2+) iron

• Structure of porphyrins • Different porphyrins vary in the nature of the side chains that are attached to each of the pyrrol rings. A = acetate = -CH 2 -COOH P = propionate = -CH 2 -COOH M = methyl = -CH 3 V = vinyl = -CH=CH 2
")
Site: Liver and bone marrow. • Steps: • 1 - Synthesis of d-Aminolevulinate (ALA) in mitochondria by ALA synthase. α ß γ ß + α δ

3 - Condensation of four molecules of porphyrinogen to form uroporphyrinogen III.

4 - Formation of coprophohorinogen III M M M M

5 - Formation of protoporphyrinogen III M V M

6 - Synthesis of protophorphyrin IX
 is the key in • heme synthesis.")
Regulation of heme biosynthesis (ALA synthatase I) is the key in • heme synthesis. 1 - It is inhibited by : a) Heme itself, by feed back inhibition. b) Glucose and steroids. 2 - It is stimulated by: Certain drugs as phenobarbital and iron.

Succinyl-Co. A Glycine Δ-Aminolevulinate synthatase Δ-Aminolevulinate + Phenobarbital Iron - Synthatse Glucose Steroids Heme Control Of Heme Biosynthesis

Porphyria result from 1 - deficiency of enzyme needed for heme synthesis.

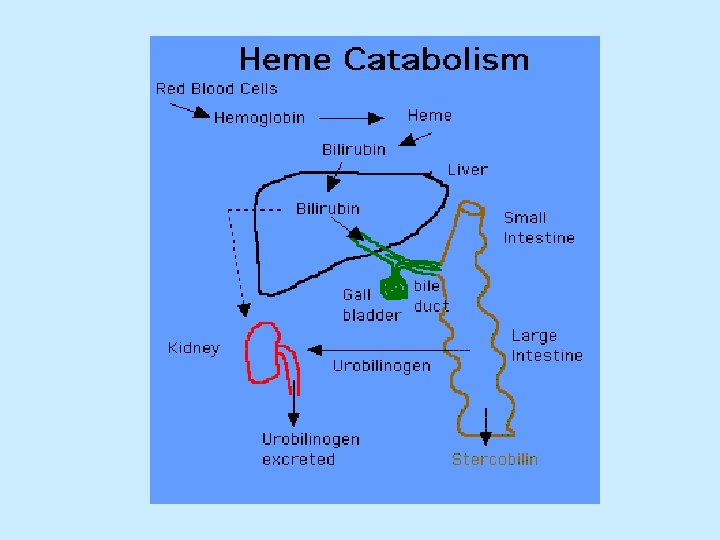
• Catabolism of heme: • After 120 days in the circulation, red blood cells are taken up and degraded by the reticuloendothelial system (RE) particularly in the liver and spleen.
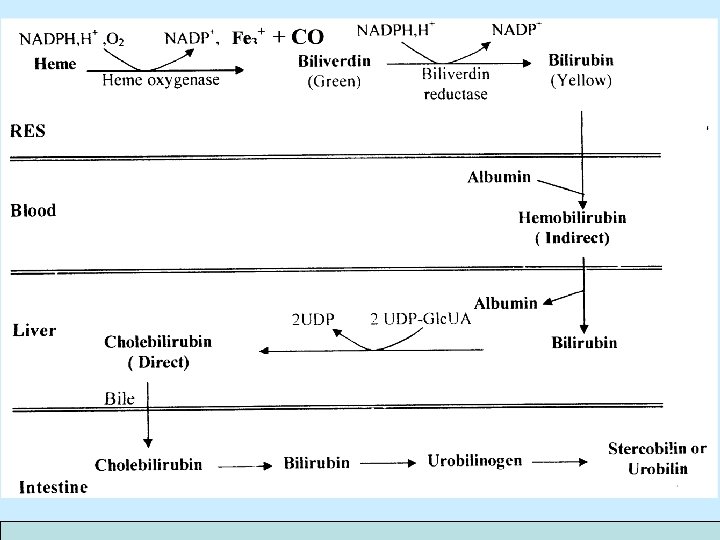

