Hematology Mohamad H Qari MD FRCPA Hematology Cellular












 l Oxygen Transport l l Oxy-hemoglobin")
 l l Margination Phagocytosis The macrophage is")
 White Blood Cell Count l Leukopoiesis l l")
 l Immunity l Subpopulation of lymphocytes known as")


 l Fibrinolysis l l Lysis of clot (plasmin)")



 l l Lymphatic signs Gastrointestinal signs")






 l Sickle cell crises l Vaso-occlusive")






 l Management l Treat the patient similarly to others.")

 l Autoimmune disease l l May be specific")



 l Glycoprotein IIb-IIIa Receptor Inhibitors l G IIb-IIIa = platelet membrane")
 Up to 750 -1500 -2000 >2000")



- Slides: 49
Hematology Mohamad H Qari, MD, FRCPA
Hematology Cellular Components of Blood Red Blood Cells l White Blood Cells l Inflammatory process l Coagulation l Blood Typing Clotting disorders
Hematology Spleen Blood Kidneys Hematopoietic System Bone Marrow Liver
Hematopoeisis Three developmental periods l Mesoblastic l l Hepatic l l Blood islands of yolk sac Primarily RBC production Embryonic hemoglobin produced At 6 weeks cell production in liver Fetal hemoglobin produced Spleen, thymus, lymph nodes also active prod. Myeloid l l l At 5 th month Bone Marrow becomes site of prod. Liver & spleen now Extramedullary Hemoglobin A ( 2 2)
Requirements For Hematopoiesis Stem Cells Growth Factors Microenviroment
Stem Cell theory § § § Pluripotent stem cell originator of all cells Gives rise to cells committed to specific development Research supporting theory PHSC has self-maintaining ability Committed cells differentiate continuously/ No Reverse Flow
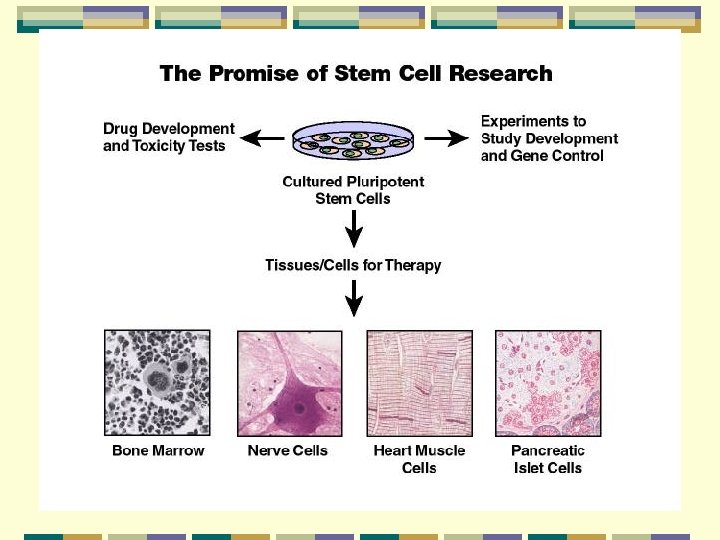
Stem cells in Research Pluripotent cells derived from: l l Cell mass of embryos at blastocyst stage (IVF) Fetal tissue from terminated pregnancy Application l l l Identification of factors of cellular decision-making Development and testing of drugs Generation of cells and tissue for therapy
Cytokines & Growth Factors Cytokines stimulate or inhibit § Prevent apoptosis § Colony-Stimulating Factors produced by many different cells § Interleukins numbered according to discovery §
Components of Blood Plasma l Transport mechanism l l l 90 -92% water. 6 -7% proteins 2 -3% l l l Fats Carbohydrates (glucose) Electrolytes Gases (O 2, CO 2) Chemical messengers
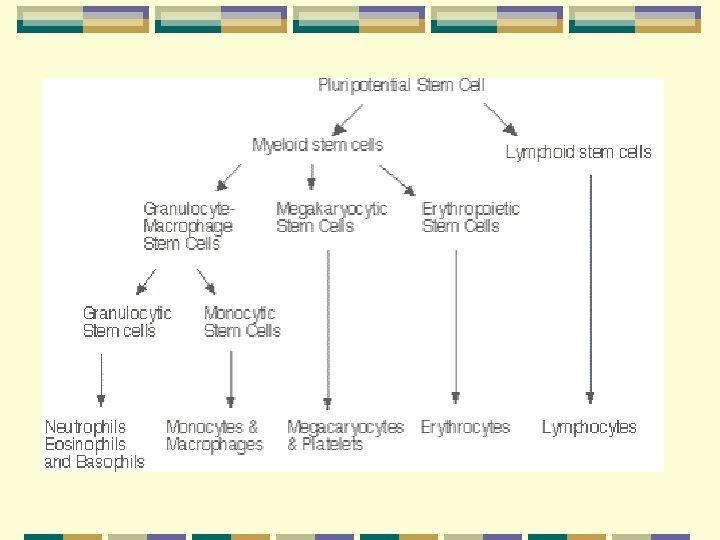
Cellular Components Pluripotent Stem Cell Myeloid Multipotent Stem Cells Common Lymphoid Stem Cells Unipotent Progenitors Lymphocytes WBC’s Basophils Eosinophils Neutrophils Monocytes RBC’s Thrombocytes Platelets Erythrocytes Erythropoietin
Components of Blood Red Blood Cells l Erythrocyte l Hemoglobin – O 2 bearing molecule l l Comprised of 4 subunits: • Globin (binds to 1 O 2 molecule) • Heme (iron) 100% saturation = 4 globin subunits carrying O 2 • Each gram of hemoglobin = 1. 34 ml O 2 Cellsalive. com
Blood Products and Blood Typing Blood Types l Antigens l l A, B, AB, O Rh factor Rh+ = ~85% l Rh- = ~15% l Blood transfusion
Components of Blood Red Blood Cells (cont. ) l Oxygen Transport l l Oxy-hemoglobin dissociation curve 2, 3 -DPG
Components of Blood White Blood Cells (Leukocytes) l l Margination Phagocytosis The macrophage is using its internal cytoskeleton to envelop cells of the fungus Candida albicans.
Components of Blood Leukocytes (cont. ) White Blood Cell Count l Leukopoiesis l l Granulocytes l l l Neutrophil Basophil Eosinophil Monocytes l Lymphocytes l Human Neutrophil: Phagocytosis of Strep pyogenes
Components of Blood Leukocytes (cont. ) l Immunity l Subpopulation of lymphocytes known as T cells and B cells l l T cells develop cellular immunity. B cells produce humoral immunity
Components of Blood Inflammatory Process l l MAST CELLS. l Immunoglobulin E antibody Ig. E, Antigens l l l Antigens stick to the mast cell Ig. E antibodies, causing granules in the mast cell to fire their contents into the surrounding tissue. This releases a host of inflammatory materials - leukotrienes, tumor necrosis factor, interleukin-4 and other cytokines that turn on other inflammatory cells. These materials cause fluid to leak from the capillaries and white cells including neutrophils, T cells and eosinophils to leave the circulation. The end result is a "local inflammatory response", a red, itchy welt. Cellsalive. com
Components of Blood Hemostasis 3 mechanisms l Vascular spasm l l Platelet plug l l Contraction of tunica media Platelet aggregation Coagulation l Formation of fibrin clot
Components of Blood Hemostasis (cont. ) l Fibrinolysis l l Lysis of clot (plasmin) Thrombosis Thrombolytics l Medications affecting clot formation l l Alter the enzyme on the platelet. Affect the coagulation cascade. Enhance clotting.
Coagulation Cascade - Synopsis
This scanning electron micrograph shows the fine structure of a blood clot. Platelets released from the circulation and exposed to the air use fibrinogen from the blood plasma to spin a mesh of fibrin.
General Assessment - Management Focused History and Physical Exam l SAMPLE history l l Hematological disorders are rarely the chief complaint. Physical exam l l Evaluate nervous system function. Skin signs
General Assessment - Management Physical Exam (cont. ) l l Lymphatic signs Gastrointestinal signs l l l Musculoskeletal signs l l l Arthralgia (rheumatoid arthritis) Hemarthrosis Cardiorespiratory signs l l Epistaxis Atraumatic bleeding gums Thrush Atraumatic splenic/hepatic pain Tachycardia, cx pn, dyspnea - CHF Genitourinary signs l l l Hematuria Menorrhagia Infection
Blood Products and Blood Typing - ABO Blood type Antigen present Antibody present on erythrocyte in serum O AB B A None A and B B A Anti-A, Anti-B None Anti-A Anti-B
Blood Products and Blood Typing Compatibility Among ABO Blood Groups Reaction with serum of Recipient Donor Cells AB B A O - + + + - -= no reaction + = reaction
Blood Products and Blood Typing Brady; Paramedic Care Principles and Practice
Diseases of Erythrocytes Anemias l Anemia is a sign, not a separate disease process. l l l Signs and symptoms may not be present until the body is stressed. Differentiate chronic anemia from acute episode. Treat signs and symptoms. l l Maximize oxygenation and limit blood loss. Establish IV therapy if indicated.
Diseases of Erythrocytes Brady; Paramedic Care Principles and Practice
Diseases of Erythrocytes Sickle Cell Disease l Normal red cells maintain their shape as they pass through the capillaries and release oxygen to the peripheral tissues (upper panel). Hemoglobin polymers form in the sickle rell cells with oxygen release, causing them to deform. The deformed cells block the flow of cells and interrupt the delivery of oxygen to the tissues (lower panel).
Diseases of Erythrocytes Sickle Cell Disease (cont. ) l Sickle cell crises l Vaso-occlusive l l Hematological l l Musculoskeletal/abdominal pain Priapism Renal/cerebral infarctions Lowered hemoglobin Splenic sequestration Infectious Management l l Follow general treatment guidelines prn. Consider analgesics.
Diseases of Erythrocytes Polycythemia l Overproduction of erythrocytes. Occurs in patients > 50 years old or with secondary dehydration. l Most deaths due to thrombosis l l Results in bleeding abnormalities: l l Epistaxis, spontaneous bruising, GI bleeding. Management: l Follow general treatment guidelines.
Diseases of Leukocytes Leukopenia/Neutropenia Too few white blood cells or neutrophils. l Follow general treatment guidelines and provide supportive care. l Leukocytosis l An increase in the number of circulating white blood cells, often due to infection. l Leukemoid reaction
Diseases of Leukocytes Leukemia Cancer of hematopoietic cells l Initial presentation l Acutely ill, fatigued, febrile and weak, anemic. l Thrombocytopenia l Often have a secondary infection. l l Management Follow general treatment guidelines. l Utilize isolation techniques to limit risk of infection. l