Unconjugated bilirubin Conjugated bilirubin Normally in plasma Normally in bile Attached to albumin Conjugated to glucuronic acid Has high molecular weight and cannot be filtered through the kidney Has small molecular weight and can be filtered through the kidney Can cross BBB in neonates causing brain damage Soluble in plasma and cannot cross brain barrier Give indirect Van den Bergh reaction Gives direct Van den Bergh reaction

Plasma bilirubin • Normally 0. 2 -1. 0 mg/dl • Hyperbilirubinamia : 1 -3 mg/dl • Jaundice : more than 3 mg/dl • Kernictrus : more than 20 mg/dl
 • Pathological 1 - haemolytic jaundice 2 -")
Types of jaundice • Neonatal (physilogic) • Pathological 1 - haemolytic jaundice 2 - hepatic jaundice 3 - obstructive jaundice • Congenital 1 - Gilbert’s disease 2 - Crigler-Najjar syndrome 3 - Dubin-Johnson syndrome
 1 -Causes : Hemolysis of RBC due to favism 2 -")
Prehepatic (Hemolytic jaundice) 1 -Causes : Hemolysis of RBC due to favism 2 - Type of bilirubin increase in blood ↑ unconjucated bilirubin in blood because there are large amount of unconjucated bilirubin come from hemolysis and liver cannot convert this large amount 3 - Urinary change No bilirubin in urine because unconjucated bilirubin is large molecular weight so can not pass through kidney Increase bile pigment as urobilinogen large amount of unconjucated bilirubin converted to bile pigment 4 - Van Den Bergh reaction is indirect
 1 - Causes : Hepatites or chirrosis 2 - Type of")
Hepatic (hepatocellular jaundice) 1 - Causes : Hepatites or chirrosis 2 - Type of bilirubin increase in blood increase unconjucated bilirubin in blood because liver is diseased Increase conjucated bilirubin because edema in bile duct cause partial obstruction 3 -Urinary change Bilirubin in urine because conjucated bilirubin is small molecular weight so can pass through kidney ↑ bile pigment in moderate amount 4 - Van Den Bergh reaction is biphasic
 A- Causes : Stone in bile duct B - Type")
Post hepatic (obstructive jaundice) A- Causes : Stone in bile duct B - Type of bilirubin increase in blood ↑conjucated bilirubin C-Urinary and stool change Urine: Deep brown because conjucated bilirubin ↑ in urine Stool: Clay (white) colour because no bile pigment due to obstruction D- Van Den Bergh reaction is direct

Lab results condition Normal Haemolytic anaemia Hepatitis Obstructive jaundice Serum Urine bilirubin urobilinogen Total 0. 2 - 0 -3 mg/day 1. 0 mg/dl Urine Feacl bilirubin urobilinogen absent 30 -300 mg/day ↑ indirect increased Absent increased ↑ indirect and direct normal present decreased absent Present absent ↑ direct

Causes of Unconjugated hyperbilirubinemia • 1 - Neonatal or physiologic jaundice: Most common cause of jaundice in neonatal age. • Results from increased hemolysis and decrease liver • ability of uptake, conjugate bilirubin. Characterized by high plasma level of unconjugated • bilirubin, if > 20 mg/dl, produce toxic encephalopathy or kernicterus -----> mental retardation. Treated by: 1 - Phenobarbital increase UDP-glucuronyl transferase enzyme. 2 - Phototherapy (exposure to visible light) convert bilirubin to more soluble easily excreted form liver in bile.

3 - Congenital Syndromes related to uptake and conjugation of bilirubin A. Crigler-Najjar Syndrome Decrease in activity of UDP-glucuronyl transferase B. Gilbert Disease Hepatic defect in uptake of bilirubin by liver C- Toxic Hyperbilirubinemia Toxin induced liver dysfunctions as chloroform
- Slides: 23