Diseases of Leukocytes Lymphomas l Cancers of the lymphatic system l l l Presentation l l l Hodgkin's Non-Hodgkins Swelling of the lymph nodes Fever, night sweats, anorexia, weight loss, fatigue, and pruritis Management l l Follow general treatment guidelines. Utilize isolation techniques to limit risk of infection.
Clotting Disorders Thrombocytosis and Thrombocytopenia l Thrombocytosis l l An abnormal increase in the number of platelets Thrombocytopenia l An abnormal decrease in the number of platelets l l Sequestration Destruction (ITP) Decreased production Management l Provide supportive care and follow general treatment guidelines.
Clotting Disorders Hemophilia l Deficiency or absence of a blood clotting factor l l l Deficiency of factor VIII causes hemophilia A. Deficiency of factor IX causes hemophilia B. Deficiency is a sex-linked, inherited disorder. l l Defective gene is carried on the X chromosome. Signs & Symptoms l Numerous bruises, deep muscle bleeding, and joint bleeding.
Clotting Disorders Hemophilia (cont. ) l Management l Treat the patient similarly to others. l l l Administer supplemental oxygen. Establish IV access. Be alert for recurrent or prolonged bleeding, and prevent additional trauma. Von Willebrand’s Disease l Deficient component of factor VIII l l Generally results in excessive bleeding. Generally is not serious; provide supportive care.
Clotting Disorders Disseminated Intravascular Coagulation
Components of Blood Leukocytes (cont. ) l Autoimmune disease l l May be specific or general Alterations in the immune process l Immunosuppression l l HIV Anti-rejection medication Chemotherapy/Cancer System activation of coagulation cascade.
Anticoagulants/Antiplatelets Classifying agents l Anticoagulants l l Antiplatelets l l Block synthesis and activation of clotting factors Interfere with platelet aggregation or activation Fibrinolytics l Dissolve fibrin component of thrombi
Anticoagulants/Antiplatelets Anticoagulants l Warfarin l l l Unfractionated Heparin l l l Blocks activation of Vit K Interferes w/ coagulation factors II, VII, IX, and X Binds antithrombin III (AT-III) Inhibits coagulation factors IX and thrombin Hirudin (medicinal leech) l Prevents thrombin binding
Anticoagulants/Antiplatelets l Aspirin l Prevents platelet activation through cyclooxygenase blockade. l l l Prevents production of thromboxane A 2 Allows prostacyclin synthesis Ticlodipine l Deforms platelet membrane fibrinogen receptor
Anticoagulants/Antiplatelets (cont. ) l Glycoprotein IIb-IIIa Receptor Inhibitors l G IIb-IIIa = platelet membrane receptor of fibrinogen l l l Abciximab Eptifibatide Tirofiban Fibrinolytics l Activate plasminogen to plasmin = fibrinolysis l l l Streptokinase Anistreplase Tissue Plasminogen Activator Reteplase Urokinase
Hemorrhage Class III Class IV Blood Loss (ml) Up to 750 -1500 -2000 >2000 Blood Loss (% volume) Up to 15%-30% 30%-40% >40% Pulse <100 >120 >140 BP Normal Decreased Pulse Pressure Normal or increased Decreased Resp. Rate 14 -20 20 -30 30 -40 >35 Urine Output (ml/hr) >30 20 -30 5 -15 Negligible Mental Status Slightly anxious Mildly anxious Anxious, confused Confused, lethargic Fluid Replacement (3: 1) rule Crystalloid and blood
Transfusion Reactions Hemolytic Reaction l Signs & Symptoms l l Facial flushing, hyperventilation, tachycardia, hives, chest pain, wheezing, fever, chills, and cyanosis Treatment l l Stop transfusion, change all IV tubing, and initiate IV therapy with normal saline or lactated Ringer’s. Consider furosemide, dopamine, and diphenhydramine.
Transfusion Reactions Febrile Non-hemolytic Reactions l Signs & Symptoms l l Headache, fever, and chills Treatment Stop transfusion, change all IV tubing, and initiate IV therapy with normal saline or lactated Ringer’s. l Consider Diphenhydramine and an antipyretic. l Observe closely to ensure reaction is nonhemolytic. l